
A 2026 systematic review and meta-analysis of randomized trials found no broad superiority for phase-based complex PTSD care across most outcomes. Affect dysregulation was the clearest exception, improving more when treatment was phase-based, multi-phase, and exposure-containing.
Research Highlights
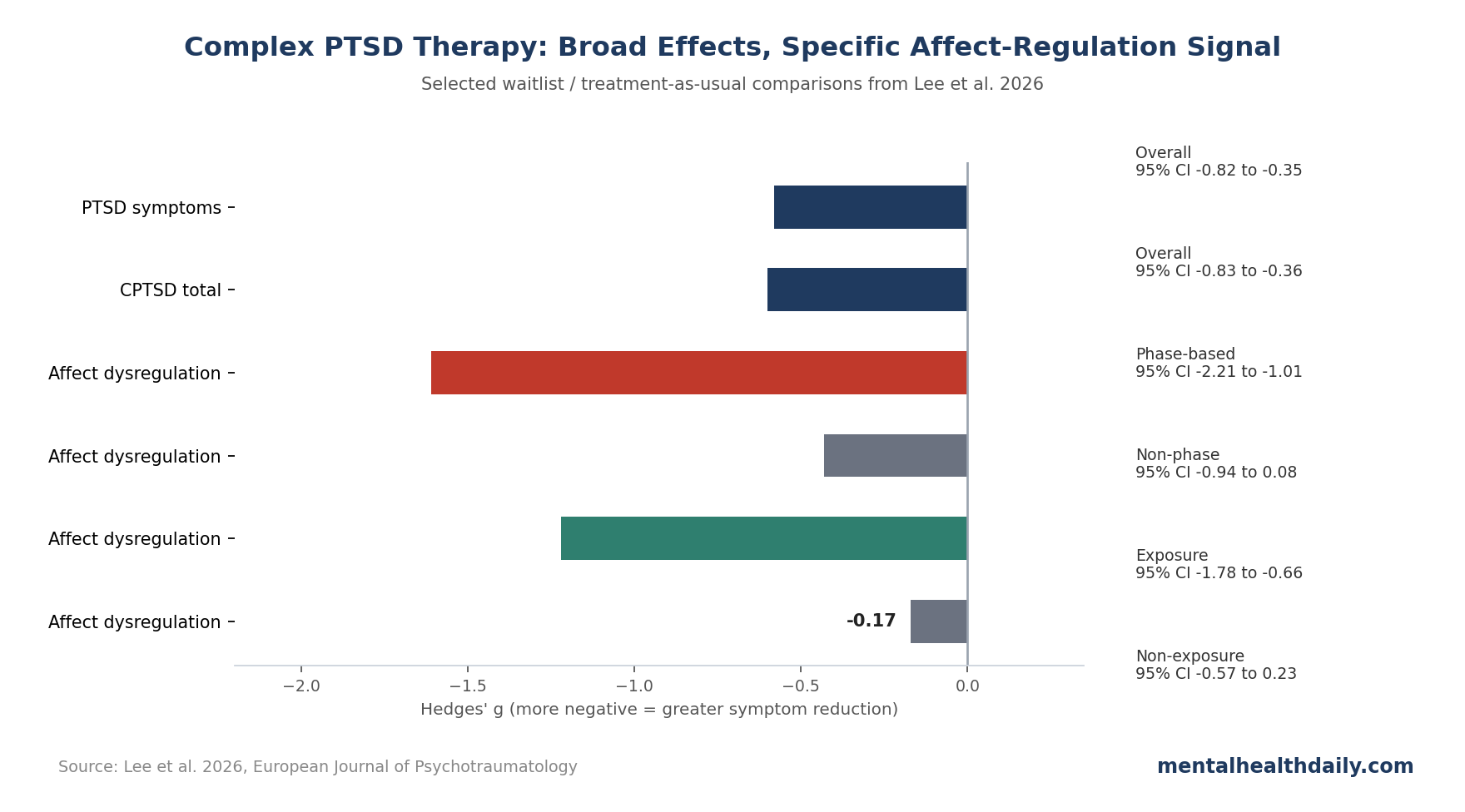
- Most therapy formats helped: across waitlist and treatment-as-usual comparisons, psychological interventions reduced PTSD symptoms (k = 9; Hedges’ g = −0.58; 95% CI −0.82 to −0.35) and total complex PTSD symptoms (k = 7; g = −0.60; 95% CI −0.83 to −0.36).
- Phase-based care did not dominate globally: phase-based and non-phase-based interventions did not significantly differ for total CPTSD (Q = 0.05; p = 0.82), relationship disturbance (Q = 2.28; p = 0.13), or head-to-head PTSD comparisons.
- Affect regulation was the exception: phase-based therapy beat non-phase-based therapy on affect dysregulation (g = −1.61; 95% CI −2.21 to −1.01 vs. g = −0.43; 95% CI −0.94 to 0.08; subgroup p < 0.01).
- Multi-phase treatment had a PTSD advantage: multi-phase interventions reduced PTSD symptoms more than single-phase interventions (g = −0.70 vs. −0.15; subgroup p = 0.04).
- Evidence remains thin: only 16 randomized studies met inclusion criteria, and follow-up analyses were not feasible because too few studies reported comparable longer-term data.
Care should stay flexible. Many trauma-focused and non-exposure approaches can help complex PTSD, but patients whose main barrier is affect dysregulation may benefit from a structured sequence that builds regulation skills before deeper trauma processing.
Complex post-traumatic stress disorder (CPTSD) in the International Classification of Diseases, 11th revision (ICD-11), includes core PTSD symptoms plus disturbances in self-organization (DSO): affect dysregulation, negative self-concept, and relational disturbance. This broader symptom profile is why the treatment debate exists in the first place.
16 Randomized Trials Focused on CPTSD Symptom Domains
Lee et al. searched the Cochrane Library, Embase, Medline, PTSDpubs, Scopus, Web of Science, and South Korean databases on June 17, 2025. Researchers identified 1,642 records, removed 503 duplicates, screened 292 full texts, and included 16 randomized controlled trials.
- Population filter: clinically significant CPTSD symptoms, or PTSD plus at least 2 disturbances in self-organization (DSO) symptom clusters.
- Comparison filter: phase-based vs. non-phase-based care, multi-phase vs. single-phase care, and exposure-containing vs. non-exposure care.
- Main limitation from the start: subgroup cells were small, so non-significant differences should be read as unresolved, not proven equal.
Eligibility criteria were deliberately CPTSD-focused. Studies needed clinically significant CPTSD symptoms or PTSD plus at least 2 DSO symptom clusters. Six studies used the International Trauma Questionnaire (ITQ), which maps directly onto ICD-11 CPTSD criteria, while older studies used measures such as the Structured Interview for Disorders of Extreme Stress (SIDES) or proxy DSO measures.
Included therapies were not one uniform package. Six studies included Skills Training in Affective and Interpersonal Regulation (STAIR) or a modified STAIR arm; 3 included prolonged exposure; 2 included imagery rescripting. Other approaches included eye movement desensitization and reprocessing (EMDR), trauma-focused cognitive behavioral therapy, emotion-focused therapy, acceptance and commitment therapy, body-oriented group therapy, stabilization therapy, mindfulness-based therapy, problem management, cognitive narrative therapy, and trauma-focused group music and imagery therapy.
Interpretation: this variety better reflects real CPTSD care, where patients are rarely assigned to a single purified psychotherapy ingredient. It also means subgroup comparisons are underpowered and sensitive to how interventions were classified.
PTSD and Total CPTSD Improved Without a Clear Phase-Based Winner
Compared with waitlist or treatment as usual, psychological interventions produced moderate-to-large symptom reductions. In Hedges’ g terms, effects around 0.5–0.8 usually mean a visible clinical signal, not a tiny statistical blip.
- PTSD symptoms improved: g = −0.58 (95% CI −0.82 to −0.35) across 9 studies, with low heterogeneity (I2 = 23.55%).
- Total CPTSD symptoms improved: g = −0.60 (95% CI −0.83 to −0.36) across 7 studies, again with low heterogeneity (I2 = 17.25%).
- Phase-based care looked numerically stronger for PTSD: g = −0.94 vs. −0.50 for non-phase-based care, but the subgroup difference was not statistically significant (Q = 1.68; p = 0.20).
- Total CPTSD did not separate by phase model: phase-based care (g = −0.80; 95% CI −1.87 to 0.27) and non-phase-based care (g = −0.67; 95% CI −0.93 to −0.41) did not significantly differ (Q = 0.05; p = 0.82).
Head-to-head interpretation: direct comparisons were flatter than waitlist comparisons. PTSD measured with the Clinician-Administered PTSD Scale had g = 0.04 (95% CI −0.23 to 0.31), and combined PTSD Checklist / CAPS outcomes had g = 0.03 (95% CI −0.22 to 0.28). Those estimates are close to zero, meaning the active therapy formats looked similar in the limited direct-comparison evidence.
Affect Dysregulation Was Where Sequencing Looked Most Useful
Affect dysregulation means emotional flooding, shutdown, unstable arousal, anger surges, dissociation-linked disengagement, and difficulty returning to baseline after threat cues. In the DSO-affect dysregulation analysis, all interventions combined produced a large effect (k = 7; g = −0.89; 95% CI −1.47 to −0.31), but heterogeneity was considerable (I2 = 78.47%).
- Phase-based vs. non-phase: phase-based interventions produced g = −1.61 (95% CI −2.21 to −1.01), compared with g = −0.43 (95% CI −0.94 to 0.08) for non-phase-based interventions; subgroup p < 0.01.
- Multi-phase vs. single-phase: multi-phase interventions outperformed single-phase interventions for affect dysregulation (g = −1.19 vs. −0.10; p = 0.01).
- Exposure vs. non-exposure: exposure-containing interventions showed a larger effect (g = −1.22; 95% CI −1.78 to −0.66) than non-exposure interventions (g = −0.17; 95% CI −0.57 to 0.23; p < 0.01).
Interpretation: sequencing and treatment ingredients separated most clearly for affect regulation. The strongest affect-regulation signal appeared when therapy included both structure and trauma processing, while patient fit still determines whether exposure should start early or follow stabilization.
Multi-Phase Treatment Beat Single-Phase Treatment for PTSD Symptoms
Another significant subgroup finding involved PTSD symptom reduction. Multi-phase interventions produced a larger PTSD effect (k = 6; g = −0.70; 95% CI −0.93 to −0.48) than single-phase interventions (k = 3; g = −0.15; 95% CI −0.62 to 0.33), with Q = 4.28 and p = 0.04.
Meaning: multi-component care looked better for PTSD symptoms, while the data still leave room for early exposure when a patient can tolerate it. Lee et al. separated 3 overlapping ideas: whether treatment was phase-based, whether it had multiple phases, and whether it included exposure. Those constructs are related, but they are not interchangeable.
For care planning, a patient may need emotion regulation skills, sleep stabilization, substance-use support, or crisis planning before trauma work is tolerable. Another patient may be ready for trauma-focused therapy without months of preliminary work. Evidence does not support a rigid bottleneck that delays exposure for everyone with CPTSD.
Relationship Symptoms and Negative Self-Concept Remain Less Settled
Disturbances in relationships improved overall, with g = −0.72 (95% CI −0.97 to −0.47) across 6 studies and I2 = 0.00%. Phase-based interventions were numerically stronger (g = −1.18; 95% CI −1.87 to −0.48) than non-phase-based interventions (g = −0.60; 95% CI −0.89 to −0.31), but the subgroup difference was not significant (Q = 2.28; p = 0.13).
Negative self-concept had too little data for serious subgroup interpretation. Pooled effect was moderate-to-large (k = 2; g = −0.69; 95% CI −1.03 to −0.36), with I2 = 0.00%, but only 2 studies contributed. This is a signal to measure this domain better, not a reason to declare that shame, guilt, and self-worth reliably respond to one particular sequencing model.
Prior construct work helps explain why these domains may not move together. Cloitre et al. argued for separating PTSD symptoms from DSO clusters, and Huynh et al. later estimated global CPTSD prevalence at 6.2%. Chong et al. linked CPTSD to suicidality beyond PTSD in adults with childhood maltreatment. CPTSD is clinically coherent, but its components are not one symptom blob.
CPTSD Treatment Should Be Matched to the Patient’s Bottleneck
Evidence points toward a practical sorting principle:
- If re-experiencing and avoidance dominate: trauma-focused work such as prolonged exposure, EMDR, cognitive processing therapy, or trauma-focused cognitive behavioral therapy may be appropriate without requiring a long stabilization detour.
- If affect dysregulation blocks engagement: phase-based or multi-phase care that starts with regulation skills may fit better, especially when dissociation, emotional flooding, impulsivity, self-harm risk, or rapid dropout risk are central.
- If relational disturbance or negative self-concept dominates: the evidence is thinner, so therapy may need more explicit interpersonal, shame-focused, and identity-focused work because trauma exposure alone may not generalize.
Rigid ideology fails on both sides. Immediate exposure for every CPTSD patient can be reckless when someone cannot stay emotionally engaged enough to process trauma safely. Endless stabilization can also become avoidance dressed up as prudence. The treatment phase should remove the patient’s actual bottleneck.
Limitations of the Lee Meta-Analysis
Trial count was small. Only 16 randomized studies met inclusion criteria, and several subgroup cells contained only 2 or 3 studies. A non-significant subgroup test in this setting leaves equivalence unresolved.
CPTSD measurement was mixed. Six studies used the ITQ, but others relied on SIDES or proxy measures. Lee et al. also required only 2 DSO symptom clusters for eligibility, so some samples may not fully match ICD-11 CPTSD.
Follow-up effects were not analyzable. The review focused on pre-to-post effects because too few studies reported comparable follow-up time points. A therapy can look similar at post-treatment and diverge months later; this analysis could not answer that durability question.
Psychotherapy blinding is inherently limited. About 30% of studies were rated high risk in deviations from intended interventions, mainly because strict blinding is not realistic in psychotherapy trials. Half had some concerns in selective reporting, and 12.5% were high risk in that domain, largely from lack of registration.
Questions About Phase-Based Therapy for Complex PTSD
Does every person with complex PTSD need stabilization before trauma exposure?
No. This 2026 meta-analysis did not find broad evidence that phase-based therapy outperformed non-phase-based therapy across most outcomes.
Stabilization still fits patients whose affect dysregulation, dissociation, crisis behavior, or dropout risk would make trauma work poorly tolerated.
Did exposure therapy look harmful for complex PTSD?
No. Exposure-containing interventions improved PTSD, total CPTSD, and affect dysregulation outcomes in the pooled analyses. Exposure is not forbidden; timing, preparation, and patient fit are the practical questions.
What symptom domain most favored phase-based care?
Affect dysregulation. Phase-based, multi-phase, and exposure-containing interventions all showed larger effects on affect dysregulation than their comparison groups.
What should future trials measure?
Trials need clearer ICD-11 CPTSD assessment, separate DSO domains, longer follow-up, dropout and adverse-event reporting, and direct comparisons that isolate sequencing from broad therapy bundles.
Bottom line: broad symptom improvement occurred across multiple complex PTSD therapy formats. Affect dysregulation was the clearest reason to favor structured, multi-phase treatment that prepares patients for trauma processing.
References
- Lee Y, Park S, Cho Y-E. Phase-based versus non-phase-based psychological interventions for complex PTSD: a systematic review and meta-analysis. European Journal of Psychotraumatology. 2026;17:2644112. doi:10.1080/20008066.2026.2644112
- Bohus M, Kleindienst N, Hahn C, et al. Dialectical behavior therapy for posttraumatic stress disorder compared with cognitive processing therapy in complex presentations of PTSD in women survivors of childhood abuse: a randomized clinical trial. JAMA Psychiatry. 2020;77:1235–1245. doi:10.1001/jamapsychiatry.2020.2148
- Cloitre M, Stovall-McClough KC, Nooner K, et al. Treatment for PTSD related to childhood abuse: a randomized controlled trial. American Journal of Psychiatry. 2010;167:915–924. doi:10.1176/appi.ajp.2010.09081247
- Karatzias T, Murphy P, Cloitre M, et al. Psychological interventions for ICD-11 complex PTSD symptoms: systematic review and meta-analysis. Psychological Medicine. 2019;49:1761–1775. doi:doi:10.1017/s0033291719000436
- McLean CP, Levy HC, Miller ML, Tolin DF. Exposure therapy for PTSD: A meta-analysis. Clinical Psychology Review. 2022;91:102115. doi:10.1016/j.cpr.2021.102115
- Huynh PA, Kindred R, Perrins K, et al. Prevalence of complex post-traumatic stress disorder: a systematic review and meta-analysis. Psychiatry Research. 2025;351:116586. doi:10.1016/j.psychres.2025.116586
- Chong D, Qu D, Xi Y, Chen R. Complex post-traumatic stress disorder is uniquely linked to suicidality beyond posttraumatic stress disorder in adults with childhood maltreatment: a multinational study across 4 countries. Social Science & Medicine. 2024;362:117406. doi:10.1016/j.socscimed.2024.117406