A 2026 community study of 101 older adults found that pulse-wave harmonics changed in a more organized way during a subtraction task in cognitively intact participants than in people with MoCA-defined mild cognitive impairment: amplitude-coherence scores averaged 9.00 vs. 6.40, a 2.60-point gap on a 0-10 scale.
Research Highlights
- Cognitive stress exposed the signal: resting pulse harmonics showed only weak clinical correlations, but the subtraction task separated 10 reference participants from 45 MCI participants by response organization.
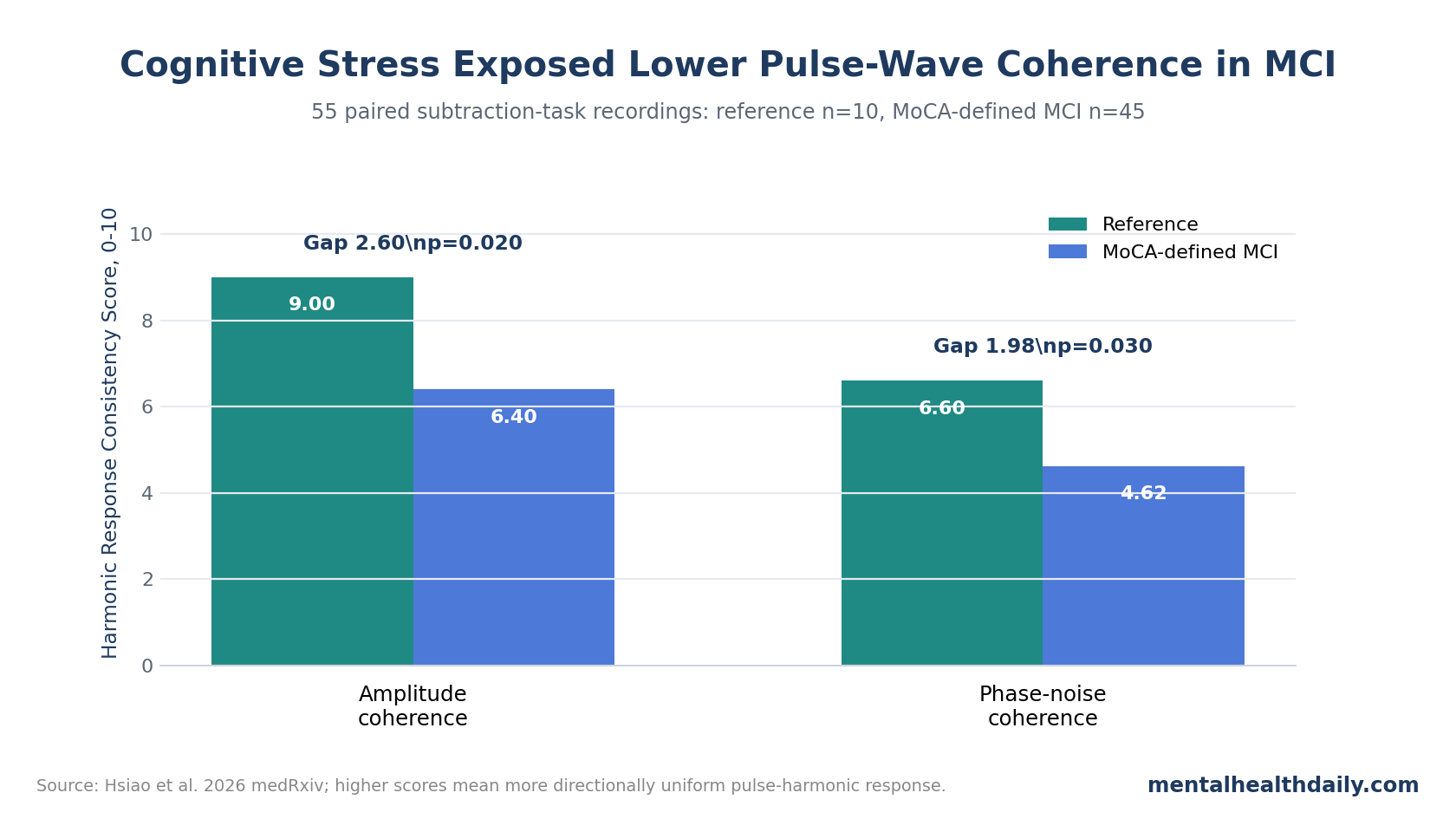
- Amplitude coherence was lower in MCI: the reference group averaged 9.00 vs. 6.40 in the MCI group, with a mean difference of 2.60 points (95% CI 0.29-4.91; p = 0.020).
- Phase-noise coherence also separated groups: reference participants averaged 6.60 vs. 4.62 in the MCI group (mean difference 1.98; 95% CI 0.04-3.92; p = 0.030).
- The sample was screening-defined: MoCA scores sorted 12 people into the reference group, 50 into MCI, and 39 into dementia-level impairment; only 55 had usable paired task recordings.
- The finding is exploratory: this was a 2026 medRxiv preprint with a 10-person reference task sample, so the result fits biomarker-development logic rather than clinical-diagnosis logic.
Pulse-wave harmonic analysis breaks the wrist pulse waveform into frequency components, then asks whether those components change in an organized way. In this study, the important feature was not a single pulse value; it was whether 10 harmonic orders moved together after cognitive demand.
Harmonic Response Consistency Score (HRCS) was the study’s summary measure for that organization. A score near 10 meant the harmonic components changed in the same direction after the task; a score near 0 meant the response was scattered across components.
Cognitive Stress Revealed a Pattern That Resting Pulse Measures Missed
Hsiao et al. studied community-dwelling older adults in southern Taiwan and classified them by Montreal Cognitive Assessment (MoCA) scores, a brief cognitive screening test often used to flag possible mild cognitive impairment or dementia-level impairment. The full cohort included 101 people: 12 with MoCA scores of 26 or higher, 50 with scores from 18 to 25, and 39 with scores below 18.
The dementia-level group could not complete the subtraction-task analysis, and some recordings failed quality control. The main task-evoked comparison therefore used 55 paired recordings: 10 reference participants and 45 participants in the MoCA-defined MCI stratum.
Static pulse-cognition links were modest: baseline pulse harmonics correlated weakly with clinical variables. Lower-order harmonic amplitudes C1-C3 correlated with systolic blood pressure (r = -0.218 to -0.250; p = 0.032 to 0.016), while P1 correlated with depressive symptoms on the BDI (r = 0.244; p = 0.018) and P6 correlated with AD8 cognitive-change scores (r = 0.216; p = 0.037). Most other correlations were small or nonsignificant.
That pattern matters for interpretation because resting pulse features did not behave like a clean cognitive screen. They looked more like vascular-regulatory state markers, which is exactly why the cognitive task became the sharper test.
The cohort also carried the kind of background physiology that can blur a simple biomarker story. Chronic cardiometabolic conditions were common, and cognitive strata differed on several non-cognitive variables: mean age rose from 74.75 years in the reference group to 78.26 years in the MCI group and 83.56 years in the dementia-level group; education also shifted strongly across strata. Systolic and diastolic blood pressure differed by group as well.
Those imbalances do not erase the task result, because the HRCS comparison used within-person pre-post change rather than a single resting pulse snapshot. They do mean the signal should be read as stress-response physiology in a community screening sample, not as a clean brain-only marker of mild cognitive impairment.
MCI Had Lower Pulse-Wave Coherence During the Subtraction Task
The subtraction task produced small average pre-post changes in individual harmonics. In the reference group, harmonic amplitudes generally decreased after the task, but no individual pre-post comparison reached statistical significance. In the MCI group, average changes stayed close to zero and pointed in mixed directions.
HRCS changed the readout from single-feature magnitude to whole-response organization. The reference group showed a high amplitude-coherence score of 9.00 ± 2.16, while the MCI group averaged 6.40 ± 3.48. The between-group difference was significant by Mann-Whitney U testing (U = 326.50; p = 0.020), with a 2.60-point mean gap and a 95% CI from 0.29 to 4.91.
Phase-noise coherence moved in the same direction. Reference participants averaged 6.60 ± 2.68 vs. 4.62 ± 2.79 in the MCI group (U = 322.50; p = 0.030), with a 1.98-point mean difference and a 95% CI from 0.04 to 3.92. Independent-samples t-tests gave the same broad result for amplitude coherence (p = 0.028) and phase-noise coherence (p = 0.046).
Non-significant domains: phase-angle consistency and variability consistency did not differ significantly between groups. The result is therefore narrower than “pulse harmonics diagnose MCI”: 2 coherence domains separated the groups, while 2 did not.
Why Autonomic-Cognitive Coupling Is a Plausible MCI Signal
The finding fits a broader literature linking cognition with autonomic regulation, the body’s automatic control of heart rate, blood-vessel tone, breathing-linked rhythms, and stress-response physiology. Forte et al. reviewed heart-rate variability and cognition and found that autonomic measures repeatedly tracked cognitive performance, especially domains such as attention and executive control that depend on flexible regulation.
Pavlov et al. added a task-level piece: pulse-wave amplitude changed during working-memory load, supporting the idea that peripheral vascular responses can track cognitive effort over short time windows. Hsiao et al. extended that logic from cognitive load in general to cognitive aging, asking whether a simple stressor could reveal loss of organized cardiovascular response in older adults with lower MoCA scores.
Longitudinal MCI and dementia studies make the same direction biologically credible. Nicolini et al. reported that autonomic function predicted cognitive decline in mild cognitive impairment, while Chou et al. linked autonomic modulation in a middle-aged cohort to dementia risk over 17 years. Those studies do not validate HRCS specifically, but they support the larger claim that autonomic-cognitive coupling is more than a side observation.
The mechanism is plausible but not pinned down. Serial subtraction is supposed to recruit working memory and executive control, which in turn engage prefrontal and anterior cingulate regions connected to the central autonomic network. That network helps coordinate vagal and sympathetic output to the heart and blood vessels. In a healthy response, mental arithmetic can produce a short sympathetic shift, peripheral vasoconstriction, arterial stiffening, and a pulse-wave shape change.
Hsiao et al. inferred that intact cognition preserved a more coordinated version of that chain, while MoCA-defined MCI fragmented it across harmonic orders.
Missing pathway measurements limit the mechanism claim. The study did not directly record simultaneous heart-rate variability, beat-to-beat blood pressure reactivity, or neural activation during the task, so HRCS remains a downstream pulse-pattern marker rather than proof of a specific autonomic pathway.
The Screening Claim Needs Calibration
This study is best read as a biomarker-development result. It says a cognitive challenge may expose cardiovascular response coherence that resting measures miss. It does not say wrist-pulse harmonics can diagnose MCI, replace neuropsychological testing, or predict conversion to dementia.
The strongest version of the claim is narrower and more useful: a brief cognitive perturbation may reveal loss of coordinated cardiovascular regulation before resting pulse features look informative. That is a screening-development hypothesis. It becomes clinically meaningful only if future studies show that HRCS adds measurable accuracy beyond MoCA, age, education, vascular risk, mood symptoms, informant reports, and ordinary blood-pressure data.
- Diagnosis: cognitive status came from MoCA strata, not a full clinical adjudication of MCI or dementia.
- Sample size: the task-evoked reference group had only 10 usable paired recordings, so the comparison is sensitive to sampling noise.
- Mechanism: the researchers did not simultaneously record heart-rate variability, task blood-pressure reactivity, or other autonomic markers during the subtraction task.
- Publication status: the article was a medRxiv preprint at intake, so peer review had not yet tested the analysis.
The useful clinical direction is triage research: pair a low-burden physiological recording with a brief cognitive stressor, then test whether response coherence improves screening accuracy when added to MoCA, informant reports, vascular-risk data, and longitudinal follow-up.
Questions About Pulse-Wave Harmonics and MCI
Could pulse-wave harmonics become a dementia screening tool?
Possibly, but this study is an early signal. A screening tool would need larger samples, blinded clinical diagnoses, test-retest reliability, device-standardization work, and evidence that the pulse metric adds accuracy beyond MoCA and ordinary risk factors.
Why use a subtraction task instead of resting pulse data?
Resting pulse features mostly tracked vascular-regulatory state and had weak cognitive correlations. The subtraction task challenged the cardiovascular-autonomic system, making response organization easier to see.
Was the MCI group sicker overall?
The MoCA strata differed by age, education, blood pressure, AD8, anxiety, and depressive-symptom scores. Those differences are part of the reason the result needs prospective validation rather than immediate diagnostic use.
What would make the finding stronger?
A stronger study would enroll a larger reference group, confirm clinical MCI status, repeat the task across sessions, include concurrent heart-rate and blood-pressure reactivity, and test whether HRCS predicts future cognitive decline.
References
- Hsiao K-Y. Pulse-wave harmonic signatures of cardiovascular regulatory coherence to a cognitive challenge in mild cognitive impairment: a community-based cross-sectional study. medRxiv. 2026. doi:10.64898/2026.04.24.26351647
- Forte G, Favieri F, Casagrande M. Heart rate variability and cognitive function: a systematic review. Frontiers in Neuroscience. 2019;13:710. doi:10.3389/fnins.2019.00710
- Pavlov YG, Gashkova AS, Kasanov D, Kosachenko AI, Kotyusov AI, Kotchoubey B. Task-evoked pulse wave amplitude tracks cognitive load. Scientific Reports. 2023;13:22592. doi:10.1038/s41598-023-48917-5
- Nicolini P, Lucchi T, Abbate C, Inglese S, Tomasini E, Mari D, et al. Autonomic function predicts cognitive decline in mild cognitive impairment: evidence from power spectral analysis of heart rate variability in a longitudinal study. Frontiers in Aging Neuroscience. 2022;14:886023. doi:10.3389/fnagi.2022.886023
- Chou Y-T, Sun Z-J, Shao S-C, Yang Y-C, Lu F-H, Chang C-J, et al. Autonomic modulation and the risk of dementia in a middle-aged cohort: a 17-year follow-up study. Biomedical Journal. 2023;46(6):100576. doi:10.1016/j.bj.2022.12.004
- Hsiao K-Y, Kang J-H, Wu Y-S, Chang H-H, Yang C-T. Peripheral pulse harmonic analysis and its clinical application: a systematic review. Journal of Traditional and Complementary Medicine. 2024;14(2):223-236. doi:10.1016/j.jtcme.2023.11.006