
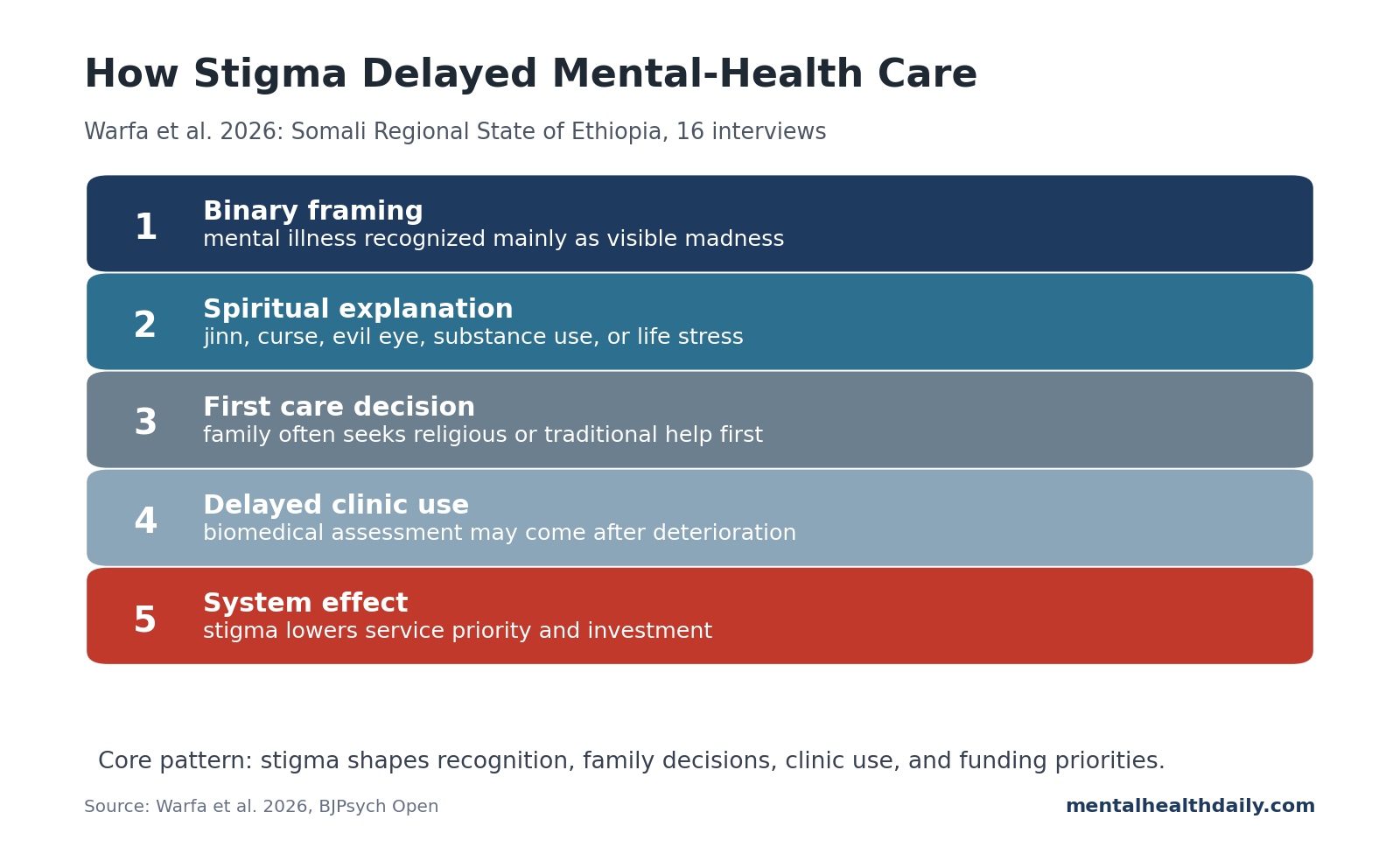
A 2026 qualitative study from Ethiopia’s Somali Regional State found a harsh care-seeking pattern: mental illness was often recognized only when it looked like visible “madness,” was commonly explained through spiritual causes, and carried stigma severe enough to delay biomedical care.1
Research Highlights
- 16 interviews shaped the analysis: Warfa et al. interviewed health workers, service users, carers, and local stakeholders in Jigjiga and Kabridahar between April and July 2024.1
- Mental illness was often framed as binary: participants described local views in which a person was either “mad” or sane, leaving depression, anxiety, PTSD, and milder illness poorly recognized.1
- Spiritual explanations drove care pathways: jinn, curses, evil eye, khat, alcohol, and life stress appeared in explanations, with religious or traditional care often sought before biomedical care.1
- Stigma affected people and services: participants described concealment, isolation, abuse, employment exclusion, marriage barriers, and underinvestment in mental health services.1
- Stigma and service access moved together: mental-health expansion in the region has to address stigma, local explanatory models, clinics, and medication access together.1
Because the research was qualitative, it investigated care-seeking mechanisms rather than prevalence: how stigma, explanatory models, family decision-making, and limited services combined to delay care.
16 Somali Region Interviews Mapped Stigma and Care-Seeking
Warfa et al. conducted semi-structured interviews with 16 adults who had experience providing, using, or supporting mental health care in Ethiopia’s Somali Regional State. Participants included pharmacists, nurses, doctors, psychiatric nurses, a psychiatrist, mental health volunteers, service users, and carers.1
Study sites were Jigjiga and Kabridahar, with recruitment from public hospitals, charity clinics, the regional health bureau, a public university, and Ilaaj facilities. Ilaaj facilities are religiously oriented inpatient settings that may combine Islamic care with biomedical elements.
Researchers identified 3 major themes:
- Mental health stigma.
- Societal neglect.
- Misunderstanding of mental ill health.
Those themes show the analysis was mapping a pathway from attitudes to help-seeking and health-system investment, with negative beliefs treated as one part of that pathway.
Binary Madness Framing Made Depression and Anxiety Hard to Recognize
Participants repeatedly described a binary model: a person is either “mad” or sane. In that framework, mental illness is recognized mainly when it is severe, visible, disruptive, psychotic, or socially frightening. Depression, anxiety, obsessive-compulsive disorder (OCD), posttraumatic stress disorder (PTSD), and early symptoms are easier to miss because they do not fit the visible “madness” category.
This recognition gap delays early care-seeking. Symptoms may be interpreted as ordinary distress, family trouble, moral weakness, spiritual attack, or something to hide until behavior becomes impossible to ignore.
The paper connects this to older Somali mental-health research. Prior work in UK Somali communities similarly found that depression was often not identified as mental illness, and that obvious behavioral disruption carried more recognition than internal suffering.3,5
A binary model can also delay recognition of early psychosis, trauma reactions, postpartum illness, obsessive-compulsive symptoms, medication side effects, substance-related syndromes, and suicidal thinking when the person still appears socially organized.
Two timing problems follow:
- Early symptoms are normalized. Distress may be treated as ordinary sadness, family conflict, spiritual trouble, or personality weakness.
- Severe symptoms become the entry point. Care may begin only when behavior becomes disruptive enough to force a family or community response.
For services, outreach needs more than formal psychiatric language about “mental illness.” It has to explain specific recognizable states: sleepless agitation, withdrawal, hearing voices, severe fear, persistent grief, trauma nightmares, self-neglect, and loss of function.
Spiritual Causes Shifted Care Toward Religious and Traditional Providers
Participants described mental distress as linked to jinn, evil eye, curses, khat chewing, alcohol use, smoking, abuse, neglect, poverty, and other life stressors. Biomedical and spiritual explanations were not mutually exclusive in these interviews, but spiritual explanations often made religious or traditional care the first stop.
In practice, this can delay biomedical treatment. Families usually make care decisions, especially when a person is visibly unwell. If the family’s explanatory model says the problem is spiritual, the first provider is likely to be religious or traditional. Biomedical care may come only after those approaches fail or symptoms become unmanageable.
Religious and traditional systems may be trusted, accessible, and culturally meaningful. The clinical risk is delay when treatable psychosis, severe depression, mania, epilepsy, substance-induced psychosis, or trauma-related illness goes without timely assessment.
Stigma Affected Employment, Marriage, Safety, and Service Funding
Stigma extended into ordinary social life. Participants described verbal abuse, stone-throwing, social isolation, concealment, family shame, exclusion from work, distrust around responsibility, and reduced marriage prospects.
Several concrete pathways appeared:
- Concealment: people hid symptoms or avoided outpatient clinics to avoid being labeled.
- Family isolation: families sometimes kept affected people out of public view.
- Employment exclusion: suspected mental illness reduced trust and responsibility.
- Marriage barriers: mental illness was treated as a family and social liability.
- Service stigma: mental-health services themselves were seen as low priority because the people who needed them were stigmatized.
The service-stigma pattern is especially sharp. One participant observed that when people with mental illness are stigmatized, their service is stigmatized too. Underinvestment is a budget problem and a social-status problem attached to the patient group.
Somali Region Services Need Earlier Recognition and Referral
Ethiopia already has evidence on mental-health stigma and severe mental-disorder service barriers, including public stigma in Jimma, perceived stigma among adults with mental illness, and barriers to equitable access in rural settings.6,7,8
Regional service fit: the Somali Region study adds cultural specificity. Services cannot assume that people will interpret depression, anxiety, trauma, psychosis, or relapse through the same categories used in biomedical psychiatry.
Care pathways are shaped by family authority, religious interpretation, stigma risk, service scarcity, medication supply, and whether the clinic itself is viewed as a place that will mark someone publicly.
Mental-health scale-up therefore has to include community education and trusted local translation. Adding a clinic without addressing stigma may produce an empty clinic, delayed presentation, or care-seeking only after severe deterioration.
A more realistic service model would treat religious leaders, families, primary-care workers, pharmacists, and local volunteers as part of the front door. This is not a replacement for psychiatric assessment; it is an acknowledgement of where people already go first and a way to build referral bridges from those settings.
The useful service targets are practical:
- Earlier recognition: teach symptom patterns that appear before crisis.
- Private access: reduce the fear that clinic attendance publicly labels a person or family.
- Referral trust: make biomedical care feel compatible with local religious and family authority rather than hostile to it.
- Medication continuity: improve supply and follow-up so treatment does not stop after first contact.
Referral bridge: earlier care becomes more realistic when biomedical services can work with trusted family and religious gatekeepers instead of treating them as obstacles.
Limitations of the Somali Region Stigma Study
- Small qualitative sample. The 16 interviews can map themes, not estimate how common each belief is across the region.
- Professional voices dominated. The authors noted that service-user and carer recruitment was difficult, and professional participants elaborated more freely.
- Stigma may have shaped participation. The same forces being studied may have made service users less willing or less able to speak openly.
- Regional specificity. Somali Region findings should not be automatically generalized to all Ethiopia, all Somali communities, or diaspora settings.
Care-Seeking Improves When Services Fit Local Explanatory Models
Service design: mental-health services need to work through religious and cultural models. If families first consult religious leaders, those leaders may need clear referral pathways.
If depression is not seen as illness, community education has to explain treatability without insulting local language or belief. If outpatient attendance exposes people to stigma, services need privacy, trust, and respectful staff behavior.
For a region with limited mental-health infrastructure, service sequence is part of the intervention:
- Reduce stigma around the person. People need to be treated as recoverable and socially included.
- Reduce stigma around the service. Mental-health clinics cannot be treated as low-status add-ons.
- Engage families and religious providers. They often shape the first care decision.
- Make early symptoms recognizable. Depression, anxiety, PTSD, and early psychosis need language that makes sense before crisis.
That is more likely to change care-seeking than simply telling people that biomedical psychiatry exists.
Questions About Mental-Health Stigma in Ethiopia’s Somali Region
Did the study say people only believe in spiritual causes?
No. Participants described spiritual causes, substance use, abuse, neglect, and life stress. The key point is that spiritual explanations often shaped first-line care-seeking.
Why does the binary “mad or sane” model delay care?
It makes mild and moderate mental illness easier to miss. A person with depression, anxiety, PTSD, or early psychosis may not be viewed as needing mental-health care until symptoms become severe and visible.
Does this mean religious care should be excluded?
No. In this setting, religious and traditional care are part of the actual pathway. The service-design question is how to create referral, collaboration, and earlier biomedical assessment when risk is high.
How should Somali Region services respond to the stigma pathway?
Mental-health investment has to address stigma directly. Otherwise, the same stigma that isolates patients can also keep services underfunded, hidden, and underused.
References
- Warfa N, Hanlon C, Abdulahi E, et al. “Since people who have mental illness are stigmatised, their service is also stigmatised”: exploring perceptions of mental health, stigma of mental illness, care-seeking and service use in the Somali Regional State of Ethiopia. BJPsych Open. 2026. doi:10.1192/bjo.2026.11016
- Warfa N, Hanlon C, Handuleh IMJ, Willott C, Hassen MA, Abdulahi E. Mental health services in the Somali Region of Ethiopia. Lancet Psychiatry. 2023;10:824-826. doi:10.1016/s2215-0366(23)00259-6
- Bhui K, Mohamud S, Warfa N, Craig T, Stansfeld S. Cultural adaptation of mental health measures: improving the quality of clinical practice and research. British Journal of Psychiatry. 2003;183:184-186. doi:10.1192/bjp.183.3.184
- Bhui K, Craig T, Mohamud S, et al. Mental disorders among Somali refugees: developing culturally appropriate measures and assessing socio-cultural risk factors. Social Psychiatry and Psychiatric Epidemiology. 2006;41:400-408. doi:10.1007/s00127-006-0043-5
- Linney C, Ye S, Redwood S, et al. “Crazy person is crazy person. It doesn’t differentiate”: an exploration into Somali views of mental health and access to healthcare in an established UK Somali community. International Journal for Equity in Health. 2020;19:190. doi:10.1186/s12939-020-01295-0
- Reta Y, Tesfaye M, Girma E, Dehning S, Adorjan K. Public stigma against people with mental illness in Jimma Town, Southwest Ethiopia. PLOS One. 2016;11:e0163103. doi:10.1371/journal.pone.0163103
- Hadera E, Salelew E, Girma E, Dehning S, Adorjan K, Tesfaye M. Magnitude and associated factors of perceived stigma among adults with mental illness in Ethiopia. Psychiatry Journal. 2019;2019:8427561. doi:10.1155/2019/8427561
- Hailemariam M, Fekadu A, Prince M, Hanlon C. Engaging and staying engaged: barriers to equitable access to mental healthcare for people with severe mental disorders in a rural African setting. International Journal for Equity in Health. 2017;16:156. doi:10.1186/s12939-017-0657-0