
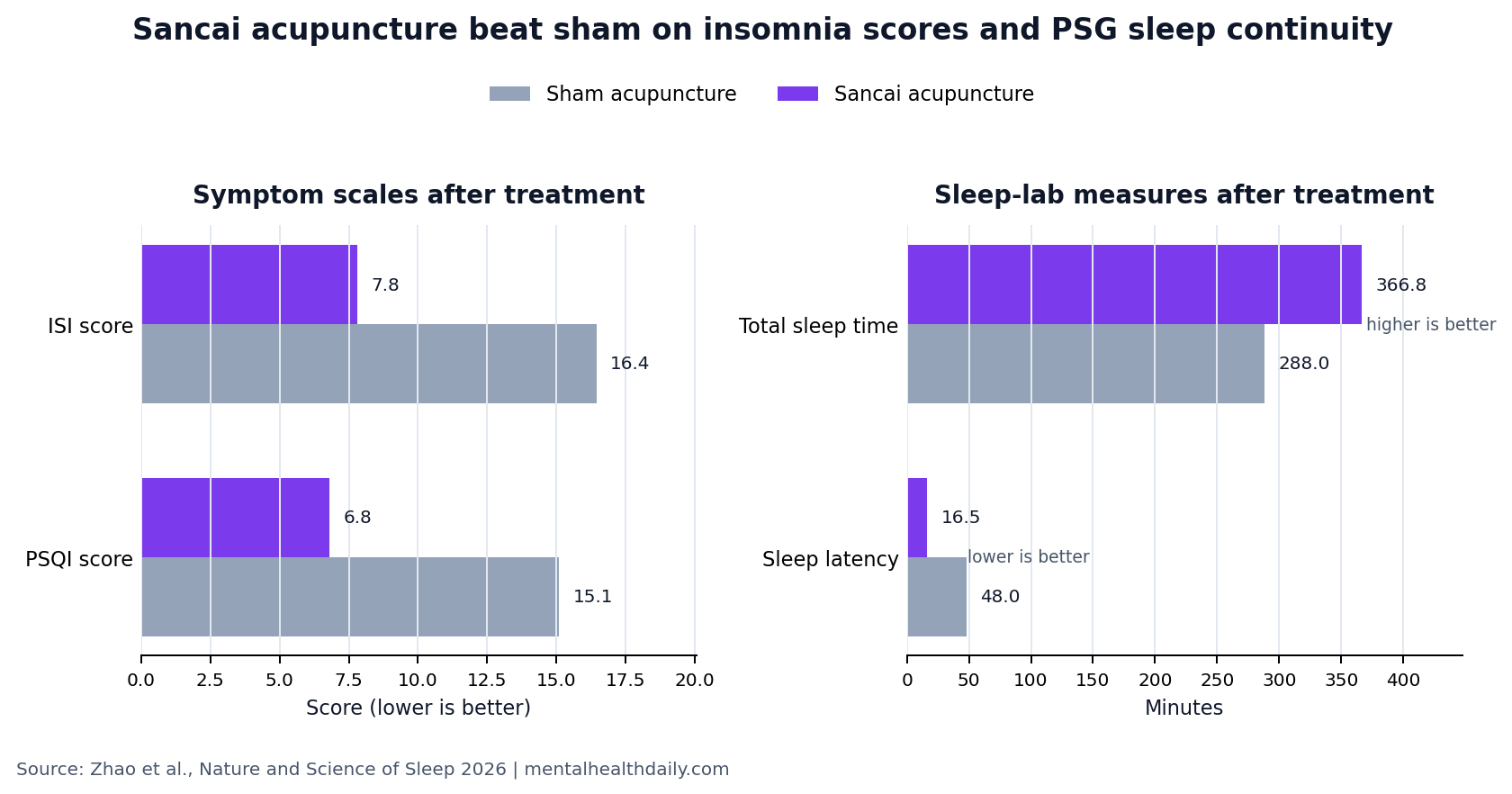
A 2026 randomized sham-controlled trial in 76 adults with primary insomnia found an 8-week Sancai acupuncture protocol reduced post-treatment Insomnia Severity Index scores to 7.80 vs. 16.45 with sham acupuncture, while total sleep time increased to 366.83 minutes vs. 287.97 minutes.1
Research Highlights
- Insomnia severity fell far more with real acupuncture: Zhao et al. randomized 38 adults to real Sancai acupuncture and 38 to sham acupuncture. Post-treatment ISI scores were 7.80 with real acupuncture vs. 16.45 with sham (SMD 2.130, p < .001).1
- Sleep-lab measures moved in the same direction: Post-treatment total sleep time was 366.83 minutes with real acupuncture vs. 287.97 minutes with sham, and sleep latency was 16.46 minutes vs. 47.97 minutes (both p < .001).1
- The durable signal was narrower: At 12-week follow-up, ISI remained lower with real acupuncture than with sham acupuncture (17.26 vs. 20.15, p = .002), but PSQI sleep-quality and SDS depression-score differences were not statistically confirmed.1
- Biomarkers support hypothesis generation, not mechanism proof: Serum 5-HT and BDNF rose more after real acupuncture than sham, but peripheral blood levels cannot establish central serotonergic or neuroplasticity changes in sleep circuits.1,8
- Safety looked mild in this small trial: 9 participants in the real-acupuncture group had mild bruising, with no serious adverse events, no infection, no syncope, and no withdrawals caused by adverse events.1
The result is stronger than a simple questionnaire-only acupuncture claim because it included non-penetrating sham needles, blinding checks, polysomnography, and serum biomarkers, but it still does not prove a central brain mechanism or long-term cure.
Sancai acupuncture is a protocol built around 3 body-region domains: head points intended to calm mental activity, chest/back points intended to regulate the heart-and-chest axis in traditional Chinese medicine, and foot/lower-limb points intended to reduce emotional stress and support bodily regulation. In this trial, the active treatment used Baihui (GV20), Shenting (GV24), Xinshu (BL15), Danzhong (CV17), Taibai (SP3), and Taichong (LR3).1
Primary insomnia means chronic insomnia not better explained by another sleep disorder, major psychiatric disorder, substance effect, or medical condition. The modern clinical standard still starts with cognitive behavioral therapy for insomnia (CBT-I), a structured behavioral treatment that changes sleep scheduling, stimulus control, sleep-related beliefs, and arousal patterns.
Acupuncture is being tested because access to high-quality CBT-I remains uneven and hypnotic medications carry tolerance, residual sedation, rebound, and dependence concerns for some patients.1,2
76 Adults Received 20 Sessions of Real or Sham Acupuncture
Zhao et al. conducted the trial at Yueyang Hospital of Integrated Traditional Chinese and Western Medicine in Shanghai between June 2023 and June 2024. Eligible participants were 18 to 65 years old, met International Classification of Sleep Disorders criteria for primary insomnia, and were either not using sleep medication or had stable sedative sleep-aid use for at least 3 months.1
Active protocol: participants received penetrating acupuncture at the 6 Sancai-linked points, with needle manipulation until DeQi sensation and 30-minute retention. Treatments were delivered 3 times per week for 4 weeks, then twice per week for 4 weeks, for 20 total sessions.
Sham protocol: participants received blunt non-penetrating placebo needles at the same points, through foam pads, for the same retention time. Participants, outcome assessors, polysomnography scorers, laboratory staff, and data analysts were blinded, although acupuncturists could not be masked.
Blinding checks were reassuring for participants: Bang’s Blinding Index was 0.143 in the real-acupuncture group and −0.077 in the sham group, within the authors’ adequate-blinding range. That does not eliminate performance bias from unblinded practitioners, but it reduces the concern that participants simply knew which treatment they received.
Post-Treatment ISI Scores Dropped Below the Clinical-Insomnia Range
Insomnia Severity Index (ISI) is a 7-item scale that rates insomnia symptoms and daytime impact; scores above 14 indicate clinically significant insomnia. Baseline ISI scores were similar: 20.84 in the real-acupuncture group and 21.58 in the sham group.1
After treatment, the real-acupuncture group averaged 7.80, while the sham group averaged 16.45. The between-group difference was large (SMD 2.130, 95% CI 1.535 to 2.725, p < .001). The real-acupuncture group also exceeded the trial’s predefined minimal clinically important difference: mean ISI reduction was 13.04 points, above the 4-point threshold.
Durability was mixed rather than all-or-nothing. ISI remained better at 12 weeks (17.26 vs. 20.15, p = .002), but the real-acupuncture mean had partly regressed. Pittsburgh Sleep Quality Index (PSQI) scores were strongly better immediately after treatment and at weeks 1 and 4, yet the 12-week PSQI difference was not statistically confirmed (16.11 vs. 15.06, p = .167).
Polysomnography Made the Result Harder to Dismiss as Expectancy Alone
Polysomnography is overnight sleep-lab recording that measures brain waves, eye movement, muscle activity, breathing, oxygen saturation, and cardiac signals. It matters here because insomnia trials often show subjective improvement without clear objective sleep change.
Objective sleep continuity favored real acupuncture after treatment:
- Total sleep time: 366.83 minutes with real acupuncture vs. 287.97 minutes with sham (p < .001).
- Sleep efficiency: 76.75% vs. 68.29% (p = .005).
- Sleep latency: 16.46 minutes vs. 47.97 minutes (p < .001).
- Wake after sleep onset: 96.69 minutes vs. 157.39 minutes (p < .001).
- Arousal index: 6.93 vs. 10.88 events/hour (p = .001).
- N3 slow-wave sleep: 29.61% vs. 24.54% (p = .034).
These sleep-lab results do not make acupuncture first-line ahead of CBT-I, and they do not show whether booster sessions are needed. They do make the Sancai trial more informative than studies that rely only on self-rated sleep quality.
5-HT and BDNF Rose, but Blood Biomarkers Are Not Brain Proof
5-HT (5-hydroxytryptamine, or serotonin) is a neurotransmitter involved in sleep-wake regulation, mood, and arousal. BDNF (brain-derived neurotrophic factor) is a growth factor involved in synaptic plasticity, stress resilience, and mood regulation. The trial measured both in serum before and after treatment.1,8
Post-treatment 5-HT was higher after real acupuncture than sham (101.91 vs. 87.07 ng/mL, p < .001). BDNF separated more sharply: 38.18 vs. 24.78 ng/mL (p < .001). The sham group had a smaller 5-HT increase but no significant BDNF change.
Mechanistic limit: serum biomarkers are peripheral measurements. They cannot prove that acupuncture changed serotonin signaling in the brainstem, hypothalamus, default mode network, salience network, or other sleep-regulation circuits. The cleaner interpretation is that biomarker changes tracked clinical response and justify neuroimaging or cerebrospinal-fluid follow-up, not that they settle the mechanism.
Earlier Acupuncture Evidence Fits the Direction, but Heterogeneity Still Matters
Kim et al.’s 2021 systematic review and meta-analysis reported that acupuncture improved insomnia outcomes across randomized trials, but the evidence base included heterogeneous protocols, controls, and outcome measures.4 Zhao et al.’s 2021 review asked a narrower question — whether acupuncture improves objective sleep indices in primary insomnia — and highlighted why objective endpoints need to be separated from questionnaire change.5
Earlier randomized trial evidence also points in the same broad direction. Yin et al. reported acupuncture benefits in primary insomnia in 2017, while a later electroacupuncture trial in patients with depression found insomnia improvement in a mood-disorder population.6,7 The new Sancai trial adds a protocol-specific sham-controlled test with PSG and biomarker data, not a final verdict on every acupuncture style.
Evidence-strength note: this was a small, single-center, sham-controlled RCT. It can support a short-term efficacy claim for the tested 20-session Sancai protocol in primary insomnia. It cannot show whether the protocol beats CBT-I, whether benefits persist without maintenance, whether the same result holds in broader clinics, or whether blood-marker changes reflect central nervous system repair.
Questions About Sancai Acupuncture for Insomnia
Did Sancai acupuncture beat sham acupuncture?
Yes on the primary post-treatment insomnia endpoint. ISI scores were 7.80 after real acupuncture vs. 16.45 after sham acupuncture, with a large standardized difference and p < .001. Several objective PSG measures also favored real acupuncture immediately after treatment.1
Did the benefit last 12 weeks?
Partly. ISI and anxiety scores remained significantly better at 12-week follow-up, but PSQI sleep-quality and SDS depression-score differences were no longer statistically confirmed. The 12-week data look like partial durability, not full maintenance of the immediate post-treatment response.
Does this mean acupuncture should replace CBT-I?
No. The trial compared Sancai acupuncture with sham acupuncture, not with CBT-I. It supports acupuncture as a plausible structured intervention for primary insomnia, especially where CBT-I access is limited, but it does not overturn CBT-I’s first-line role.
Were there safety concerns?
Safety looked acceptable in this small trial. Nine participants in the real-acupuncture group had mild bruising that resolved within 2 weeks, and no serious adverse events or withdrawals due to treatment were reported. Larger pragmatic trials would be needed to characterize uncommon harms.
What would make the finding more clinically decisive?
A larger multicenter trial comparing Sancai acupuncture with CBT-I, usual care, and credible sham control would be more decisive. Longer follow-up, booster-session testing, actigraphy or repeated PSG, and mechanistic neuroimaging would clarify whether the immediate objective sleep gains persist and who is most likely to respond.
References
- Acupuncture with the Sancai Acupoint Matching Method for Primary Insomnia: A Randomized Controlled Trial. Zhao N et al. Nature and Science of Sleep. 2026;18:590127. doi:10.2147/NSS.S590127
- Applying therapist-guided digital cognitive behavioral therapy for insomnia in psychiatry: a mixed-methods process evaluation. Reesen JE et al. BMC Psychiatry. 2025;25:428. doi:10.1186/s12888-025-06824-1
- Comparative effects of pharmacological interventions for the acute and long-term management of insomnia disorder in adults: a systematic review and network meta-analysis. De Crescenzo F et al. Lancet. 2022;400(10347):170-184. doi:10.1016/S0140-6736(22)00878-9
- Efficacy of acupuncture for insomnia: a systematic review and meta-analysis. Kim SA et al. American Journal of Chinese Medicine. 2021;49(5):1135-1150. doi:10.1142/S0192415X21500543
- Can acupuncture improve objective sleep indices in patients with primary insomnia? A systematic review and meta-analysis. Zhao FY et al. Sleep Medicine. 2021;80:244-259. doi:10.1016/j.sleep.2021.01.053
- Efficacy and safety of acupuncture treatment on primary insomnia: a randomized controlled trial. Yin X et al. Sleep Medicine. 2017;37:193-200. doi:10.1016/j.sleep.2017.02.012
- Effect of electroacupuncture on insomnia in patients with depression: a randomized clinical trial. Yin X et al. JAMA Network Open. 2022;5(7):e2220563. doi:10.1001/jamanetworkopen.2022.20563
- Brain-derived neurotrophic factor and mental disorders. Lin CC & Huang TL. Biomedical Journal. 2020;43(2):134-142. doi:10.1016/j.bj.2020.01.001