A 2026 population-based polysomnography study involving 1,206 adults found current smokers had 1.75x higher odds of worse obstructive sleep apnea severity than non-smokers or occasional smokers after adjustment for age and body mass index. Former smokers showed almost the same overall signal — 1.76x higher odds than never smokers — but that part of the result needs more caution because sex, obesity, pack-years, and quit timing were harder to separate.1
Research Highlights
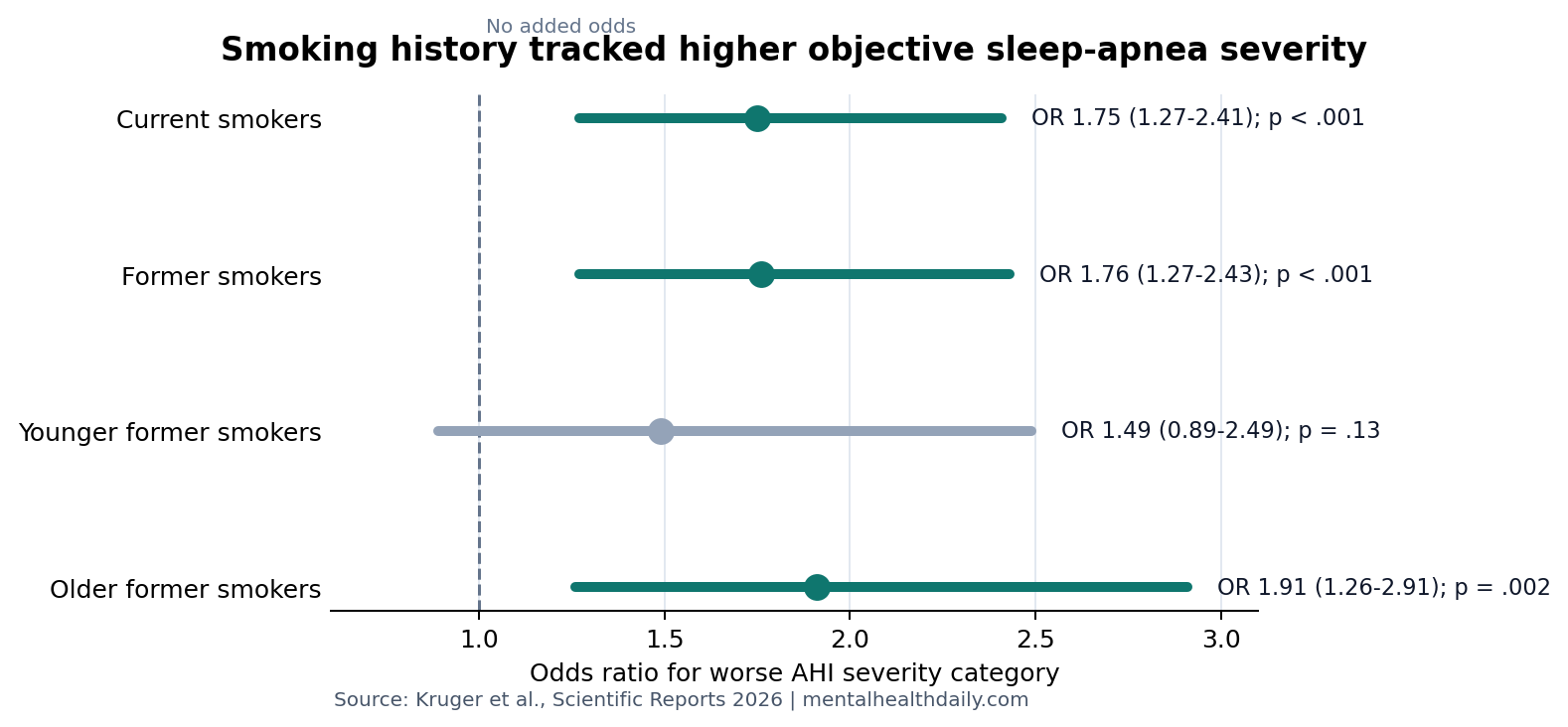
- Current smoking tracked higher objective OSA severity: Kruger et al. analyzed 1,206 adults from the Study of Health in Pomerania with overnight polysomnography and smoking interviews. Current smokers had higher odds of being in a worse apnea-hypopnea index (AHI) severity category than non-smokers or occasional smokers (OR 1.75, 95% CI 1.27 to 2.41, p < .001).1
- Former smoking was not a clean all-clear: Former smokers had higher severity odds than never smokers (OR 1.76, 95% CI 1.27 to 2.43, p < .001), but the sex- and pack-year sensitivity model was no longer statistically confirmed (β = 2.50 AHI events/hour, 95% CI −0.67 to 5.67, p = .12).1
- Age split changed the former-smoker pattern: Former smoking was not statistically confirmed in younger adults (OR 1.49, 95% CI 0.89 to 2.49, p = .13), while older former smokers had confirmed higher severity odds vs. older never smokers (OR 1.91, 95% CI 1.26 to 2.91, p = .002).1
- Polysomnography makes the study more useful than questionnaire screens: The study used attended overnight sleep-lab measurement instead of relying on a STOP-Bang or snoring questionnaire, which is important because population screening tools can misclassify OSA risk.1,4
- The design supports screening, not fatalism: Cross-sectional data cannot prove smoking caused irreversible airway damage. Smoking history should raise suspicion for OSA, while cessation and weight management remain separate risk-reduction targets.1,5
Obstructive sleep apnea (OSA) means repeated partial or complete upper-airway collapse during sleep. The common severity measure is the apnea-hypopnea index (AHI), the number of breathing pauses or shallow-breathing events per hour of sleep.
Smoking is biologically plausible as an OSA risk amplifier because cigarette smoke can inflame the upper airway, increase airway resistance, alter sleep architecture, and impair neuromuscular reflexes that help keep the airway open during sleep.3 The harder question is whether smoking history still predicts objectively measured OSA severity in a general-population sample rather than only in sleep-clinic patients who already have symptoms.
1,206 Adults Had Smoking Interviews and Overnight Sleep Testing
Kruger et al. used the SHIP-TREND-0 cohort from northeastern Germany. Out of 4,420 cohort participants, 1,264 agreed to attended overnight polysomnography — full sleep-lab recording with electroencephalography, eye movement, muscle activity, electrocardiography, respiratory effort, nasal pressure, oxygen saturation, snoring microphone, and body-position sensors.1
The final analytic sample included 1,206 people with complete AHI data and smoking interview data. Current regular smoking meant at least 1 cigarette per day. Former smoking meant regular smoking for at least 10 years and quitting at least 1 year earlier.
Current-smoking comparison: 208 current smokers were compared with 998 non-smokers or occasional smokers, a comparison group that included former smokers.
Former-smoking comparison: 190 former smokers were compared with 495 never smokers, with current smokers removed from that model.
Current Smokers Had 1.75x Higher Odds of Worse AHI Severity
The first model treated AHI as a continuous number. After adjustment for age and BMI, current smoking was associated with 3.11 additional AHI events/hour (95% CI 1.13 to 5.10, p = .002). Because model assumptions looked imperfect, the researchers also used ordinal logistic regression across AHI severity categories: normal (<5), mild (5 to <15), moderate (15 to <30), and severe (≥30).
That ordinal model is the cleaner headline: current smokers had higher odds of worse AHI severity than non-smokers or occasional smokers (OR 1.75, 95% CI 1.27 to 2.41, p < .001). Age-stratified analysis stayed positive in both younger adults (OR 1.56, p = .036) and older adults (OR 1.75, p < .001).1
Former Smoking Looked Similar Overall, Then Less Stable Under Sensitivity Testing
Former smokers had a higher mean AHI than never smokers: 15.1 vs. 9.4 events/hour. In the main ordinal model, former smoking was associated with 1.76x higher odds of worse AHI severity (95% CI 1.27 to 2.43, p < .001).1
The subgroup pattern was less uniform. Younger former smokers had a directionally higher but not statistically confirmed estimate than never smokers (OR 1.49, 95% CI 0.89 to 2.49, p = .13). Older former smokers had a stronger confirmed association than older never smokers (OR 1.91, 95% CI 1.26 to 2.91, p = .002).
Why the caveat matters: Former smokers were 78% male vs. 40% of never smokers and 52% obese vs. 33% of never smokers. When a reviewer-suggested sensitivity model added sex and pack-years with nonlinear age/BMI terms, the current-smoking association remained significant (β = 2.59 AHI events/hour, p = .02), but the former-smoking model did not (β = 2.50, p = .12).1
That does not erase the former-smoker signal. It lowers confidence that the overall former-smoker estimate cleanly isolates prior tobacco exposure from male sex, obesity, cumulative pack-years, or other factors that cluster in long-term smokers.
Polysomnography Adds Weight Beyond STOP-Bang Screening
Questionnaire-based OSA screening is useful, but it is not the same as measuring sleep breathing directly. The Korean health-behavior study by Chung and Kim linked behaviors to STOP-Bang OSA risk, but without polysomnography it could not say whether smoking tracked actual AHI categories.4
Measurement advantage: Kruger et al. filled that measurement gap by using attended overnight sleep testing. Smoking can affect snoring, sleep quality, daytime sleepiness, and cardiometabolic health in ways that may inflate or obscure questionnaire risk. AHI is still an imperfect endpoint, but it is closer to the disease mechanism than a checklist.
The new result also fits Zeng et al.’s 2023 meta-analysis, which found a smoking-OSA association most consistently in polysomnography-based studies and did not find a clear disappearance of risk among former smokers.2
Mechanisms Point to Airway Inflammation, Sleep Architecture, and Weight
Krishnan et al. summarized several routes by which smoking could worsen OSA: nasal and pharyngeal inflammation, mucosal edema, oxidative stress, altered arousal thresholds, and impaired upper-airway reflexes.3 Those mechanisms make current smoking a plausible contributor to airway collapsibility.
Former smoking is biologically harder to interpret. Persistent airway remodeling, cumulative vascular burden, and long-term inflammation are possible. So are confounding and selection effects: people who smoked for 10+ years and quit may differ from never smokers in occupation, cardiometabolic risk, alcohol exposure, body weight, and medical contact.
- Airway pathway: chronic smoke exposure can thicken or inflame upper-airway tissues, narrowing the collapsible segment during sleep.
- Neuromuscular pathway: nicotine and smoke exposure may alter reflexes that stabilize the pharyngeal airway.
- Weight pathway: smoking cessation can produce weight gain, while obesity is one of the strongest modifiable OSA drivers.
- Reverse pathway: OSA can worsen mood, fatigue, and quality of life, which may make quitting harder for some patients.
Otelea et al. argued that smokers with OSA may represent a recognizable clinical phenotype, not because smoking alone explains OSA, but because tobacco exposure, inflammation, obesity, and cessation barriers often travel together.5
Smoking History Should Trigger OSA Screening, Not Cessation Fatalism
The practical interpretation is straightforward: current and former smoking should increase suspicion for OSA, especially when snoring, witnessed apneas, hypertension, obesity, morning headaches, resistant fatigue, or cognitive complaints are present. Fietze et al. previously showed that OSA was common in the same SHIP-TREND population and rose strongly with age and male sex.6
Fatalism is the wrong inference. Kruger et al. explicitly warned that the former-smoker result should not be read as “the damage is already done.” Smoking cessation still reduces many cardiovascular, pulmonary, cancer, and vascular risks; weight management can be handled as a parallel OSA-reduction target rather than as a reason to keep smoking.1
Evidence-strength note: this was a cross-sectional observational analysis. It can support a screening and risk-stratification claim. It cannot prove that smoking caused OSA, that quitting fails to help OSA, or that any specific cessation sequence is best for a given patient.
Questions About Smoking and Sleep Apnea
Does smoking cause obstructive sleep apnea?
Smoking can plausibly worsen OSA through airway inflammation, oxidative stress, and upper-airway reflex changes, but this study cannot prove causality. It measured smoking status and AHI at the same broad timepoint, so it supports association and screening relevance rather than a direct cause-and-effect claim.1,3
Does quitting smoking lower sleep apnea risk?
Not clearly from this paper. Former smokers still had higher overall OSA severity odds than never smokers, but the former-smoker signal weakened in a sensitivity model that accounted for sex and pack-years. Longer quit duration, shorter smoking history, weight change after quitting, and baseline airway damage were not separated cleanly.
The practical answer is still to quit smoking, while also screening for OSA and managing weight when relevant.
Should smokers be screened for sleep apnea?
Yes when symptoms or risk factors are present. Smoking history alone is not a diagnosis, but in a patient with snoring, witnessed apneas, sleepiness, hypertension, obesity, depression symptoms, or cognitive complaints, it raises the value of asking about OSA and considering formal testing.
Why does the study focus on AHI?
AHI counts breathing disruptions per hour of sleep and is the standard severity metric for OSA. It does not capture every clinically important dimension — oxygen desaturation depth, arousal burden, sleep architecture, and symptoms also matter — but it is a direct objective measure from polysomnography.
Could OSA make quitting smoking harder?
Possibly. OSA can worsen fatigue, mood, irritability, and quality of life, which can undermine cessation attempts. That bidirectional possibility is one reason smoking cessation and OSA screening should be integrated rather than treated as unrelated problems.
References
- Breathing bad: increased risk for obstructive sleep apnea in current and former smokers. Kruger M et al. Scientific Reports. 2026;16:13382. doi:10.1038/s41598-026-48908-2
- Association between smoking behavior and obstructive sleep apnea: a systematic review and meta-analysis. Zeng X et al. Nicotine & Tobacco Research. 2023;25(3):364-371. doi:10.1093/ntr/ntac126
- Where there is smoke…there is sleep apnea. Krishnan V et al. Chest. 2014;146(6):1673-1680. doi:10.1378/chest.14-0772
- Association between health-related behaviors and obstructive sleep apnea among Korean adults. Chung Y & Kim JS. Scientific Reports. 2024;14:21244. doi:10.1038/s41598-024-72401-3
- Smoking obstructive sleep apnea: arguments for a distinctive phenotype and a personalized intervention. Otelea MR et al. Journal of Personalized Medicine. 2022;12(2):293. doi:10.3390/jpm12020293
- Prevalence and association analysis of obstructive sleep apnea with gender and age differences: results of SHIP-Trend. Fietze I et al. Journal of Sleep Research. 2019;28:e12770. doi:10.1111/jsr.12770
- Association between obstructive sleep apnea and multiple adverse clinical outcomes: evidence from an umbrella review. Wang Q et al. Frontiers in Medicine. 2025;12:1497703. doi:10.3389/fmed.2025.1497703