A 2026 review of electroacupuncture for depression found a familiar split: mechanistic evidence is rich, but clinical proof remains uneven because representative trials ranged from 65 to 270 participants, used different sham or drug comparators, and often failed to connect stimulation parameters with biological endpoints.1 Electroacupuncture is plausible as a subtype-matched neuromodulation strategy, but it is not yet a broadly proven depression treatment.
Research Highlights
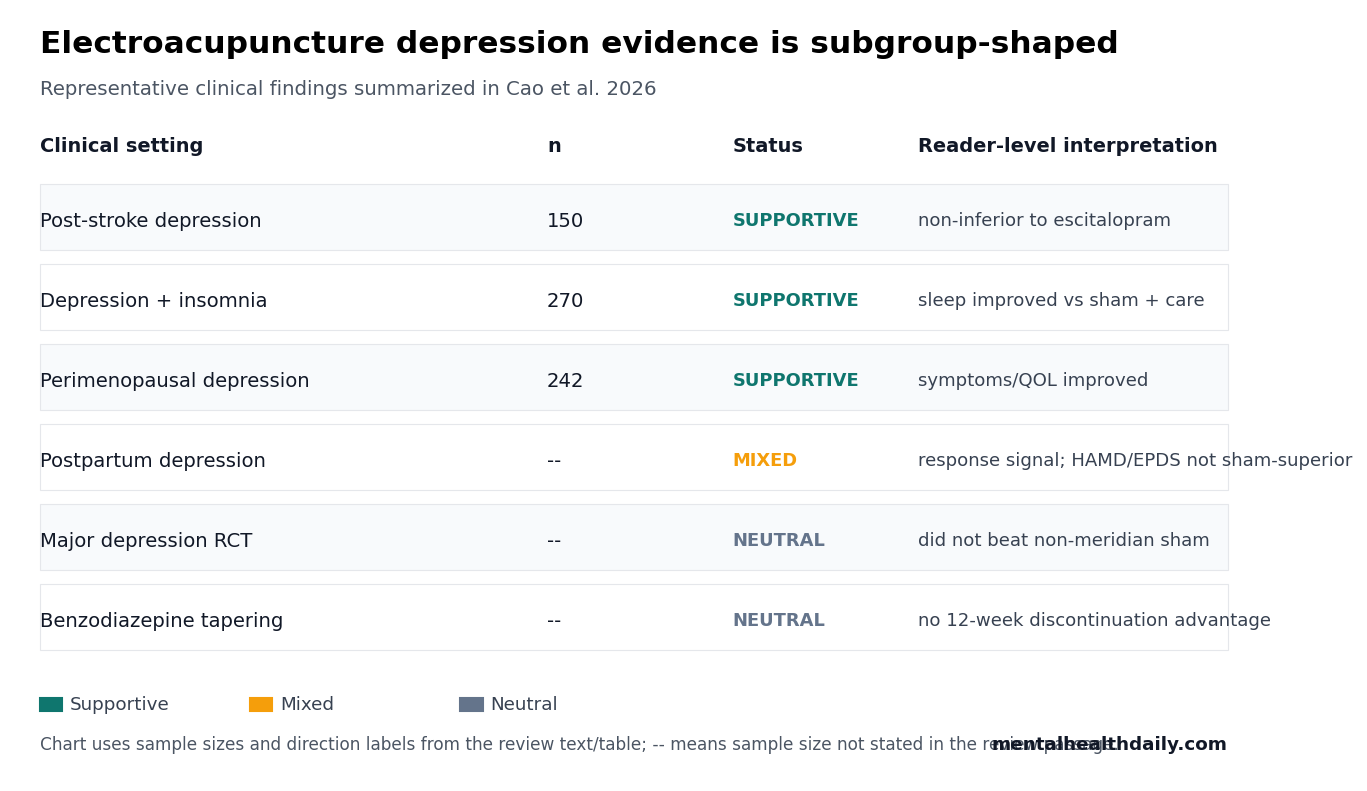
- Clinical evidence was heterogeneous: the review’s representative depression-related studies ranged from 65 to 270 participants and mixed post-stroke depression, perimenopausal depression, insomnia, pain comorbidity, and benzodiazepine tapering.
- Post-stroke depression looked most promising: a 150-person trial was summarized as non-inferior to escitalopram, while updated reviews have treated post-stroke depression as one of the more coherent electroacupuncture targets.
- Sham-controlled results were not uniformly positive: a US major-depression RCT did not beat non-meridian scalp sham stimulation, and a benzodiazepine-tapering trial found no 12-week discontinuation advantage vs. placebo acupuncture.
- Dose remains poorly defined: one first-episode depression protocol used 3 sessions weekly for 8 weeks, then 2 sessions weekly for 4 weeks, but deqi sensation was not quantitatively tied to response.
- Mechanisms need clinical anchoring: neural-circuit, IL-6/TNF-α, BDNF, autonomic, and gut-brain findings are plausible, but they need biomarker-stratified trials before they can guide patient selection.
Electroacupuncture is acupuncture with a small electrical current delivered through inserted needles. In depression research, the intervention is being studied as a form of peripheral neuromodulation that may influence brain circuits, autonomic tone, inflammation, sleep, and neuroplasticity.
Deqi is the traditional needle sensation described as soreness, heaviness, numbness, distension, or spreading sensation. Cao et al. treated deqi as part of the biological “dose” problem: 2 patients can receive the same frequency and session length while experiencing very different stimulation intensity.
Mechanisms Are Ahead of the Clinical Evidence
Cao et al. did not present a new randomized trial. Their review synthesized clinical and preclinical electroacupuncture work and argued that the main translational failure is not a shortage of proposed mechanisms. It is the failure to connect those mechanisms to standardized clinical protocols.
Mechanistic studies cited by the review covered several plausible antidepressant pathways:
- Neuroinflammation: electroacupuncture studies have reported effects on NF-κB, NLRP3 inflammasome activity, microglial polarization, and cytokines such as IL-6 and TNF-α.
- Neuroplasticity: animal studies have linked electroacupuncture with BDNF (brain-derived neurotrophic factor, a growth factor for brain cells), CaMKIIβ, hippocampal synaptic structure, and myelin-related repair pathways.
- Autonomic and vagal pathways: peripheral stimulation may engage vagal afferents, nucleus tractus solitarius pathways, heart-rate variability, and prefrontal-limbic regulation.
- Gut-brain signaling: some rodent work connects electroacupuncture to microbiota, short-chain fatty acids, serotonin pathways, and inflammatory bowel disease models with depressive-like behavior.
Those mechanisms are biologically interesting, but they do not by themselves prove clinical antidepressant efficacy. A forced-swim test, sucrose-preference test, or cytokine shift in a rodent model cannot map cleanly onto human depression symptoms such as guilt, rumination, suicidal ideation, impaired concentration, and functional disability.
Broader acupuncture evidence has the same problem in a less specific form. Chen et al. reviewed acupuncture for depression and found enough signal to keep the intervention scientifically active, but broad acupuncture reviews cannot answer the narrower electroacupuncture question: which electrical parameters, acupoints, and biological subtypes are doing the work?3
Clinical Trials Point to Subgroup Signals, Not a General Verdict
The strongest clinical signals in the review came from narrower populations rather than undifferentiated major depression. A 150-person post-stroke depression trial was summarized as showing non-inferiority to escitalopram, with electroacupuncture superior at some time points.2 A 65-person post-stroke depression RCT compared electroacupuncture with sham acupuncture and reported neurological-function improvement.
Hu et al.’s 2025 post-stroke depression review belongs in the same bucket: post-stroke depression is one of the more coherent electroacupuncture targets because the population, comparator, and neurological-recovery context can be specified more tightly.7
Other depression-adjacent settings were larger but still hard to combine. A 242-person perimenopausal depression trial compared acupuncture with escitalopram over 12 weeks and included symptoms plus quality-of-life outcomes. A 270-person depression-with-insomnia trial compared electroacupuncture with sham acupuncture plus standard care over 8 weeks, where sleep quality improved and depression/anxiety scores also moved.
Postpartum depression calibrates the signal: Fang et al.’s meta-analysis was summarized as showing better overall response rates, but it did not show significant superiority over sham electroacupuncture for Hamilton Depression Rating Scale or Edinburgh Postnatal Depression Scale scores.6 That pattern is more useful than a simple positive/negative label: response classification can look favorable while core symptom scales remain less convincing.
Sham Controls Keep the Evidence Honest
Sham acupuncture is not a perfect placebo. It can involve touch, expectation, clinician interaction, scalp or non-meridian needling, and physical sensations that may themselves change symptoms. Even so, sham-controlled studies are essential because depression outcomes are highly expectancy-sensitive.
Two neutral findings in Cao et al.’s review are especially important. Andreescu et al. tested acupuncture for major depressive disorder and found that a depression-specific protocol did not outperform non-meridian scalp sham stimulation.4 Yeung et al. tested electroacupuncture for tapering long-term benzodiazepine use and found no significant difference vs. placebo acupuncture in complete discontinuation or dose reduction at 12 weeks.5
Clinical implication: electroacupuncture may still help some patients, especially in enriched subgroups or as an adjunct. The evidence does not support treating it as a reliably superior stand-alone antidepressant across ordinary major depression populations.
Dose Is More Than Frequency
Drug trials can state a dose in milligrams. Electroacupuncture needs a broader dose language: frequency, current intensity, waveform, pulse width, session duration, number of sessions, acupoint selection, needle placement, tissue impedance, and patient sensation all potentially shape the biological effect.
Cao et al. used a first-episode depression protocol as an example: 3 sessions weekly for 8 weeks, then 2 sessions weekly for 4 weeks. The schedule was explicit, but the review noted that the deqi sensation was not quantitatively assessed or linked to treatment response.1
Frequency evidence: the review cited work suggesting that low-frequency electroacupuncture may affect neuroinflammatory pathways in methamphetamine-induced depressive-like behavior, but that animal work did not establish a full gradient model connecting frequency, biomarkers, and symptom change.8
A clinical field that cannot define dose precisely will struggle to explain why one trial works and another does not.
Biomarker Stratification Is the Right Test
Endophenotypes are measurable biological or behavioral traits that sit between a broad diagnosis and a mechanism. For depression, potential endophenotypes include inflammatory activation, sleep-rhythm disruption, autonomic imbalance, prefrontal-limbic circuit dysfunction, or fatigue-heavy metabolic profiles.
Cao et al. argued that future trials should pre-register patient stratification rather than treating all depression as the same target. A biomarker-enriched electroacupuncture trial might test whether patients with high inflammatory markers respond differently from patients with primarily sleep-rhythm or autonomic dysregulation.
This is where electroacupuncture could become scientifically interesting. If a protocol can be matched to a measurable phenotype, the claim moves from “acupuncture for depression” to a testable neuromodulation question: which stimulation parameters, at which points, in which biological subtype, change which symptom domain?
What Electroacupuncture for Depression Can Support Now
Evidence-strength note: Cao et al. 2026 is a review and translational proposal. It can organize the evidence, expose trial-design problems, and identify plausible research pathways. It cannot prove that electroacupuncture treats depression, because it did not randomize patients or estimate a new treatment effect.
The current evidence supports 3 cautious claims:
- Mechanistic plausibility is real: electroacupuncture can influence pathways relevant to depression biology in animal models and biomarker studies.
- Clinical promise is subgroup-shaped: post-stroke depression, insomnia-linked depression, and comorbidity-enriched settings look more coherent than a broad all-comers major-depression claim.
- Trial proof remains unfinished: sham-controlled results, dose uncertainty, subjective scales, small-to-medium samples, and limited long-term follow-up keep the evidence from being firm.
That practical role is narrow but not empty. A clinician-facing electroacupuncture trial would need to preserve standard depression care, define whether stimulation is being tested as add-on symptom relief or as a true antidepressant comparator, and separate mood change from sleep, pain, fatigue, and neurological-recovery effects.
Those domains often move together in real patients, but a trial that cannot separate them leaves the mechanism cloudy. A useful clinical test would name the subgroup, stimulation protocol, sham or active comparator, and pre-specified symptom domain where the biological pathway makes sense.
For now, electroacupuncture belongs in the research category of plausible adjunctive neuromodulation, not proven replacement therapy. A strong next trial would define stimulation dose, verify blinding, stratify patients by biomarkers, include objective sleep/autonomic/inflammatory endpoints, and still measure ordinary depression outcomes in language clinicians and patients can understand.
Questions About Electroacupuncture for Depression
Is electroacupuncture proven to treat major depression?
No. Some studies are encouraging, especially in specific subgroups, but sham-controlled and mixed findings prevent a general major-depression efficacy claim.
Could electroacupuncture be useful as an add-on treatment?
Possibly. The most defensible near-term role is adjunctive or subtype-matched use, especially when insomnia, post-stroke depression, pain comorbidity, or medication intolerance shapes the clinical problem.
What would make the evidence stronger?
Trials need explicit dosing, credible sham controls, long enough follow-up, biomarker-defined subgroups, and outcomes that connect mechanism to symptom change rather than relying only on broad rating-scale totals.
References
- Cao J, Ding D, Ming X, Liu C, Xu Y. Mechanism-driven translation of electroacupuncture for depression: bridging the gap between preclinical and clinical research. Neuropsychiatric Disease and Treatment. 2026;22:598864. https://doi.org/10.2147/ndt.s598864
- Ma F, Cao G, Lu L, Zhu Y, Li W, Chen L. Electroacupuncture versus escitalopram for mild to moderate post-stroke depression: a randomized non-inferiority trial. Frontiers in Psychiatry. 2024;15:1332107. https://doi.org/10.3389/fpsyt.2024.1332107
- Chen B, Wang CC, Lee KH, Xia JC, Luo Z. Efficacy and safety of acupuncture for depression: a systematic review and meta-analysis. Research in Nursing & Health. 2023;46(1):48-67. https://doi.org/10.1002/nur.22284
- Andreescu C, Glick RM, Emeremni CA, Houck PR, Mulsant BH. Acupuncture for the treatment of major depressive disorder: a randomized controlled trial. Journal of Clinical Psychiatry. 2011;72(8):1129-1135. https://doi.org/10.4088/jcp.10m06105
- Yeung WF, Chung KF, Zhang ZJ, et al. Electroacupuncture for tapering off long-term benzodiazepine use: a randomized controlled trial. Journal of Psychiatric Research. 2019;109:59-67. https://doi.org/10.1016/j.jpsychires.2018.11.015
- Fang X, Wang X, Zheng W, Han J, Ge X. Efficacy and safety of electroacupuncture in patients with postpartum depression: a meta-analysis. Frontiers in Psychiatry. 2024;15:1393531. https://doi.org/10.3389/fpsyt.2024.1393531
- Hu X, Pan Y, Tang Y, et al. Efficacy and safety of electroacupuncture-based comprehensive treatment for post-stroke depression: a systematic review and meta-analysis of randomized controlled trials. Frontiers in Psychiatry. 2025;16:1610032. https://doi.org/10.3389/fpsyt.2025.1610032
- Zhang J, Hui R, Xu J, et al. Low-frequency electroacupuncture attenuates methamphetamine-induced depressive-like behaviors and cognitive impairment via modulating neuroinflammation. Frontiers in Neurology. 2025;16:1652065. https://doi.org/10.3389/fneur.2025.1652065