
A 2026 cross-sectional study in Moshi, Tanzania found that only 26 of 246 injury patients who drank alcohol, or 10.6%, had ever told a healthcare provider about their alcohol use.1 The calibration result was contrary to the prediction: measured alcohol stigma did not track disclosure, while alcohol-related consequences did.
Research Highlights
- Disclosure was rare: among 246 injury patients who reported current or past-year alcohol use, 26 (10.6%) had previously disclosed alcohol use to a healthcare provider.
- Women were absent from the disclosure group: 0 of 43 women had disclosed alcohol use, while 26 of 203 men (12.8%) had done so.
- Consequences separated the groups: median Drinker Inventory of Consequences scores were 25.0 among patients who disclosed vs. 6.0 among those who did not.
- Perceived stigma missed the signal: perceived alcohol stigma showed no significant association with disclosure (OR 0.91, 95% CI 0.43-1.90, p = 0.82).
- Screening cannot wait for self-disclosure: 36.6% of the sample met the AUDIT threshold for hazardous drinking, far above the 10.6% who had disclosed.
Alcohol use disclosure means telling a medical doctor, nurse, or other healthcare professional about drinking. In alcohol use disorder care, disclosure is not a small administrative step. It is often the point where screening, brief counseling, referral, medication discussion, or harm-reduction advice becomes possible.
Alcohol use disorder (AUD) is a pattern of drinking that causes impaired control, craving, risky use, tolerance, withdrawal, or continued use despite harm. Many health systems still find AUD through self-report tools and patient-provider conversations, so the person who never says anything can stay invisible even after an injury, hospital visit, or repeated alcohol-related consequence.
Nickenig Vissoci et al. studied injury patients at Kilimanjaro Christian Medical Center, a major referral hospital in northern Tanzania.1 The sample came from an emergency-department setting, not a specialty addiction clinic, which makes the finding more practical: an injury visit may be one of the few moments when hazardous drinking is visible to the healthcare system.
Only 10.6% of Drinking Injury Patients Had Told a Provider
The researchers enrolled 341 injury patients, excluded 95 who abstained from alcohol, and analyzed 246 people who reported current or past-year alcohol use. Previous disclosure was uncommon: 26 patients had ever talked with a medical doctor or other professional about alcohol use, while 220 had not.
The study measured disclosure against several alcohol-related variables:
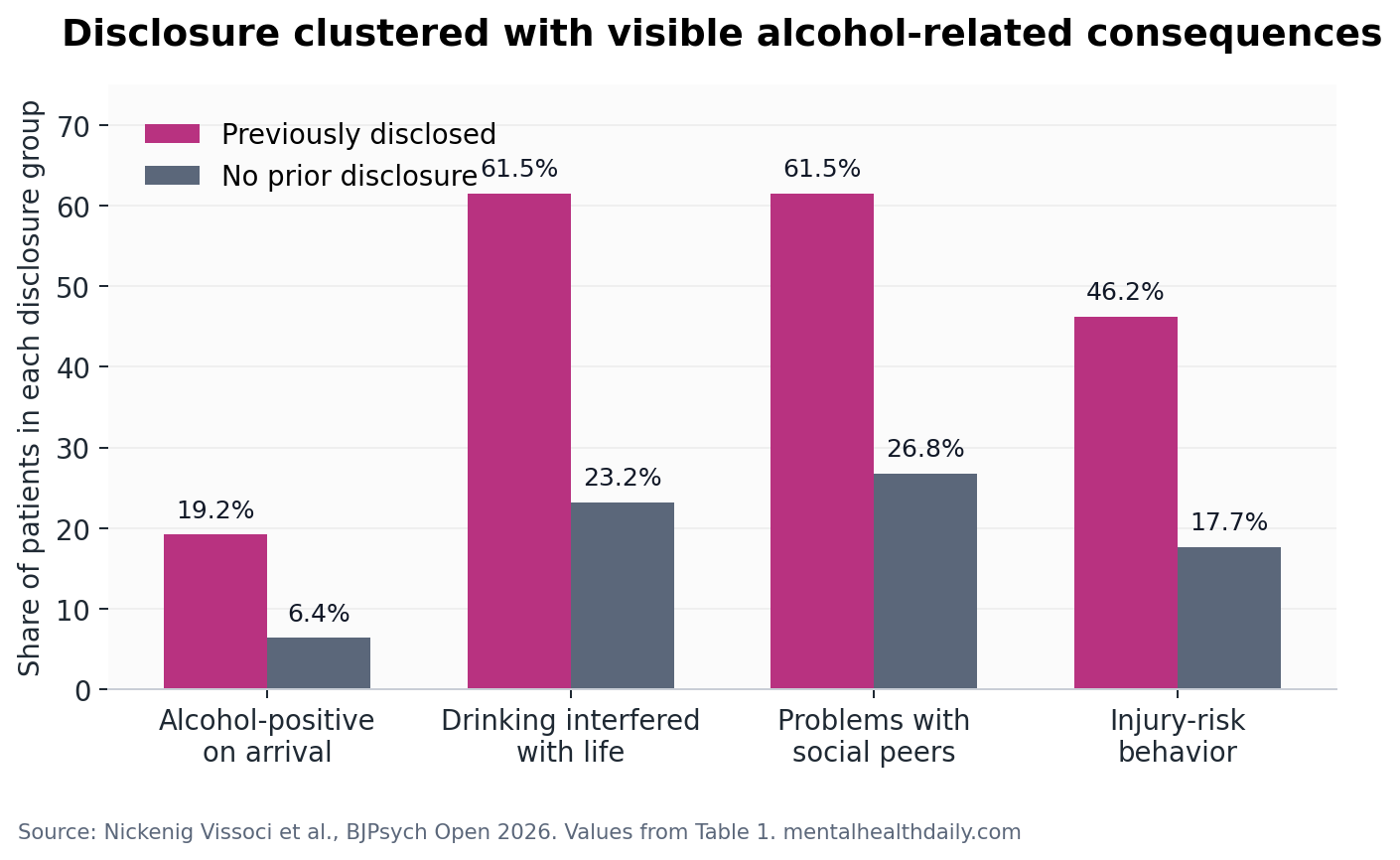
- Alcohol-positive arrival: 19.2% of patients who disclosed were alcohol-positive on arrival vs. 6.4% of those who did not disclose.
- Drinks per day: the disclosure group reported a median of 4.0 drinks per day vs. 2.0 in the non-disclosure group.
- AUDIT score: median Alcohol Use Disorders Identification Test score was 19.0 vs. 4.0.
- Alcohol consequences: median Drinker Inventory of Consequences score was 25.0 vs. 6.0.
AUDIT, the Alcohol Use Disorders Identification Test, is a 10-item screening tool for hazardous and harmful drinking. Scores run from 0 to 40, and a cut-off of 8 or higher is commonly used to flag risky alcohol use.
In Tanzania specifically, Vissoci et al. had already shown that the Swahili-adapted AUDIT retained useful psychometric performance in Moshi, supporting its use as a local screening measure rather than an imported form used blindly.2
The Tanzanian AUDIT validation matters here because Nickenig Vissoci et al. connected worse drinking, alcohol-related harm, and prior disclosure inside a locally tested measurement context. A screening instrument and a consequence inventory pointed toward the same practical conclusion: waiting for spontaneous disclosure misses many people whose alcohol use is clinically relevant.
Alcohol-Related Consequences Predicted Disclosure Better Than Stigma
Patients who said drinking interfered with life were much more likely to have disclosed alcohol use (61.5% vs. 23.2%; OR 17.45, 95% CI 4.31-118.49, p < 0.01).
Problems with social peers were also more common in the disclosure group (61.5% vs. 26.8%; OR 6.86, 95% CI 2.09-27.21, p < 0.01), as was drinking-related risk behavior linked to injury (46.2% vs. 17.7%; OR 5.93, 95% CI 1.72-20.89, p < 0.01).
Drinker Inventory of Consequences (DrInC) is a 50-item measure of alcohol-related harms across interpersonal, physical, social, impulsive, and intrapersonal domains. It asks a different question from AUDIT. AUDIT screens drinking severity and hazardous use; DrInC captures the damage drinking has already produced.
Mediation result: harmful alcohol use was associated with disclosure, but the pathway appeared to run through alcohol-related consequences. In the researchers’ path model, harmful alcohol use correlated with alcohol-related consequences (R = 0.60), and the indirect effect through consequences was larger than the direct effect without that mediator.
Conner et al. found a related pattern in treatment-naive people with severe alcohol use disorder: alcohol-related consequences were tied to intention to seek care.5 The Moshi injury-patient study extends that logic into an emergency-department disclosure question. People may speak when the consequences have become hard to ignore, but that is late triage, not early detection.
Measured Alcohol Stigma Did Not Explain Disclosure
The researchers expected stigma to be important. Perceived alcohol stigma refers to the expectation that people who drink heavily will be devalued, discriminated against, or socially rejected. The study used an alcohol-adapted perceived devaluation-discrimination scale and converted responses into a 0-100 factor score.
The prediction did not hold. Median perceived alcohol stigma was nearly the same in the disclosure and non-disclosure groups (24.1 vs. 22.7), and the association with disclosure was not significant (OR 0.91, 95% CI 0.43-1.90, p = 0.82). The researchers also reported no significant gender difference in perceived alcohol stigma scores.
This is the calibrated interpretation: the study does not prove stigma is irrelevant to alcohol care in Tanzania. It shows that this measured stigma variable did not explain whether injury patients had ever disclosed drinking to a provider. That narrower claim is still useful because it redirects attention toward consequence-based screening, provider workflow, and whether patients interpret injury care as a safe moment to discuss alcohol.
Alcohol stigma remains a real construct in other settings. Glass et al. developed and validated a perceived alcohol stigma measure and linked stigma expectations with poorer mental health and lower treatment-seeking likelihood among drinkers in high-income settings.6
Finn et al. also found that public stigma influenced treatment preferences for alcohol use disorders, including whether people preferred primary care or specialized services.7 Nickenig Vissoci et al. therefore contradict a simple stigma-first story, not the existence of stigma itself.
0 of 43 Women Disclosed Alcohol Use
The gender result is impossible to ignore and easy to overread. Among 43 women in the sample, 0 had disclosed alcohol use to a healthcare provider. Among 203 men, 26 had disclosed, or 12.8%.
The subgroup is small, so it should not be treated as a stable population estimate for all women in Moshi or Tanzania. It does, however, fit with qualitative work from the same research ecosystem. Pauley et al. interviewed people in Moshi about alcohol, gender, stigma, and sexual assault, and participants described harsher social judgment toward women who drink than toward men who drink.4
Clinical implication: universal screening protects against a disclosure-only model that depends on patients volunteering stigmatized information. If women, injured patients, or socially exposed drinkers are less likely to disclose, the health system needs a normal, routine alcohol-screening process that does not make disclosure feel like a personal confession.
Pauley et al. also showed why the emergency department is a logical place to ask. In a separate Moshi emergency-department analysis, alcohol use and harmful drinking were common among patients receiving acute care, and injury presentations were part of the alcohol-harm pattern.3 Injury care is not an addiction clinic, but it can be a high-yield point for brief screening and referral.
Emergency-Department Screening Should Not Depend on Confession
Operationally, a clinician does not need to decide whether stigma, denial, fear, transport delay, gender norms, or treatment pessimism is the single true reason a patient stays silent. The safer default is to build alcohol screening into injury care before the patient has to initiate the topic.
Screening language: a patient presenting after injury may not see alcohol as the reason for the visit, may not trust confidentiality, or may not know what help would follow a positive screen.
In low-resource settings, asking about alcohol without a referral pathway can feel extractive. The Moshi study points toward several concrete design requirements:
- Routine screening: ask everyone in a relevant injury pathway rather than singling out people who look intoxicated.
- Locally validated tools: use instruments such as the Swahili-adapted AUDIT when they have evidence in the target setting.
- Consequence prompts: ask about injuries, peer problems, daily-life interference, and risk behavior alongside quantity and frequency.
- Nonpunitive framing: make clear that the goal is treatment, safety, and injury prevention, not blame.
- Referral realism: connect screening to trained providers or brief interventions that can actually be delivered.
Evidence-strength note: this was a cross-sectional survey with exploratory path analysis. It can show which factors were associated with prior disclosure, and it can identify a plausible consequence-mediated pattern. It cannot prove that consequences caused disclosure, that stigma has no causal role, or that universal emergency-department screening would improve alcohol-treatment uptake by a specific percentage.
The study still changes the screening logic. If disclosure rises only after alcohol has already disrupted life, damaged social relationships, or contributed to injury-risk behavior, disclosure is a late signal. Emergency-department alcohol screening should be designed to catch the risk before the patient has to supply that signal on their own.
Questions About Alcohol Disclosure in Tanzania
Did the study show that stigma does not matter?
No. It showed that measured perceived alcohol stigma was not associated with prior disclosure in this injury-patient sample. Stigma may still affect treatment-seeking, gendered judgment, trust, and willingness to discuss alcohol in other contexts.
Why focus on injury patients?
Injury care can make alcohol risk visible at a moment when the patient is already inside the healthcare system. That creates an opportunity for screening, brief intervention, and referral, especially in settings where specialty addiction care is scarce.
What does the 10.6% disclosure number mean?
It means only 26 of 246 injury patients who reported current or past-year alcohol use had ever talked with a medical doctor or other professional about alcohol use. Risky drinking was more common than disclosure; 36.6% of the sample met the AUDIT threshold for hazardous drinking.
Should every emergency department screen for alcohol use?
The Moshi data support routine screening as a safer model than waiting for self-disclosure, but implementation depends on staffing, training, referral options, privacy, and locally validated screening tools.
References
- Nickenig Vissoci JR, Nascimento de Oliveira N, Mwita WC, et al. Factors associated with reporting behaviour of alcohol use in Moshi, Tanzania. BJPsych Open. 2026;12(3):e109. https://doi.org/10.1192/bjo.2026.11010
- Vissoci JRN, Friedman K, Caruzzo NM, et al. Clinical evaluation of the alcohol use disorders identification test (AUDIT) in Moshi, Tanzania. PLOS One. 2023;18(11):e0287835. https://doi.org/10.1371/journal.pone.0287835
- Pauley A, Thatcher EC, Sarafian JT, et al. Alcohol use among emergency medicine department patients in Tanzania: a comparative analysis of injury versus non-injury patients. PLOS Global Public Health. 2023;3(11):e0001900. https://doi.org/10.1371/journal.pgph.0001900
- Pauley A, Metcalf M, Buono M, et al. “When a man drinks alcohol it’s cool but when a woman drinks she is a hoe”: a qualitative exploration of alcohol, gender, stigma, and sexual assault in Moshi, Tanzania. PLOS Global Public Health. 2024;4(1):e0002382. https://doi.org/10.1371/journal.pgph.0002382
- Conner KR, Abar B, Aldalur A, Chiang A, Hutchison M, Maisto SA, et al. Alcohol-related consequences and the intention to seek care in treatment-naive women and men with severe alcohol use disorder. Addictive Behaviors. 2022;131:107337. https://doi.org/10.1016/j.addbeh.2022.107337
- Glass JE, Kristjansson SD, Bucholz KK. Perceived alcohol stigma: factor structure and construct validation. Alcoholism: Clinical and Experimental Research. 2013;37(Suppl 1):E237-E246. https://doi.org/10.1111/j.1530-0277.2012.01887.x
- Wallhed Finn S, Mejldal A, Nielsen AS. Public stigma and treatment preferences for alcohol use disorders. BMC Health Services Research. 2023;23:76. https://doi.org/10.1186/s12913-023-09037-y