A 2026 study of 958 adults entering Japanese multidisciplinary pain centers found that 17.1% screened positive for ADHD, rising to 27.4% among patients whose average pain was NRS 9-10; ASD screening was 4.4% overall and did not show the same pain-intensity signal.1
Research Highlights
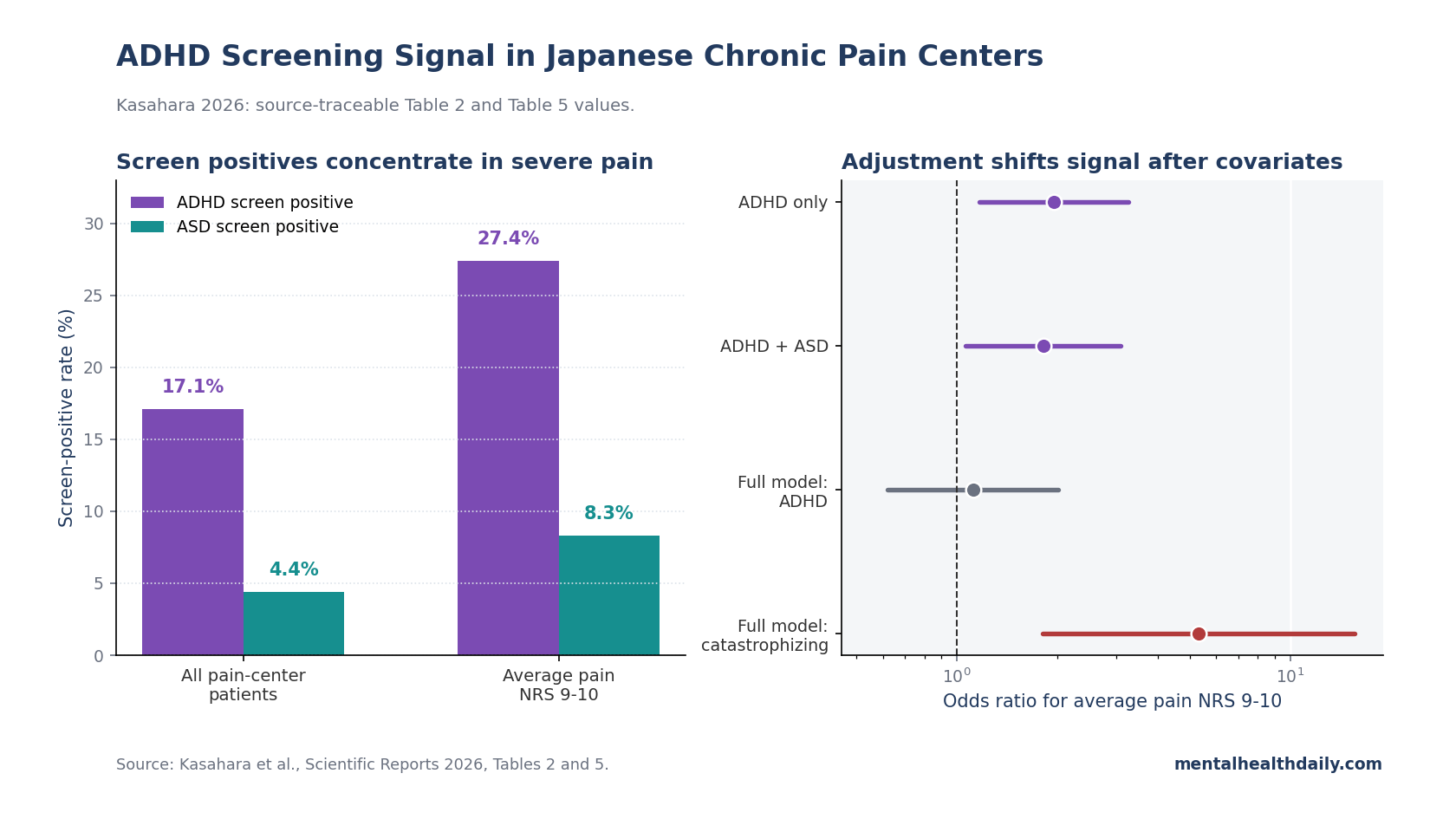
- ADHD screening was elevated in tertiary pain care: 164 of 958 patients (17.1%) screened positive on the Adult ADHD Self-Report Scale, compared with 42 of 958 (4.4%) on the Autism-Spectrum Quotient.1
- Severe pain carried the strongest ADHD signal: 23 of 84 patients with average NRS 9-10 pain (27.4%) screened positive for ADHD, versus 141 of 874 patients (16.1%) with NRS < 9.1
- ASD did not track pain intensity the same way: ASD screening was 8.3% in the NRS 9-10 group and 4.0% in the NRS < 9 group, a nonsignificant difference after correction (p = 0.32).1
- Adjustment changed the interpretation: ADHD had an unadjusted odds ratio of 1.96 for NRS 9-10 pain, but the fully adjusted estimate fell to 1.12 after education, anxiety/depression, insomnia, catastrophizing, and self-efficacy entered the model.1
- Catastrophizing became the stronger clinical flag than ADHD screen positivity: in the full model, pain catastrophizing had an odds ratio of 5.32 for NRS 9-10 pain, and path analysis linked ADHD symptoms to severe pain indirectly through anxiety/depression and catastrophizing.1
the calibrated interpretation is narrow but important: this is not proof that ADHD causes chronic pain, and it is not a reason to hand stimulants to every pain patient. It is evidence that ADHD-like attentional and emotional dysregulation may identify a subgroup in which severe persistent pain is routed through anxiety, depression, and pain catastrophizing.
ADHD means attention-deficit/hyperactivity disorder, a neurodevelopmental condition involving inattention, impulsivity, executive-function difficulty, and emotional regulation problems. ASD means autism spectrum disorder, a neurodevelopmental condition involving social-communication differences and restricted or repetitive behavioral patterns; ASD can involve sensory sensitivity, but this study did not find an ASD-specific pain-intensity gradient.
958 First-Visit Pain-Center Patients Were Screened
Kasahara et al. studied adults with persistent chronic pain despite standard care at their initial visit to 13 multidisciplinary pain centers in Japan from June 2019 through December 2021.1 About 4,128 patients attended an initial visit and were approached; 958 provided consent and completed the self-administered questionnaires used in the analysis.
The cohort was not a community chronic-pain sample. These were tertiary-care referrals whose pain had continued despite pharmacological treatment, nerve blocks, rehabilitation, or other standard care in primary or secondary settings.
That selection matters because complex pain clinics concentrate patients with psychiatric comorbidity, sleep disruption, disability, and prior treatment failure.
The main tools were straightforward:
- ADHD symptoms: the Adult ADHD Self-Report Scale (ASRS), an 18-item measure with a 6-item screener; the paper cited sensitivity of 68.7% and specificity of 99.5% for the screener.6
- ASD symptoms: the 50-item Autism-Spectrum Quotient (AQ), using AQ ≥ 33 as the screen-positive cutoff.
- Pain severity: average pain on a 0-10 Numerical Rating Scale (NRS), with NRS 9-10 treated as extremely severe pain.
- Psychosocial pathways: Hospital Anxiety and Depression Scale (HADS), Athens Insomnia Scale, Pain Catastrophizing Scale (PCS), pain self-efficacy, disability, and quality of life.
Pain catastrophizing is the tendency to magnify pain threat, ruminate about pain, and feel helpless in response to pain. In chronic pain research it is not an insult or a claim that pain is imaginary; it is a measurable cognitive-affective pattern that predicts pain interference and treatment difficulty.
ADHD Positivity Rose in the NRS 9-10 Group
The study’s most direct descriptive result was the screening prevalence. Among all 958 patients, 164 screened positive for ADHD (17.1%) and 42 screened positive for ASD (4.4%).
Among the 84 patients reporting average pain NRS 9-10, 23 screened positive for ADHD (27.4%). The lower-pain comparison group, NRS < 9, had 141 ADHD-positive screens among 874 patients (16.1%).1
That is the first calibration. ADHD screen positivity was more than high in pain centers overall; it was higher in the extremely severe pain subgroup.
Figure 2 grouped average NRS into 6 levels, and the ASRS-positive rate increased significantly across pain-intensity levels (p < 0.01). The figure caption reported the group sizes: NRS grade 0 had 6 patients, grade 1 had 80, grade 2 had 223, grade 3 had 327, grade 4 had 238, and grade 5 had 84.1
ASD screening looked different. The NRS 9-10 group had 7 ASD-positive patients (8.3%), while the NRS < 9 group had 35 (4.0%), but the corrected comparison was not statistically significant (p = 0.32).
Continuous AQ scores correlated with pain catastrophizing (Spearman’s rho = 0.24, p < 0.001), but not with NRS pain-intensity measures.1
The Full Model Shifted Away From Direct ADHD Effects
The unadjusted logistic model made ADHD look like a direct marker of extremely severe pain: OR 1.96, 95% CI 1.17-3.27, p < 0.01. After ASD entered the model, the ADHD estimate remained significant at OR 1.82, 95% CI 1.06-3.10, p < 0.05.
That is enough to reject a lazy explanation that the ADHD signal is just generic neurodevelopmental overlap with ASD.1
The signal changed once the model added the variables pain clinicians already worry about. In the fully adjusted model, ADHD fell to OR 1.12, 95% CI 0.62-2.02.
ASD was also nonsignificant at OR 1.63, 95% CI 0.63-4.21. The remaining significant variables were junior-high-school education (OR 2.00, 95% CI 1.12-3.58), anxiety/depression (OR 1.87, 95% CI 1.05-3.32), and pain catastrophizing (OR 5.32, 95% CI 1.81-15.6).1
That pattern does not erase ADHD. It places ADHD upstream of a plausible pathway rather than as a stand-alone pain generator.
If ADHD symptoms feed emotional dysregulation, sleep difficulty, task paralysis, rumination, missed appointments, and inconsistent home practice, the pain-center problem may look like “severe refractory pain” while the treatable bottleneck is partly executive and emotional control.
Path Analysis Put Anxiety, Depression, and Catastrophizing in the Middle
Path analysis is a statistical model that tests whether the observed correlations are compatible with a proposed chain of relationships. It does not prove causality, especially in a cross-sectional study, but it can show whether a directional model fits the data better than a simple direct-association story.
Kasahara et al. tested models in which ADHD symptoms linked to a latent severe-pain construct built from NRS 9-10 status and Brief Pain Inventory severity. The best-fitting simpler model linked ADHD symptoms to anxiety/depression with a standardized coefficient of 0.54, then linked anxiety/depression to severe chronic pain with a coefficient of 0.32.
The total indirect coefficient from ADHD symptoms to severe pain was 0.17.1
A second clinically favored model inserted pain catastrophizing between anxiety/depression and severe pain. In that model, ADHD symptoms linked to anxiety/depression at 0.54, anxiety/depression linked to catastrophizing at 0.57, and catastrophizing linked to severe chronic pain at 0.43.
The total indirect coefficient from ADHD symptoms to severe pain was 0.13.1
The distinction is practical. Screening for ADHD in pain centers is not mainly about labeling pain as psychiatric.
It is about finding patients whose attention, emotion regulation, and pain-threat appraisal may be blocking standard rehabilitation from working as intended.
Earlier Studies Pointed in the Same Direction
A representative English adult sample had already found a similar attenuation pattern. Stickley et al. analyzed 7,403 adults from the 2007 Adult Psychiatric Morbidity Survey and reported that ASRS score ≥ 14 was associated with extreme pain at OR 3.15, 95% CI 2.09-4.74.
After common mental disorders entered the model, the estimate fell to OR 1.64, 95% CI 1.05-2.58, meaning anxiety and depression explained much of the association but not all of it.2
A 2025 Japanese internet survey by Kasahara et al. moved the question into a 4,028-person adult sample and found both direct and indirect paths from ADHD symptoms to chronic pain through mental health problems.3 The 2026 pain-center paper is more clinically concentrated: in patients whose pain had already resisted standard care, the model no longer needed a significant direct ADHD-to-severe-pain path once anxiety/depression and catastrophizing were modeled.
Developmental pain pathway: Battison et al.’s youth scoping review gives the mechanism a developmental frame: attention problems, executive dysfunction, and emotional dysregulation can plausibly worsen pain coping, adherence, and disability even before adult pain-center referral.4
Wiwe Lipsker et al. also found, in 146 children with chronic pain, that autistic traits and ADHD symptoms related to pain interference, depression, and health-related quality of life rather than supporting a simple pain-intensity-only explanation.5
Clinical Use Is Screening, Not Overclaiming
The strongest case for pain-center ADHD screening is operational. The ASRS-6 is brief, low-cost, and already validated for adult ADHD screening.
In this Japanese referral sample, it flagged roughly 1 in 6 patients overall and more than 1 in 4 patients in the NRS 9-10 subgroup. A positive screen should not be treated as a diagnosis, but it gives the pain team a reason to ask about lifelong inattention, impulsivity, restlessness, emotional outbursts, missed routines, and difficulty completing rehabilitation tasks.
Treatment implications should stay conservative. ADHD medications may help some patients with comorbid ADHD and chronic pain, and a 2025 Frontiers review described medication strategies tailored to behavioral features in chronic pain.7
But the 2026 study did not randomize ADHD treatment, did not test stimulant analgesia, and did not show that treating ADHD alone reduces pain. It supports a multidisciplinary path: diagnose ADHD carefully when screens are positive, treat anxiety/depression and catastrophizing directly, and adapt pain rehabilitation for executive-function problems.
For patients, the sensible question is not “Is my pain all ADHD?” The better question is whether untreated ADHD symptoms are making pain care harder to execute: remembering exercises, pacing activity, attending sessions, sleeping regularly, avoiding rumination spirals, and staying with a plan long enough to see whether it works.
Limitations of This Japanese Pain-Center Study
Screeners are not diagnoses. ASRS and AQ results identify probable symptom profiles, not clinician-confirmed ADHD or ASD. Chronic pain can also impair attention, sleep, mood, and executive function, so some positive ADHD screens may reflect pain burden rather than lifelong ADHD.
Cross-sectional mediation is not causation. The path model fits an ADHD → anxiety/depression → catastrophizing → severe pain pathway, but the reverse sequence is also plausible. Severe chronic pain can produce insomnia, depression, anxiety, and concentration problems.
The sample is referral-biased. Tertiary multidisciplinary pain centers see a harder group than primary care or community chronic pain samples. The 17.1% screen-positive rate should not be quoted as the prevalence of ADHD in all chronic pain.
ASD inference was underpowered. Only 42 patients screened positive for ASD, and AQ dichotomization may miss subtler adult ASD presentations. The paper’s negative ASD pain-intensity finding is useful, but it should not be read as proof that ASD is irrelevant to pain experience.
Questions About ADHD Screening in Chronic Pain Clinics
Did the 2026 study show that ADHD causes NRS 9-10 pain?
No. It showed that ADHD screening was more common in the NRS 9-10 subgroup (27.4%) than in the NRS < 9 subgroup (16.1%), and that the unadjusted ADHD odds ratio for NRS 9-10 pain was 1.96.
Causation is not established because the study was cross-sectional.
Why did the ADHD odds ratio shrink after adjustment?
The full model added education, anxiety/depression, insomnia, catastrophizing, and pain self-efficacy. Once those variables entered, ADHD fell from OR 1.96 unadjusted to OR 1.12 fully adjusted, while catastrophizing remained much stronger at OR 5.32.
That suggests ADHD may matter partly through emotional and cognitive pain pathways rather than as an independent pain-intensity driver.
Should a chronic-pain patient ask for ADHD screening?
It is reasonable when pain has persisted despite standard care and there is a lifelong history of inattention, disorganization, impulsivity, emotional volatility, or trouble following multi-step treatment plans. A screen is only a first step; diagnosis still requires clinical evaluation.
Why did ASD not show the same pain-intensity pattern?
ASD screening was uncommon (4.4% overall), and the NRS 9-10 comparison was not statistically significant after correction (p = 0.32). AQ scores did correlate with catastrophizing as a continuous measure, so ASD-related traits may still influence pain interpretation, function, or distress without showing a clear NRS-intensity gradient in this sample.
Would ADHD medication be a pain treatment here?
Not as a stand-alone pain treatment. The study supports recognizing and treating comorbid ADHD when it is present, while continuing standard chronic-pain care.
Medication decisions should follow an ADHD diagnosis and risk assessment, not an NRS score alone.
References
- Attention-deficit/hyperactivity disorder and autism spectrum disorder in chronic pain: a study in Japanese pain centers. Kasahara S, Aono S, Takatsuki K, Niwa SI, Yabuki S. Scientific Reports. 2026;16:10544. doi:10.1038/s41598-026-45300-y
- ADHD symptoms and pain among adults in England. Stickley A, Koyanagi A, Takahashi H, Kamio Y. Psychiatry Research. 2016;246:326-331. doi:10.1016/j.psychres.2016.10.004
- Correlation between attention deficit/hyperactivity disorder and chronic pain: a survey of adults in Japan. Kasahara S, Yoshimoto T, Oka H, Sato N, Morita T, Niwa SI, Uchida K, Matsudaira K. Scientific Reports. 2025;15:13165. doi:10.1038/s41598-025-95864-4
- Associations between chronic pain and attention-deficit hyperactivity disorder (ADHD) in youth: a scoping review. Battison EAJ, Brown PCM, Holley AL, Wilson AC. Children. 2023;10(1):142. doi:10.3390/children10010142
- Autistic traits and attention-deficit hyperactivity disorder symptoms associated with greater pain interference and depression, and reduced health-related quality of life in children with chronic pain. Wiwe Lipsker C, Hirvikoski T, Balter LJT, Bolte S, Lekander M, Holmstrom L, Wicksell RKW. Frontiers in Neuroscience. 2021;15:716887. doi:10.3389/fnins.2021.716887
- The World Health Organization Adult ADHD Self-Report Scale (ASRS): a short screening scale for use in the general population. Kessler RC, Adler L, Ames M, Demler O, Faraone S, Hiripi E, et al. Psychological Medicine. 2005;35(2):245-256. doi:10.1017/S0033291704002892
- Innovative therapeutic strategies using ADHD medications tailored to the behavioral characteristics of patients with chronic pain. Kasahara S, Takahashi M, Suto T, Morita T, Obata H, Niwa SI. Frontiers in Pharmacology. 2025;16:1500313. doi:10.3389/fphar.2025.1500313