
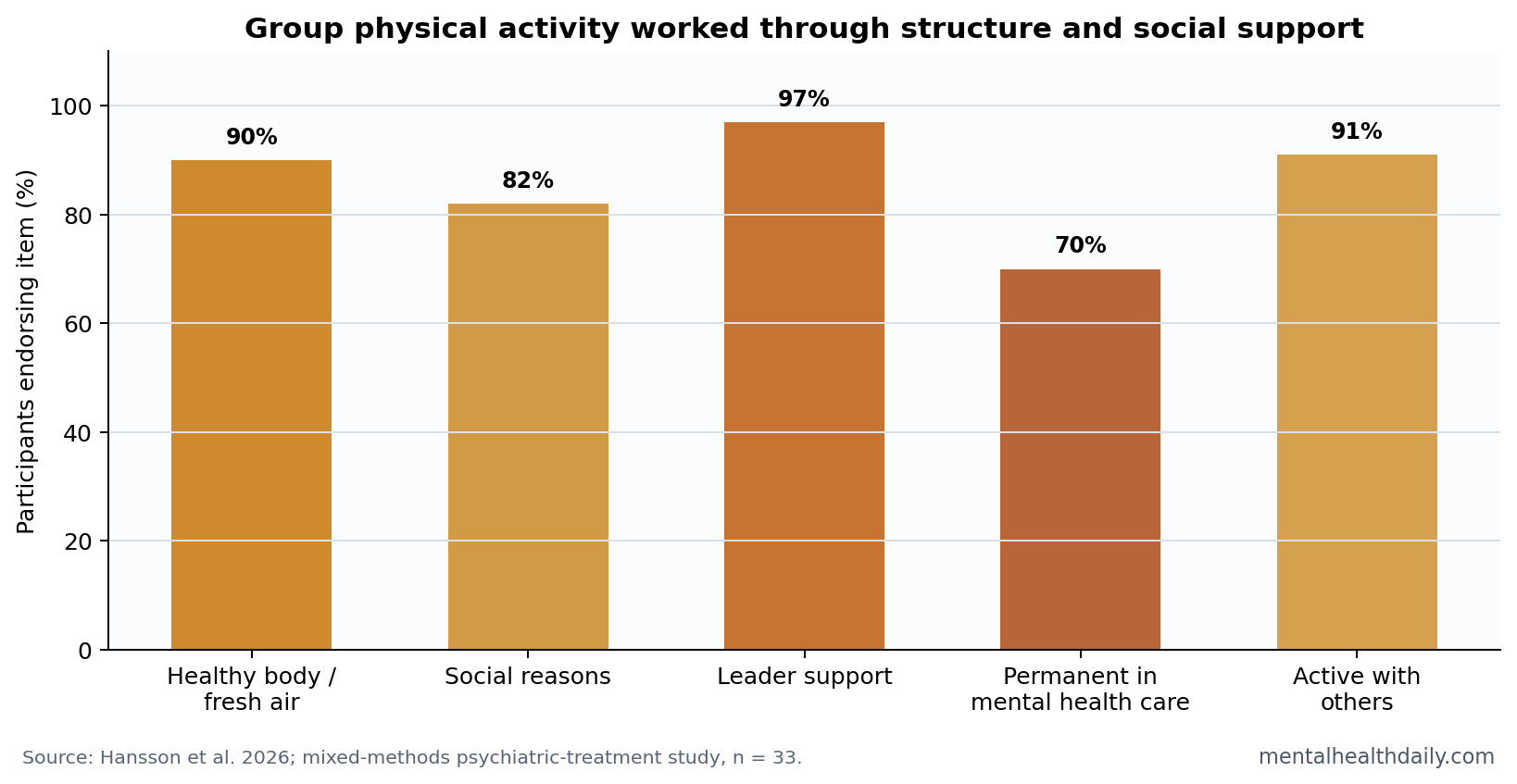
A 2026 mixed-methods study of group physical activity inside psychiatric treatment found that 90% of participants joined to have a healthy body and get fresh air, 97% felt supported by activity leaders, and 91% wanted to stay active with others after treatment.1 The useful message is not “tell people with severe mental illness to exercise”; it is that exercise programs need structure, trusted leaders, and a transition plan.
Research Highlights
- Participants valued the program: In 33 adults receiving psychiatric treatment, 90% joined to have a healthy body and get fresh air, and 82% named social reasons.1
- Perceived effects were strong: Mean positive-effect ratings were 7.9/10 for physical health and 7.7/10 for mental health.1
- Leaders were central: 97% agreed that they felt supported by activity leaders, and participants missed an average of 0.9 sessions per month.1
- Physical activity belonged in care: 70% believed activity should be a permanent part of mental health care services.1
- Maintenance needed social support: 91% wanted to stay active with others, but interviews showed weak concrete plans for sustaining activity after treatment.1
Severe mental illness usually refers to conditions such as schizophrenia spectrum disorders, bipolar disorder, and severe recurrent mood disorders that can disrupt work, relationships, daily routines, and physical health. Exercise evidence is strongest when physical activity is treated as a care process, not as a motivational slogan.
Hansson et al. studied a real psychiatric-treatment program where participants attended 1 to 4 sessions per week, including hiking, swimming, endurance training, and strength work.1
33 Adults Described Exercise as Routine, Belonging, and Support
The study used a qualitative-driven mixed-methods design: 8 active participants completed in-depth interviews and questionnaires, while 25 occasional participants completed questionnaires only. The full questionnaire sample was 33 adults, and more than half of the interview sample had a schizophrenia spectrum disorder.1
Mixed-methods means the study combined interviews with structured questionnaire data. Here, interviews explained how participants experienced the program, while questionnaire results checked whether those themes appeared in a broader group.
Activity Leaders Were Not a Peripheral Detail
The most operational finding was leader support. Nearly all participants, 97%, agreed that they felt supported by activity leaders. Interviews described leaders as motivators who created safety, cohesion, and a team feeling.1
That helps explain why simple referral lists often fail. A person with medication-related fatigue, poor sleep, low motivation, social unease, and weight gain may not benefit from being handed a list of gyms. The program’s structure reduced the distance between intention and action.
Implementation implication: in severe mental illness, exercise support needs appointment structure, familiar leaders, social safety, and flexible activities. Advice without logistics is underpowered.
This is where psychiatric exercise programs differ from generic wellness classes. The program has to absorb missed sessions, symptom fluctuation, anxiety about groups, and medication effects without turning attendance into a moral test. A skilled leader can keep expectations steady while making participation feel possible.
Activity choice also matters. Hiking, swimming, endurance work, and strength training do different things for confidence, fatigue, social contact, and body image. A program that offers only one format may accidentally exclude people whose symptoms, medications, or shame make that format hard to tolerate.
Intensity should be flexible for the same reason. A person recovering from psychosis, depression, mania, or heavy medication changes may need a low-friction entry point before endurance or strength goals make sense. Early success can be as simple as showing up, walking with the group, and returning the next week.
Clinical design: the safest program logic is stepped participation. Start with social presence and routine, then build volume and intensity as confidence, sleep, medication tolerance, and physical conditioning improve.
Medication Side Effects and Fatigue Were Real Barriers
Participants described medication-related fatigue and weight gain as barriers to being active. Other barriers included poor sleep, fluctuating motivation, seasonal conditions, practical scheduling problems, and discomfort with illness-defined group identity.1
Those barriers are not excuses. They are treatment-design constraints. Many antipsychotics and mood stabilizers can increase sedation, appetite, weight, and cardiometabolic risk. If the program ignores those realities, it will overselect for people already able to exercise despite them.
- Medication burden: fatigue and weight gain can reduce energy before exercise begins.
- Sleep instability: poor sleep can make scheduled activity feel impossible.
- Motivation swings: symptoms and medication effects can make attendance inconsistent.
- Stigma: a group defined by illness can support belonging for some people and feel labeling for others.
Follow-Up After Treatment Was the Weak Link
The transition problem was sharp. Many participants wanted to keep exercising, but interviews showed limited concrete plans and low confidence about maintaining activity alone. A simple list of community options was often not enough.1
Questionnaire data showed that 63.6% knew about alternatives, but 91% wanted to be active with others. That pattern explains why knowledge alone did not solve the transition problem. The missing piece was supported continuity.
Physical activity in psychiatric care therefore has 2 jobs: create activity during treatment and build a bridge to activity after treatment. The second job may be the harder one.
A stronger discharge pathway would identify a specific community group, confirm transportation, introduce the person to a future contact, and schedule the first post-treatment activity before the hospital-based program ends. The study’s social-support findings make that kind of handoff more defensible than a printed list.
Program design: severe-mental-illness exercise support should treat continuity as part of the intervention. Without continuity, benefits can remain trapped inside the treatment setting.
Handoff detail: continuity should be operational, not inspirational. A discharge plan can name the next activity, day, time, location, contact person, transportation route, and backup option for a bad-symptom day. That level of specificity fits the study’s finding that 91% wanted activity with others even when many already knew alternatives existed.1
The study also helps explain why exercise trials can look better than real-world advice. Trials often provide contact, structure, monitoring, and repeated encouragement. Ordinary clinical advice often gives a recommendation without the scaffolding that made the trial feasible.
For psychiatric services, the implementation target is therefore concrete: make physical activity an attended, supported, repeatable care option. When the service ends, transfer the support system rather than assuming motivation will carry itself.
Exercise Advice Works Better When It Becomes a Service
Severe mental illness often disrupts planning, energy, sleep, and social confidence. Those are exactly the functions a person needs to find an exercise option, arrive consistently, tolerate discomfort, and return after a missed session.
A service can compensate for those weak points. Scheduled sessions reduce planning load. Leaders reduce uncertainty. Group familiarity reduces social threat. Follow-up reduces the chance that a missed week becomes a permanent dropout.
That is the operational lesson from the Hansson study. Physical activity belongs in psychiatric care when the care system supplies the structure that symptoms and side effects often erode.
Measurement should follow that service logic. Future studies should track attendance, missed-session recovery, transition success, physical health, symptoms, and whether participants stay active 3 to 6 months after discharge. Symptom scales alone would miss the implementation problem this study exposed.
That follow-up window is where care design succeeds or fails.
The program is strongest when routine becomes portable.
Adjacent Exercise Evidence Supports the Direction, Not the Exact Program
Exercise evidence in severe mental illness is not limited to this small implementation study. Ashdown-Franks et al. published consensus guidance on physical activity in severe mental illness, Dauwan et al. meta-analyzed exercise effects across mental disorders, and Firth et al. summarized broad physical-activity evidence for depression, anxiety, and distress.234
The Hansson study adds patient-side implementation detail. It shows why a program can be liked and still fail after discharge if follow-up is weak. The exercise itself is only part of the intervention; leader support, social belonging, and continuity planning are part of the active system.
Evidence-strength note: this was an experience and implementation study, not a symptom-efficacy trial. It can describe barriers, preferences, and perceived benefits. It cannot estimate how much the program reduced psychosis, depression, mania, hospitalization, or cardiometabolic risk.
That is why adjacent evidence should be used carefully. Meta-analyses and consensus guidance support physical activity as a serious treatment-support target in severe mental illness, but Hansson et al. add a different layer: what participants said made attendance possible. The practical synthesis is service design first, then exercise prescription.
That order matters for implementation. A perfect exercise recommendation fails if the person cannot get there, feels unsafe in the group, or stops after the first missed session. A modest activity plan with reliable leader contact may do more useful work than an ambitious plan that assumes stable energy, transport, and confidence.
Questions About Exercise Programs in Severe Mental Illness
Did this study prove exercise treats schizophrenia or bipolar disorder?
No. It studied experiences with a physical-activity program inside psychiatric treatment, not symptom reduction in a randomized trial.
What was the clearest implementation signal?
Leader support. The 97% support figure and interview themes both pointed to trusted leaders as a major reason participants could attend.
What should programs fix first?
Follow-up. Participants wanted social activity after treatment, but many lacked concrete plans and support for making that transition.
References
- Hansson G, et al. Mind in motion: patients’ experiences with group-based physical activity in psychiatric treatment – a mixed-methods study. BMC Psychiatry. 2026. https://doi.org/10.1186/s12888-026-08117-7
- Stubbs B, et al. EPA guidance on physical activity as a treatment for severe mental illness: a meta-review of the evidence and Position Statement from the European Psychiatric Association. European Psychiatry. 2018. https://pubmed.ncbi.nlm.nih.gov/30257806/
- Dauwan M, Begemann MJH, Heringa SM, Sommer IE. Exercise improves clinical symptoms, quality of life, global functioning, and depression in schizophrenia: a systematic review and meta-analysis. Psychological Medicine. 2016. doi:10.1017/s0033291716001732
- Singh B, et al. Effectiveness of physical activity interventions for improving depression, anxiety and distress: an overview of systematic reviews. British Journal of Sports Medicine. 2023. https://pubmed.ncbi.nlm.nih.gov/36796860/