
A 2026 review in the Japanese Journal of Radiology argued that amyloid PET has moved from an optional Alzheimer’s disease biomarker to a practical eligibility gate for anti-amyloid antibody therapy, while tau PET and FDG-PET answer different questions in the same clinical workflow.1 The key shift is not that every memory complaint needs PET; it is that disease-modifying therapy makes biological confirmation harder to skip.
Research Highlights
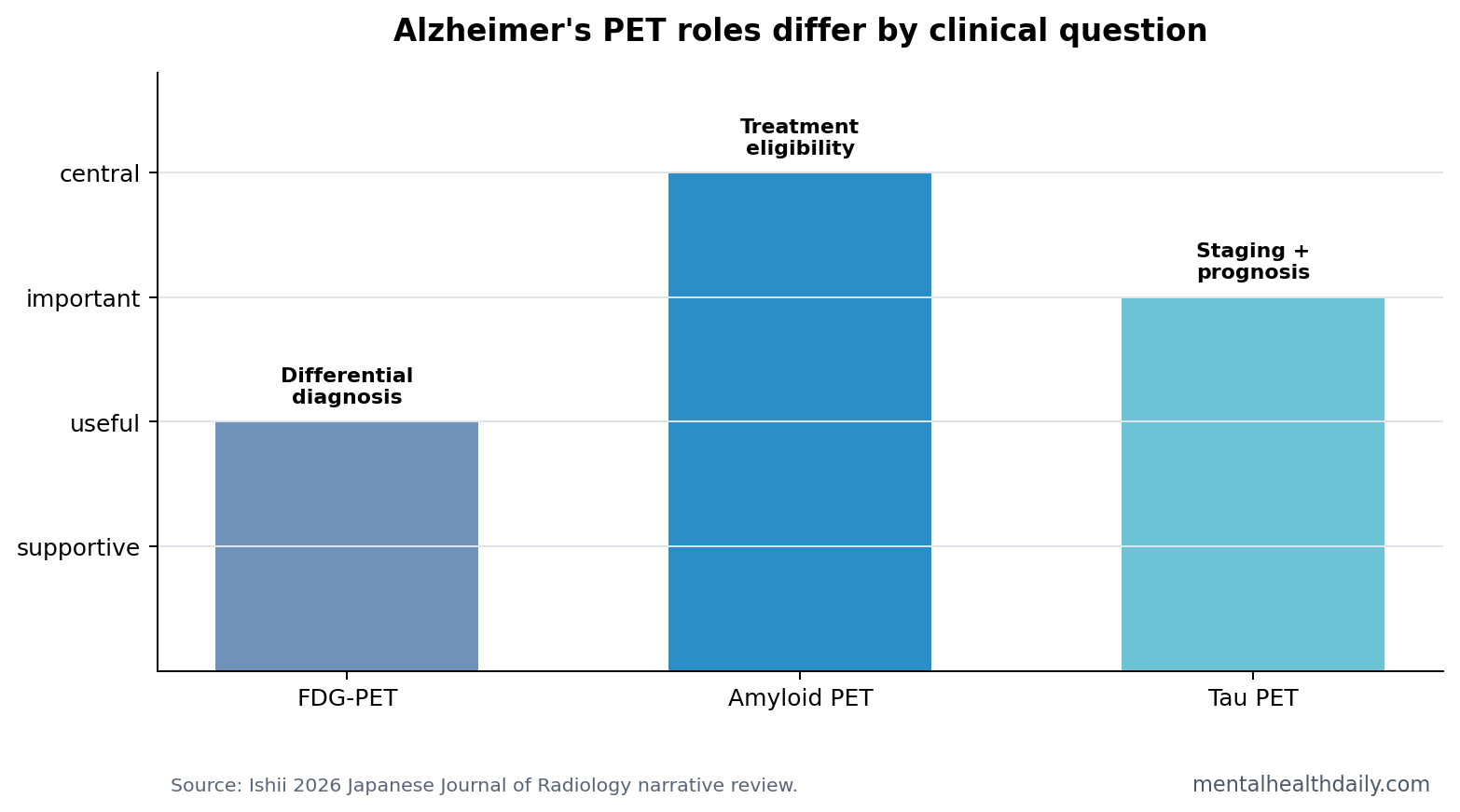
- 3 PET roles now separate: FDG-PET supports differential diagnosis, amyloid PET confirms amyloid positivity, and tau PET adds disease-stage and prognosis information.1
- 2 anti-amyloid therapies changed the workflow: lecanemab and donanemab made biomarker-confirmed Alzheimer’s disease more operationally important before treatment.1
- Amyloid PET is the treatment gate: the review describes amyloid PET as essential for confirming eligibility before anti-amyloid antibody therapy.1
- Tau PET is not the same test: tau PET maps neurofibrillary pathology and correlates more closely with severity and progression than amyloid burden alone.1
- Screening remains inappropriate: PET should answer 1 defined clinical question, with broad population or wellness testing left outside the review’s clinical frame.
Positron emission tomography (PET) is a molecular-imaging method that tracks a radiotracer in the brain. In Alzheimer’s disease, different tracers can show glucose metabolism, amyloid-β plaque burden, or tau pathology. Those are related but not interchangeable biological signals.
Anti-amyloid antibodies such as lecanemab and donanemab target amyloid biology rather than only treating symptoms. That makes the diagnostic standard stricter: treating someone without confirming amyloid positivity exposes the person to cost and adverse-event risk without clear biological rationale.
Amyloid PET Confirms Whether Anti-Amyloid Therapy Is Biologically Plausible
Ishii’s review places amyloid PET at the center of the current treatment-selection problem. Amyloid PET visualizes cerebral amyloid-β deposition, which is the pathology that anti-amyloid monoclonal antibodies are designed to reduce.1
Eligibility logic: if amyloid PET is negative, the patient may still have cognitive impairment, but the rationale for amyloid-removing therapy is weak. If amyloid PET is positive, the treatment question can move to disease stage, symptom severity, comorbidity, safety monitoring, and patient preference.
Lecanemab and donanemab trials both used biomarker-selected Alzheimer’s populations, making the imaging question more concrete than older diagnostic debates.2,3
Tau PET Adds Staging and Prognosis, Not a Duplicate Amyloid Answer
Tau PET measures the spread of tau neurofibrillary pathology. Tau burden tends to sit closer to current clinical severity and future progression than amyloid positivity alone, because amyloid can be present before symptoms are advanced.1
That distinction changes how PET results should be explained. Amyloid PET asks whether the disease biology needed for anti-amyloid treatment is present. Tau PET asks how far the disease process has moved through the brain and how aggressive the clinical trajectory may be.
FDG-PET Still Helps Differential Diagnosis
FDG-PET measures regional glucose metabolism, a proxy for neuronal activity. It does not directly show amyloid plaques or tau tangles. Its value is pattern recognition: Alzheimer’s disease, frontotemporal dementia, dementia with Lewy bodies, and other neurodegenerative syndromes can produce different hypometabolic patterns.
That makes FDG-PET supportive rather than definitive for anti-amyloid treatment. It can sharpen the differential diagnosis when symptoms and MRI leave uncertainty, but it cannot replace amyloid confirmation for a drug that targets amyloid biology.
Appropriate-Use Criteria Limit the PET Expansion
The review emphasizes appropriate-use criteria and guideline interpretation. That guardrail is necessary because a positive amyloid scan can be misread. Amyloid positivity is common in older adults and does not automatically prove that every symptom is caused mainly by Alzheimer’s disease.
- Good use: early symptomatic cognitive decline where the result will change diagnosis, treatment eligibility, or counseling.
- Weak use: low-risk screening, vague memory worry without objective impairment, or testing when no treatment or management decision depends on the answer.
- Safety context: anti-amyloid therapy also requires MRI monitoring and risk discussion because amyloid-related imaging abnormalities can occur.
Narrative Review Limits
Evidence-strength note: Ishii’s paper is a narrative review, not a new randomized trial or quantitative meta-analysis. It is strongest as an implementation synthesis: which PET modality answers which clinical question now that anti-amyloid therapy exists.
Local constraints still matter. PET access, tracer availability, reader expertise, reimbursement, and national treatment rules vary. A clean conceptual algorithm can become uneven in real clinics if the scan is unavailable, delayed, or interpreted without dementia-specialist context.
Blood Tests May Triage, but PET Still Anchors Hard Cases
Blood biomarkers are changing Alzheimer’s workups quickly. Plasma p-tau217, p-tau181, glial fibrillary acidic protein, and neurofilament light can help triage who is likely to have Alzheimer’s biology and who needs confirmatory testing. For many clinics, blood testing may become the first filter because it is cheaper, faster, and easier to repeat than PET.
PET still has a role when the decision carries high consequence. Anti-amyloid therapy is expensive, requires infusion infrastructure, and can cause amyloid-related imaging abnormalities. A direct brain amyloid test can be valuable when blood results are borderline, symptoms are atypical, comorbid brain disease is present, or treatment eligibility depends on a clear biological answer.
Clinical sequence: a practical pathway may use cognitive assessment and MRI first, blood biomarkers as a triage layer, amyloid PET or cerebrospinal fluid testing for confirmation, and tau PET when staging or prognosis would change counseling or trial enrollment. Ishii’s review fits that sequence because it treats PET as question-specific imaging rather than a single universal dementia test.
Why sequence matters: each extra test should reduce a specific uncertainty. If MRI already shows another dominant explanation, amyloid PET may not change the decision.
If blood biomarkers are strongly positive but symptoms are atypical, PET or cerebrospinal fluid testing can help confirm whether Alzheimer’s biology is actually present. If amyloid status is already known, tau PET should be reserved for staging, prognosis, or trial selection rather than repeated confirmation of the same disease label.
Access problem: this workflow is easier to describe than to deliver. PET capacity, tracer availability, insurance coverage, dementia-specialist interpretation, and infusion-center access can all become bottlenecks. That makes the review’s modality separation practical: clinics with limited PET access need to reserve scans for decisions where the result changes treatment eligibility, risk counseling, or diagnostic direction.
Scarce imaging should answer the highest-stakes question first.
PET Results Need Symptom-Level Interpretation
Amyloid positivity can coexist with vascular disease, Lewy body disease, depression, sleep apnea, medication effects, or normal-pressure hydrocephalus. In older adults, mixed pathology is common. The scan result therefore needs to be interpreted alongside the clinical syndrome.
Positive amyloid PET: Alzheimer’s pathology is present. The clinician still needs to ask whether that pathology explains the current symptoms and whether the patient is in the treatment window targeted by anti-amyloid trials.
Negative amyloid PET: Alzheimer’s disease becomes less likely as the main cause of cognitive impairment. That result can redirect the workup toward frontotemporal dementia, Lewy body disease, vascular cognitive impairment, psychiatric causes, medication effects, sleep disorders, or other neurological conditions.
Tau PET pattern: widespread neocortical tau generally carries a different prognosis from minimal or medial-temporal-limited tau. That is why tau PET may be most useful when family counseling, progression risk, or trial selection is the clinical pressure point.
Anti-Amyloid Therapy Makes False Positives More Costly
Older Alzheimer’s diagnostic uncertainty often led to symptomatic treatment, monitoring, and caregiver planning. Disease-modifying therapy changes the risk calculation. A false-positive biological assignment can expose someone to treatment burden without a plausible target. A false-negative assignment can keep an eligible patient away from a therapy they might reasonably consider.
That is the practical reason PET interpretation standards matter. The scan governs access to a treatment class whose benefits, risks, monitoring demands, and costs are substantial.
What Patients Should Hear From the Imaging Result
The reader-facing explanation should be concrete. A positive amyloid PET means amyloid plaques are present in the brain. It does not automatically mean treatment is indicated, because disease stage, symptom pattern, bleeding risk, anticoagulant use, MRI findings, age, frailty, and goals of care still shape the decision.
A tau PET result adds a different kind of information. Minimal tau can support an earlier-stage disease interpretation; widespread tau can signal a more advanced process with different prognosis. FDG-PET, meanwhile, can help when the clinical picture could be Alzheimer’s disease, frontotemporal dementia, dementia with Lewy bodies, vascular disease, or another cause of cognitive decline.
That layered explanation is more honest than telling patients that PET simply “confirms Alzheimer’s.” The modality, tracer, clinical question, and treatment plan all determine what the scan result means.
Questions About Alzheimer’s PET
Is amyloid PET the same as an Alzheimer’s diagnosis?
No. Amyloid PET confirms amyloid pathology. Diagnosis still needs the clinical syndrome, alternative explanations, disease stage, and whether the result fits the patient’s symptoms.
Why not use blood biomarkers instead?
Blood biomarkers such as plasma p-tau217 are becoming powerful triage tools, but PET can still provide direct brain-pathology confirmation, especially when treatment eligibility, uncertain diagnosis, or discordant results are involved.
When does tau PET help most?
Tau PET is most useful when disease stage and prognosis are the main question. It can show whether pathology is limited or already widespread, which may affect counseling and trial eligibility.
References
- Ishii K. Brain PET in the era of anti-amyloid-β antibody therapy. Japanese Journal of Radiology. 2026. doi:10.1007/s11604-026-01998-4
- van Dyck CH, Swanson CJ, Aisen P, et al. Lecanemab in early Alzheimer’s disease. New England Journal of Medicine. 2023. doi:10.1056/nejmoa2212948
- Sims JR, Zimmer JA, Evans CD, et al. Donanemab in early symptomatic Alzheimer’s disease. JAMA. 2023. doi:10.1001/jama.2023.13239
- Rabinovici GD, et al. Appropriate use criteria for amyloid and tau PET in Alzheimer’s disease. PubMed