Some sleep apnea patients stay sleepy even when their CPAP is used 6+ hours a night and apnea events have been driven back to normal range. A 2026 cross-sectional study of 65 PAP-adherent adults found those residually sleepy patients performed measurably worse on global cognition, memory, executive function, attention, and processing speed than their well-rested peers.1
Research Highlights
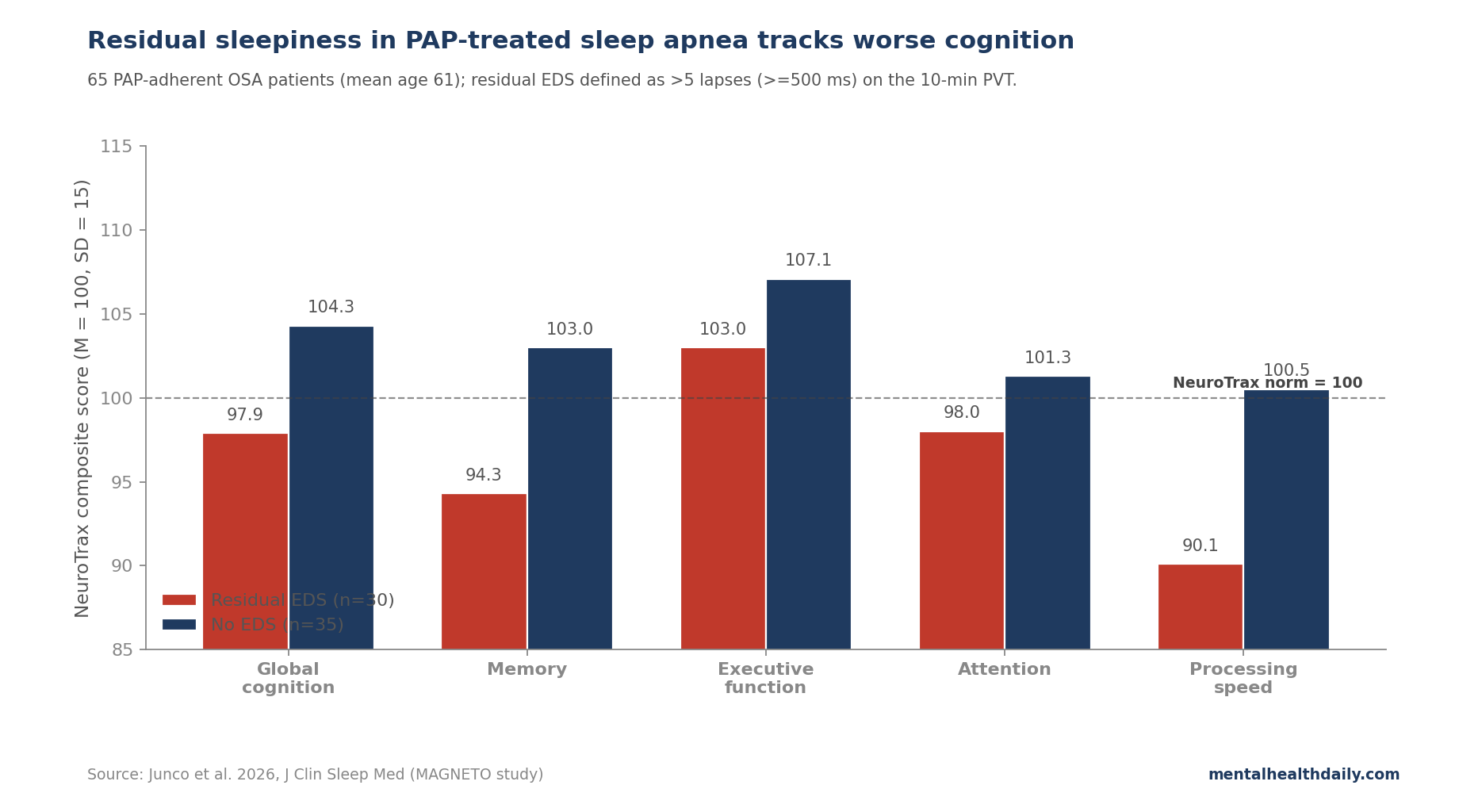
- 46% of PAP-adherent OSA patients had residual daytime sleepiness on objective testing. Junco et al. enrolled 65 adults using positive airway pressure (PAP) at least 6 hours per night with normalized apnea-hypopnea index (AHI < 5 events/hour). 30 of 65 met objective criteria for excessive daytime sleepiness on the Psychomotor Vigilance Task (PVT) — a 10-minute reaction-time test where >5 lapses of 500 ms or longer marks impaired alertness.1
- Subjective sleepiness scales did not match. Mean Epworth Sleepiness Scale scores were similar in both groups, and the correlation between Epworth and objective PVT lapses was essentially zero (Spearman’s rho = 0.021, p = 0.876). Patients self-reporting normal alertness can still be objectively impaired.1
- Higher PVT lapse counts tracked poorer cognition across every domain tested. Adjusted regression: lapses vs. global cognition β = −4.09, p < 0.001; memory β = −3.97, p = 0.001; executive function β = −3.91, p = 0.004; attention β = −2.68, p = 0.036; processing speed β = −4.89, p = 0.012. Effects survived false-discovery-rate correction across cognitive outcomes.1
- The between-group cognitive gap was clinically meaningful. Residual-EDS patients scored 0.43–0.58 NeuroTrax standard deviations lower on global cognition (mean difference 6.4 points) and memory (8.8 points), comparable to 1–2 points on standard cognitive screens like the MoCA or MMSE.1
- Cross-sectional and exploratory. 65 patients, single site, mostly Hispanic, no causal claim. The design supports a residual-EDS cognitive risk phenotype hypothesis, not a clinical diagnostic algorithm.
Obstructive sleep apnea (OSA) is the repeated upper-airway collapse during sleep that drives intermittent hypoxemia, sleep fragmentation, and sympathetic activation. CPAP and bilevel PAP machines treat the breathing events directly — the AHI usually drops to normal range — but a meaningful subset of patients keep complaining of daytime sleepiness anyway.2
Estimates of how big that subset is depend on which sleepiness measure is used. On the self-report Epworth Sleepiness Scale, 22–34% of PAP-adherent OSA patients endorse residual sleepiness. On objective wake-test paradigms (the Maintenance of Wakefulness Test or Multiple Sleep Latency Test), the figure rises to 65%. The disagreement is the clinical problem: patients who feel fine may still be objectively impaired.1
Why PVT Is the Practical Tool
The Psychomotor Vigilance Task (PVT) is a 10-minute reaction-time test in which a stimulus appears at random intervals and the participant presses a key as fast as possible. The standard scoring tallies lapses — reaction times of 500 ms or longer — and the mean reaction time.
The test is sensitive to acute and chronic sleep loss, hypoxemia, and circadian disruption, and is widely used in transportation safety, military operations, and sleep medicine research.3
It has 2 advantages over MWT/MSLT for clinical use. First, it takes 10 minutes versus the day-long sleep-latency protocols. Second, it does not depend on language, education, or cultural context, which made it usable in this study’s 72% Hispanic sample without translation issues.
Junco et al. used >5 lapses as the cutoff for residual EDS, in line with prior OSA research linking PVT lapses to nocturnal hypoxemia severity.4
The Cohort: PAP-Adherent, Real-World OSA
Participants were 65 adults aged 40+ with mild to severe OSA, all using PAP at least 6 hours per night for at least 6 months, with device-reported normalized AHI < 5 events/hour. Mean baseline diagnostic AHI was 38, and 49% had been diagnosed as severe.
Cognitive testing used the NeuroTrax computerized battery, normalized for age and education, covering 5 composite domains: global cognition, memory (verbal and non-verbal, immediate and delayed), executive function (Go/No-Go, Stroop, Catch Game), attention (Stroop, Staged Information Processing), and information processing speed.
Exclusions were heavy and clinically reasonable: prior stroke, coronary artery disease, heart failure, arrhythmia, COPD, dementia, narcolepsy, sedating medications. The sample is therefore an unusually clean OSA-with-PAP-adherence-and-no-cardiovascular-comorbidity slice — less generalizable to typical sleep clinic populations, but a stronger test of whether residual sleepiness alone tracks cognition.
The Cognitive Gradient: More PVT Lapses, Worse Performance
Robust generalized linear models, adjusted for sex, time since OSA diagnosis, and self-reported sleep duration, found PVT lapses associated with worse performance on every domain tested. The largest effect was on processing speed (β = −4.89, p = 0.012); the most robust by FDR-corrected p-value was global cognition (β = −4.09, p < 0.001).1
Mean reaction time on the PVT, used as an alternative continuous index, gave a similar pattern: longer RT was associated with poorer global cognition, memory, executive function, and processing speed. Reaction-time variability (the within-task SD/mean ratio) was not independently associated with cognition after FDR correction — suggesting it is the frequency and depth of attentional lapses, not response noise per se, that tracks the cognitive deficit.
Categorical analysis using the >5-lapse cutoff produced cleaner clinical anchors:
- Global cognition: EDS group mean 97.9 (SD 11.7) vs. no-EDS 104.3 (SD 7.7), F = 4.79, p = 0.033, partial η² = 0.07.
- Memory: EDS 94.3 (SD 12.7) vs. no-EDS 103.0 (SD 7.5), F = 10.43, p = 0.002, partial η² = 0.14.
- Adjusted mean differences: 6.4 NeuroTrax points for global cognition, 8.8 for memory — roughly 0.43–0.58 of a NeuroTrax SD, comparable to 1–2 points on a standard cognitive screen.1
That magnitude is not catastrophic. It is also not nothing, particularly on memory, where 0.58 SD is in the range of effects routinely cited in mild cognitive impairment screening trials.
The Subjective-Objective Disconnect Is the Clinical Punchline
The Epworth Sleepiness Scale, the standard clinic questionnaire (8 items, scored 0–24, >10 typically marks excessive sleepiness), did not separate the EDS and no-EDS groups in this sample. Both groups averaged below the conventional Epworth cutoff. The Spearman correlation between Epworth and PVT lapses was 0.021 (p = 0.876).1
This replicates a long-standing finding in OSA: self-report and objective sleepiness measures often diverge, especially in patients who have spent years with chronic partial sleep deprivation and may have recalibrated their internal sense of “normal alertness.” Pepin et al. 2009 made similar observations comparing Epworth scores to objective wake tests in PAP-treated OSA cohorts.5
The implication for clinical practice is real but easy to overstate. A PAP-adherent patient who scores well on the Epworth may still be objectively impaired; a PAP-adherent patient who scores poorly on the Epworth may be fine on the PVT. Neither test is a perfect substitute for the other, but pairing them improves phenotyping.
Why Residual Sleepiness Might Be a Cognitive-Risk Phenotype
Dementia risk gives the residual-sleepiness finding its longer clinical horizon. Sleep-disordered breathing and excessive daytime sleepiness have been associated with elevated dementia incidence in multiple longitudinal cohorts:
- Yaffe et al. 2011 followed 298 older women without dementia and found that sleep-disordered breathing roughly doubled the odds of mild cognitive impairment or dementia 5 years later (adjusted OR around 1.85).6
- Bubu et al. 2017 meta-analyzed 27 studies and reported that OSA was associated with elevated risk of cognitive impairment, particularly in attention and executive domains.7
- Jaussent et al. 2012 followed 4,894 older French adults and found that baseline excessive daytime sleepiness independently predicted incident all-cause dementia and faster cognitive decline over 8 years.8
The mechanistic candidates include intermittent hypoxemia (which the PAP machine has corrected on average but may not fully reverse the structural sequelae of), sleep fragmentation, glymphatic-clearance disruption, and chronic systemic inflammation. The Junco study cannot distinguish among these because it is cross-sectional, but the clinical signal — that PAP adherence with normalized AHI does not guarantee normal cognition — is consistent with all of them.
Sleep Clinics Need More Than PAP Adherence and Epworth Scores
- Adherence does not equal full treatment. A patient using PAP >6 hours per night with AHI < 5 has done their part and the device has done its part, but a substantial fraction will still have residual cognitive risk worth screening for.
- Don’t rely on Epworth alone. The standard clinic questionnaire missed nearly half of objectively impaired patients in this sample. Pairing it with a 10-minute PVT is feasible and adds information.
- Pharmacological options exist for residual EDS. Solriamfetol (Sunosi) and pitolisant (Wakix) are FDA-approved for excessive daytime sleepiness in PAP-treated OSA and have RCT evidence of improvement on objective wakefulness tests.9 They do not directly address cognition, but treating residual EDS is plausibly upstream of the cognitive trajectory.
- Look for treatable contributors. Concurrent depression, hypothyroidism, restless legs, periodic limb movements, sedating medications, alcohol use, and other sleep disorders all present as residual sleepiness on PAP and can be addressed.
Limitations of This Analysis
It is cross-sectional and exploratory. The 65-person sample, recruited at 1 university sleep center, was designed as hypothesis-generating, not as a definitive clinical study. Causal claims require longitudinal data tracking PAP-adherent patients with and without residual EDS over years for cognitive trajectories.
Sample size limits subgroup analysis. 30 vs. 35 patients across 5 cognitive domains is enough to detect moderate effects after FDR correction but underpowered for finer phenotyping (e.g., who is most at risk, which OSA severity stratum benefits most from PVT screening).
Selection bias toward healthy OSA patients. Heavy exclusions (no prior stroke, no coronary artery disease, no heart failure, no COPD, no narcolepsy, no sedating medications) make this cohort cleaner than typical clinic populations. Real-world PAP-adherent patients carry more comorbidity, which both confounds the association and may make it stronger.
Mostly Hispanic, single-site. 72% Hispanic, 6% Black, recruited in Miami. Generalizability across populations is unknown, though the use of language-independent computerized cognitive testing (NeuroTrax, available in English and Spanish) is a strength.
Cognitive testing was 1 timepoint. The study did not measure cognitive change before vs. after PAP initiation, so it cannot distinguish residual deficits from baseline differences that predisposed to OSA in the first place. Reverse causation — that early cognitive vulnerability contributes to residual EDS — remains possible.
Self-reported sleep duration as a covariate. Subjective sleep duration is a noisy proxy for actual sleep, and uncontrolled total sleep time on the night before the cognitive test could affect both PVT and cognitive scores.
Questions About Sleep Apnea, Daytime Sleepiness, and Cognition
Does this mean my CPAP isn’t working?
Not necessarily. PAP that has driven AHI below 5 is doing its mechanical job. Residual EDS in the face of good adherence and treated AHI suggests that something else — structural sequelae of years of pre-treatment hypoxemia, a comorbid sleep disorder, depression, hypothyroidism, sedating medications — is contributing.1
Talking to a sleep physician about objective sleepiness testing, comorbidity screening, and pharmacological options is the practical next step.
Should I be worried about dementia if I have residual sleepiness?
The longitudinal evidence linking residual sleepiness to faster cognitive decline and elevated dementia risk is real but not deterministic. Yaffe et al. 2011 reported roughly doubled OR for mild cognitive impairment or dementia with sleep-disordered breathing.6
The practical takeaway is that residual sleepiness is worth treating — both for current quality of life and as a potentially modifiable risk factor, even if the size of the cognitive-protection benefit from treating it has not been established in trials.
What is solriamfetol and how does it work?
Solriamfetol (Sunosi) is a dopamine-norepinephrine reuptake inhibitor approved by the FDA in 2019 for excessive daytime sleepiness in narcolepsy and OSA. It improves objective wakefulness on the MWT in PAP-treated patients with residual EDS, with the most common side effects being headache, nausea, and decreased appetite.9
Pitolisant (Wakix) is a histamine H₃ receptor inverse agonist with a different mechanism and a similar approved indication. Modafinil and armodafinil are older options that work but had labeling concerns due to rare serious skin reactions.
Why don’t Epworth scores match objective sleepiness?
People with chronic partial sleep loss often recalibrate their sense of normal alertness. The Epworth asks how likely a person is to doze off in 8 specific situations — situations that depend on lifestyle, opportunity, and what the person considers normal. Objective tests like the PVT measure performance directly and do not depend on self-perception.1
For OSA management, the 2 measures answer different questions and ideally are used together.
Could a PVT-based screen come to my sleep clinic?
Possibly. The 10-minute PVT is portable, language-independent, and inexpensive to administer. Validated tablet versions exist. Whether sleep clinics adopt it routinely will depend on reimbursement and on whether subsequent prospective studies confirm that a positive PVT screen meaningfully changes treatment recommendations.
For now, ask your sleep specialist whether objective sleepiness testing is available if subjective questionnaires don’t match how you feel.
References
- Cognition and psychomotor vigilance in treated sleep apnea patients with and without daytime sleepiness: the MAGNETO study. Junco B et al. Journal of Clinical Sleep Medicine. 2026;22:60. doi:10.1007/s44470-026-00077-9
- Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Benjafield AV et al. Lancet Respiratory Medicine. 2019;7(8):687-698. doi:10.1016/s2213-2600(19)30198-5
- Validity and sensitivity of a brief psychomotor vigilance test (PVT-B) to total and partial sleep deprivation. Basner M, Mollicone D & Dinges DF. Acta Astronautica. 2011;69(11-12):949-959. doi:10.1016/j.actaastro.2011.07.015
- Effect of obstructive sleep apnea on neurocognitive performance: results of a meta-analysis. Stranks EK & Crowe SF. Archives of Clinical Neuropsychology. 2016;31(2):186-193. doi:10.1093/arclin/acv087
- Prevalence of residual excessive sleepiness in CPAP-treated sleep apnoea patients: the French multicentre study. Pepin JL et al. European Respiratory Journal. 2009;33(5):1062-1067. doi:10.1183/09031936.00016808
- Sleep-disordered breathing, hypoxia, and risk of mild cognitive impairment and dementia in older women. Yaffe K et al. JAMA. 2011;306(6):613-619. doi:10.1001/jama.2011.1115
- Sleep, cognitive impairment, and Alzheimer’s disease: a systematic review and meta-analysis. Bubu OM et al. Sleep. 2017;40(1):zsw032. doi:10.1093/sleep/zsw032
- Excessive sleepiness is predictive of cognitive decline in the elderly. Jaussent I et al. Sleep. 2012;35(9):1201-1207. doi:10.5665/sleep.2070
- Solriamfetol for the treatment of excessive sleepiness in OSA: a placebo-controlled randomized withdrawal study. Strollo PJ Jr et al. Chest. 2019;155(2):364-374. doi:10.1016/j.chest.2018.11.005