A 2026 NHANES analysis of 6,502 adults found that urinary 3-PBA, a pyrethroid insecticide metabolite, was modestly associated with depression risk at OR = 1.02 per 1 μg/L, while self-reported household pesticide exposure weakened after full adjustment to OR = 1.43 (95% CI 0.91 to 2.25).1 The calibrated read is biomarker signal first, causal language later.
Research Highlights
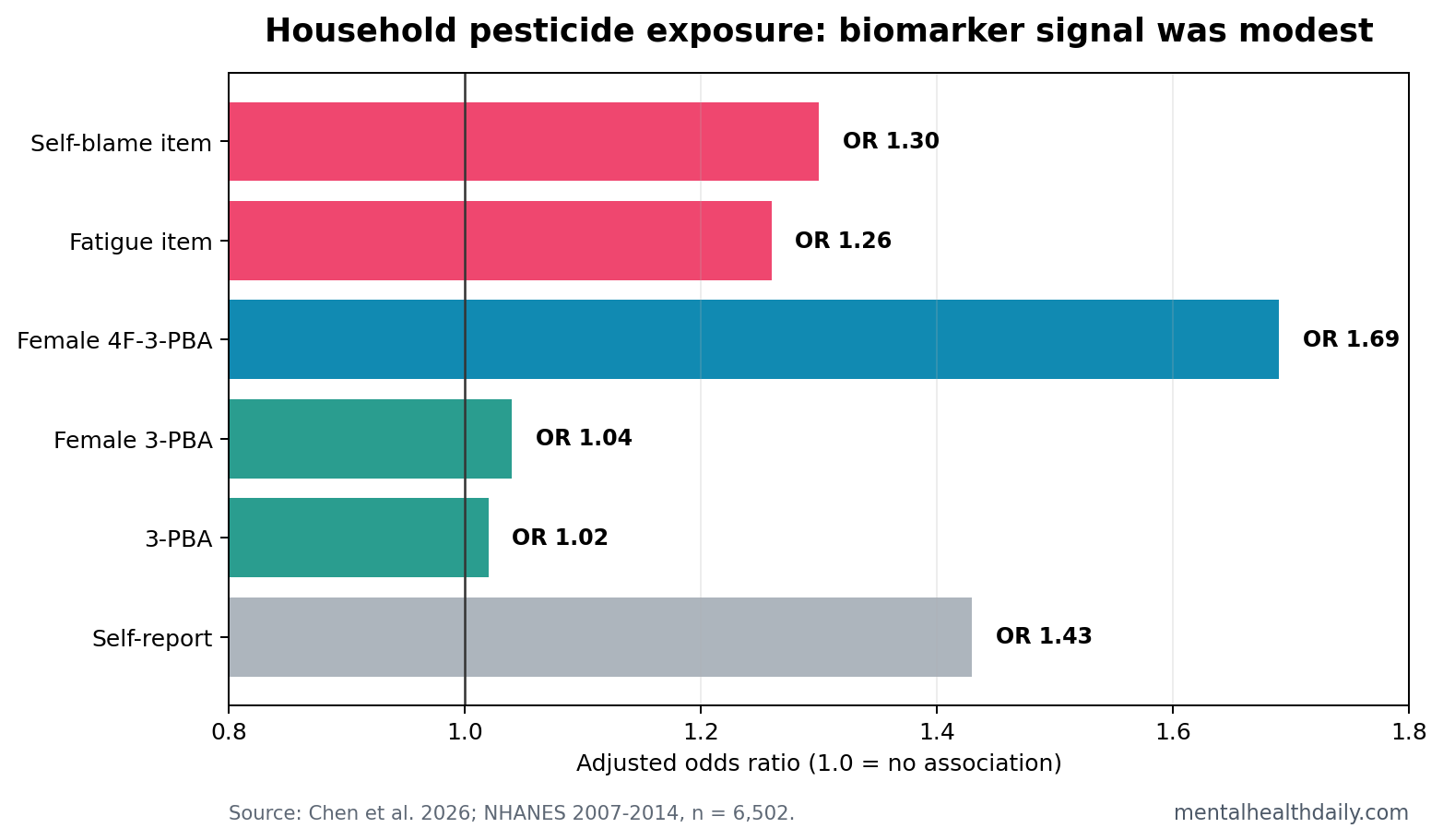
- 3-PBA carried the clearest overall signal: each 1 μg/L increase was associated with OR = 1.02 for depression (95% CI 1.00 to 1.04) after full adjustment.
- Self-report attenuated after adjustment: reported household pesticide use was OR = 1.51 before adjustment but OR = 1.43 with a 95% CI crossing 1.00 after full covariate adjustment.
- Female subgroup estimates were higher than overall estimates: female participants showed OR = 1.04 for 3-PBA and OR = 1.69 for 4F-3-PBA in subgroup models.
- Symptoms were not uniform: fatigue (OR = 1.26), self-blame (OR = 1.30), and appetite disturbance (OR = 1.17) contributed more clearly than suicidal thoughts.
- Causality remains unresolved: the 6,502-person analysis was cross-sectional, so housing conditions, pest burden, income, health behavior, and reverse causality remain serious alternatives.
3-PBA, or 3-phenoxybenzoic acid, is a urinary metabolite used as a biomarker of pyrethroid insecticide exposure. Pyrethroids are common in residential pest-control products, so 3-PBA can sometimes capture exposure more objectively than asking someone whether sprays or chemicals were used at home.
NHANES self-report was narrower than the phrase “household pesticide exposure” can sound. Participants were asked whether chemicals had been used in the past 7 days to control fleas, cockroaches, ants, termites, or other insects, while urine testing measured metabolites from insect repellents and pyrethroid insecticides.1
PHQ-9 depression in this study meant a Patient Health Questionnaire-9 score of at least 10. That threshold identifies clinically meaningful depressive symptoms; it is not the same as a structured psychiatric interview.
Urinary 3-PBA Outperformed Self-Reported Exposure
Chen et al. analyzed NHANES 2007-2014 data from adults with both urinary pesticide metabolites and valid PHQ-9 depression data.1 The final analytic sample included 6,502 adults, including 612 people classified as depressed by PHQ-9 threshold.
Self-reported household pesticide use looked elevated in simple models, but the signal attenuated after adjustment for age, sex, race, ethnicity, marital status, poverty-income ratio, education, alcohol, smoking, diabetes, hypertension, hyperlipidemia, and BMI. The fully adjusted OR was 1.43, but the 95% CI was 0.91 to 2.25.
Urinary 3-PBA held a small dose-related association. The fully adjusted model estimated OR = 1.02 per 1 μg/L. That effect size is modest, but it is biologically more anchored than a 7-day recall question about household chemical use.
Female-Specific Signals Were Stronger Than the Overall Estimate
Subgroup results sharpened the pattern. Among women, 3-PBA was associated with depression at OR = 1.04 (95% CI 1.01 to 1.07), and 4F-3-PBA was associated at OR = 1.69 (95% CI 1.18 to 2.41). The male subgroup showed different mixture weights, with DCBA contributing more in the weighted quantile sum model.
Sex-specific toxicology signals should be handled carefully. They can reflect biological vulnerability, product-use patterns, occupational context, home pest burden, housing quality, body composition, metabolism, or measurement noise. The study supports sex-stratified follow-up; it does not prove that women are biologically harmed more by every household pesticide exposure.
Symptom Links Were Somatic and Mood-Related
The symptom-item pattern was not a blanket elevation across every PHQ-9 item. Fatigue, self-blame, appetite disturbance, feeling down or hopeless, and sleep trouble showed clearer associations than suicidal thoughts or psychomotor agitation/retardation.
Practical interpretation: the biomarker signal looked more like a broad depressive-symptom burden with somatic and self-evaluative features than a specific suicidal-risk marker. That distinction protects the result from being inflated into a stronger psychiatric claim than the data support.
Prior NHANES work also linked pyrethroid metabolites with depressive symptoms and suggested that physical activity may modify the association.2 Toxicology work on 3-PBA has proposed dopaminergic and oxidative-stress mechanisms, which gives the association biological plausibility.3 Exposure-science studies linking household insecticide use with urinary 3-PBA help explain why self-report and biomarkers can diverge.4
Cross-Sectional Exposure Data Cannot Carry Causal Weight
Evidence-strength note: this was a cross-sectional biomarker study. Urine metabolites and PHQ-9 symptoms were measured in the same survey window, so the timing sequence is uncertain. Depression could change cleaning habits, housing stability, pest control, time indoors, diet, or product use.
Baseline differences also make simple causal reading risky. Compared with nondepressed participants, depressed participants were more often female (65.41% vs. 49.98%), below the poverty threshold (27.37% vs. 13.04%), current smokers (38.17% vs. 18.35%), obese (48.16% vs. 34.27%), hypertensive (49.94% vs. 34.64%), and diabetic (15.67% vs. 8.23%).1
Those patterns do not erase the 3-PBA association, but they show why household pesticide biomarkers sit inside a larger housing, health, and socioeconomic risk cluster.
Confounding is also unusually plausible. Household pesticide exposure is not random. It can track building quality, infestation, neighborhood conditions, income, season, pets, children in the home, occupational take-home exposure, and local climate. Some of those variables are hard to measure well in NHANES.
The strongest next design would use repeated urine samples and repeated PHQ-9 or clinical depression measures over time. That would test whether rising 3-PBA comes before symptom worsening, whether associations persist across seasons, and whether exposure reduction changes depressive symptoms.
What Would Make the Pesticide Signal More Convincing?
A stronger causal case would need repeated exposure measurement. One urine sample can miss episodic spray use, seasonal pest-control changes, occupational take-home exposure, and product switching. Depression symptoms also fluctuate, so a single PHQ-9 window can misclassify people whose symptoms rise or fall later.
Temporal order: the most important test is whether higher 3-PBA precedes later depressive symptoms. A longitudinal design could compare people before and after pest-control episodes, or follow households across high-exposure and low-exposure seasons.
Exposure specificity: residential pesticide exposure is a mixture, not a single chemical. The 2026 paper measured DEET, DCBA, DHMB, 3-PBA, 4F-3-PBA, and cis-DCBA, but product labels, application method, ventilation, indoor dust, and pest burden would add context that urine alone cannot provide.
Mechanism: the most plausible psychiatric bridges are neuroinflammation, oxidative stress, monoamine signaling, sleep disruption, and dopaminergic toxicity. Mechanistic follow-up should measure those pathways directly instead of relying on depression symptom scores alone.
Even with those limits, the study usefully separates 2 claims. A broad self-report question about household pesticide use was not decisive after adjustment. Biomarker-based pyrethroid exposure, especially 3-PBA and female 4F-3-PBA, carried the more interesting signal.
Risk Reduction Should Be Practical, Not Alarmist
The safest public-health response is ordinary exposure minimization. That means using nonchemical pest control first when realistic, sealing entry points, reducing standing water and food sources, following label instructions, ventilating treated spaces, storing products safely, and avoiding unnecessary indoor spraying.
Why not panic: the adjusted overall 3-PBA estimate was small, and the confidence interval sat close to the null. A person with depressive symptoms should not interpret a possible pyrethroid exposure as the main explanation without considering sleep, stress, medical illness, medications, alcohol, substance use, financial strain, and prior psychiatric history.
Why not ignore it: low-dose household exposures are widespread, and small risks can matter at population scale. If repeated studies find similar biomarker associations, household pest control could become part of environmental mental-health prevention, especially in poorly ventilated or high-infestation housing.
The best current interpretation is exposure hygiene plus better research. Reducing unnecessary indoor pesticide exposure is reasonable even without a proven depression-causation claim, because pyrethroids are neuroactive chemicals and safer pest-control methods often exist.
Clinically, the result should not distract from established depression care. A person with PHQ-9 symptoms still needs ordinary assessment: symptom duration, sleep, anxiety, suicidality, substance use, medical contributors, medications, psychosocial stress, and treatment access. Environmental exposure history can be one more question, especially when indoor pest-control use is frequent.
Public-health researchers should also avoid treating “household pesticide exposure” as a single exposure. A bait station, a professional treatment, a fogger, a topical pet product, and frequent indoor spray use can create different exposure patterns. Better product-level detail would make future associations easier to interpret.
Equally, depression measurement needs depth. PHQ-9 is useful for screening, but future studies should separate new-onset depression, recurrent depression, anxiety overlap, sleep symptoms, and medication-treated illness. Those distinctions could reveal whether pesticide biomarkers track broad distress or a narrower depressive phenotype.
Until then, the association is a signal to study, not a verdict.
Questions About 3-PBA and Depression
Does this prove household pesticides cause depression?
No. The study found cross-sectional associations. It cannot prove that pesticide exposure caused depressive symptoms.
Why did urinary biomarkers look stronger than self-report?
Self-report depends on memory and awareness of products used at home. Urinary metabolites can capture recent absorbed exposure more directly, though they still vary over time.
Should the result change household pest control behavior?
It supports caution with unnecessary indoor insecticide exposure, ventilation, label-following, and nonchemical pest control when practical. A urine metabolite alone cannot diagnose a person’s depression.
References
- Chen M, Dai H, Tong Z, Lin M. Joint association of household pesticide exposure with depression in adults: a cross-sectional analysis from National Health and Nutrition Examination Survey 2007-2014. Depression and Anxiety. 2026;2026:4872833. https://doi.org/10.1155/da/4872833
- Chen Y, et al. Association between pyrethroid exposure and depressive symptoms in adults: the role of physical activity. Environmental Research. 2020. https://doi.org/10.1016/j.envres.2020.109760
- Wan J, et al. 3-Phenoxybenzoic acid exposure and dopaminergic neurotoxicity. Science of the Total Environment. 2022. https://doi.org/10.1016/j.scitotenv.2022.156027
- Kim J, et al. Household insecticide use and urinary 3-phenoxybenzoic acid concentrations. Journal of Exposure Science and Environmental Epidemiology. 2021. https://doi.org/10.1038/s41370-020-00276-3