
A randomized crossover trial found that 150 mg caffeine did not increase subjective anxiety, interoceptive attention, or anxiety from body sensations in 29 people with panic disorder compared with 53 healthy controls.1 The result runs opposite the hypothesis, but it does not make caffeine inert: caffeine still increased physiological arousal, costly avoidance, and attention problems during tasks.
Research Highlights
- The 150 mg dose did not trigger the expected anxiety rise: subjective anxiety, interoceptive attention, and anxiety from body sensations did not increase in the 29 panic disorder patients or the 53 controls.1
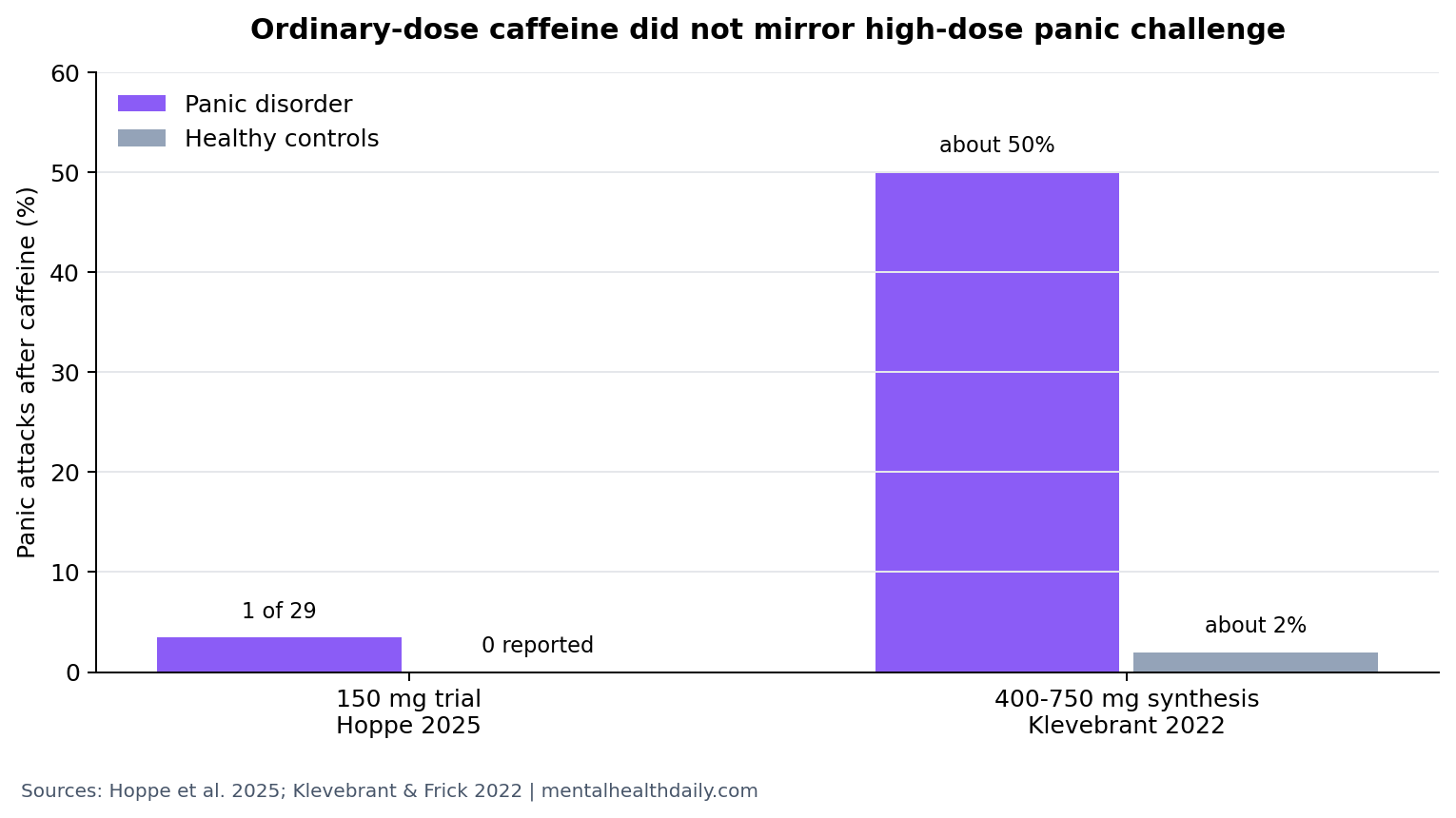
- Panic attacks were rare: only 1 panic attack occurred, and it happened in a panic disorder participant after caffeine during the emotional-reactivity task.1
- High-dose evidence still looks different: prior caffeine-challenge synthesis reported panic attacks in about 50% of panic disorder participants and 2% of controls after roughly 400-750 mg caffeine.2
- Arousal still moved: caffeine increased skin conductance responses to faces and increased costly avoidance in both groups, so the null subjective-anxiety finding was not a no-effect result.1
- Clinical advice should be dose-specific: one 150 mg challenge cannot justify blanket caffeine abstinence, but it also cannot clear high doses, repeated dosing, or individualized triggers.1
Panic disorder is a condition marked by recurrent panic attacks plus anticipatory fear of future attacks or avoidance of situations that might trigger them. Interoception means attention to internal body signals such as heartbeat, breathing, dizziness, or chest tightness; in panic disorder, those signals can be misread as danger.
The caffeine question is not “safe or unsafe” in the abstract. The more useful question is dose and context: whether an ordinary caffeine dose behaves like the high-dose laboratory challenges that historically provoked panic in vulnerable patients.
150 mg Caffeine Did Not Increase Subjective Panic Anxiety
Hoppe et al. enrolled 29 patients with panic disorder and 53 healthy controls who normally consumed no more than 300 mg caffeine per week. Participants abstained from caffeine for 36 h, then received 150 mg caffeine or placebo in a double-blind crossover design, with sessions 2-14 days apart.1
Primary outcome: subjective anxiety did not increase more after caffeine than after placebo. The same pattern held for interoceptive attention and anxiety from interoceptive signals. Panic disorder patients had higher baseline anxiety than controls, and anxiety rose during demanding tasks, but caffeine did not create the predicted extra panic-disorder-specific anxiety effect.
The trial explicitly contradicted its own expectation. The researchers expected 150 mg caffeine to increase subjective anxiety and body-signal anxiety in panic disorder, more than in controls. Instead, the ordinary dose failed to reproduce the high-dose panic-challenge pattern.
1 Panic Attack Is Not the Same as No Caffeine Effect
Only 1 panic attack occurred across the whole trial, and it occurred in a panic disorder participant after caffeine during the emotional-reactivity task.1 That single event is too rare to claim that 150 mg caffeine is panicogenic in the group as a whole.
Physiology told a narrower story. Skin conductance response is an electrical-sweat-gland measure used as a rough index of sympathetic arousal. Caffeine increased skin conductance responses to neutral, fearful, and happy faces, meaning the drug made the body more reactive even when subjective anxiety did not climb.
Costly avoidance means avoiding an option even when avoidance sacrifices reward. Caffeine increased costly avoidance in both panic disorder patients and controls, and avoidance was not more caffeine-sensitive in the panic disorder group. This is the calibrated read: 150 mg caffeine did not act like a panic trigger, but it did nudge arousal and avoidance systems.
High-Dose Caffeine Evidence Remains More Concerning
The most important comparator is the earlier caffeine-challenge literature. Klevebrant and Frick synthesized placebo-controlled studies and reported that caffeine doses roughly equivalent to 4-5 cups of coffee, about 400-750 mg, induced panic attacks in about 50% of panic disorder participants and 2% of healthy controls.2
Charney et al. also helped establish that caffeine can have stronger anxiogenic effects in panic disorder than in controls under high-dose challenge conditions.3 Those studies are why caffeine abstinence became a common recommendation in panic disorder advice.
The new trial does not erase that history. It separates an ordinary dose from a pharmacologic challenge. A single 150 mg dose is closer to a typical coffee than to the older panic-provocation experiments, and the evidence should not be collapsed across those exposure levels.
Dose translation: a 150 mg exposure is compatible with ordinary coffee intake, while 400-750 mg is closer to several strong coffees or some high-caffeine products consumed in a short window. Panic-disorder advice that treats those exposures as interchangeable loses the key clinical variable.
That dose split also helps explain why the paper’s conclusion is more useful than a simple “coffee is fine” headline. A panic disorder patient who drinks 1 moderate coffee in the morning and never notices symptoms is in a different evidence category from a patient who uses multiple coffees, energy drinks, or caffeine tablets and then enters a crowded, emotionally demanding situation.
Emotional Tasks May Reveal Effects Resting Ratings Miss
Totten and France previously gave 200 mg caffeine and placebo to people with panic disorder and controls before emotional, physical, and cognitive stressors. They reported caffeine-related increases in skin conductance during stressors without clear evidence that panic disorder patients were uniquely vulnerable.4
Hoppe et al. fit that lower-dose pattern. The subjective panic-anxiety endpoint was null, while physiological arousal and task behavior still shifted. That split matters for real-world advice because a person may not feel dramatically more anxious yet still become more reactive or more avoidant under emotionally loaded conditions.
Practical calibration: panic disorder patients who notice reliable caffeine-triggered symptoms should treat their own pattern seriously. For group-level evidence, the current trial supports individual assessment and dose reduction before categorical abstinence, especially at ordinary doses.
Task context: caffeine’s arousal effects showed up when participants processed emotional faces, made approach-avoidance choices, and performed attention tasks. That is closer to real life than resting anxiety alone. Panic disorder often becomes disabling because ordinary arousal is interpreted as danger during activity, travel, social settings, or conflict. A caffeine effect that increases arousal without increasing resting anxiety can still matter if it pushes behavior toward avoidance.
The crossover design strengthens this point because each participant experienced caffeine and placebo. Stable traits such as general anxiety level, panic history, and personality could not fully explain the substance effect. The strongest reading is therefore split-level: 150 mg caffeine did not add subjective panic anxiety in the expected way, but it did alter physiological and behavioral channels that can feed panic-relevant avoidance.
Evidence Strength and Limits
This was a randomized, placebo-controlled crossover trial, so each participant served as their own comparator. That design is stronger than a simple observational caffeine survey because expectancy, baseline anxiety, and stable individual traits are partly controlled by within-person comparison.
The limits are still real. Participants were young, consumed little caffeine habitually, and received one acute 150 mg dose after abstinence. The trial cannot answer chronic caffeine use, withdrawal effects, energy-drink doses, older patients, comorbid substance use, pregnancy, or people who already know caffeine reliably provokes their panic symptoms.
How to use the evidence: clinicians and patients can treat caffeine as a graded exposure variable. A practical experiment might compare no caffeine, a small dose with food, and a normal dose on low-stress days while tracking panic symptoms, avoidance, sleep, and rebound anxiety. That is more evidence-aligned than assuming caffeine is universally prohibited or universally harmless.
Sleep timing should be tracked too, because late caffeine can worsen next-day anxiety through insomnia rather than through an immediate panic mechanism.
Dose remains the boundary. The reassuring part of this trial applies to 150 mg caffeine, roughly a moderate coffee dose, under controlled conditions. It should not be stretched to 400-750 mg challenge studies, concentrated energy drinks, caffeine pills, or repeated use during sleep loss. The older high-dose literature still supports caution for panic-prone patients.
That dose boundary also keeps the advice practical: test the actual amount used, at the actual time of day, before turning caffeine into a global yes-or-no rule.
Symptom diaries are more useful than memory after a bad panic week.
They also expose delayed sleep-mediated anxiety patterns.
Questions About Caffeine and Panic Disorder
Does this mean coffee is safe for everyone with panic disorder?
No. The trial says 150 mg caffeine did not increase group-level subjective anxiety in this specific crossover design. It does not overrule individual sensitivity, high-dose evidence, or repeated daily intake.
How much caffeine is 150 mg?
It is roughly the caffeine content of a strong cup of coffee, depending on brew size and preparation. The older panic-challenge literature used much higher exposures, roughly 400-750 mg.
How should a panic disorder patient read the 150 mg result?
Start with dose. Ordinary caffeine did not behave like a panic challenge in this trial, but high doses remain more concerning. If caffeine reliably worsens symptoms, reduce or stop it; if it does not, the evidence does not require blanket avoidance.
References
- Hoppe JM, Bjorkstrand J, Vegelius J, et al. Acute effects of 150 mg caffeine on subjective, physiological, and behavioral components of anxiety in panic disorder and healthy controls. Journal of Psychopharmacology. 2025. doi:10.1177/02698811251344692
- Klevebrant L, Frick A. Effects of caffeine on anxiety and panic attacks in patients with panic disorder and healthy controls: a systematic review and meta-analysis. General Hospital Psychiatry. 2022. doi:10.1016/j.genhosppsych.2021.11.005
- Charney DS, Heninger GR, Jatlow PI. Increased anxiogenic effects of caffeine in panic disorders. Archives of General Psychiatry. 1985. doi:10.1001/archpsyc.1985.01790260027003
- Totten V, France CR. Physiological and subjective anxiety responses to caffeine and stress in panic disorder. Behaviour Research and Therapy. 1995. doi:10.1016/0887-6185(95)00025-j