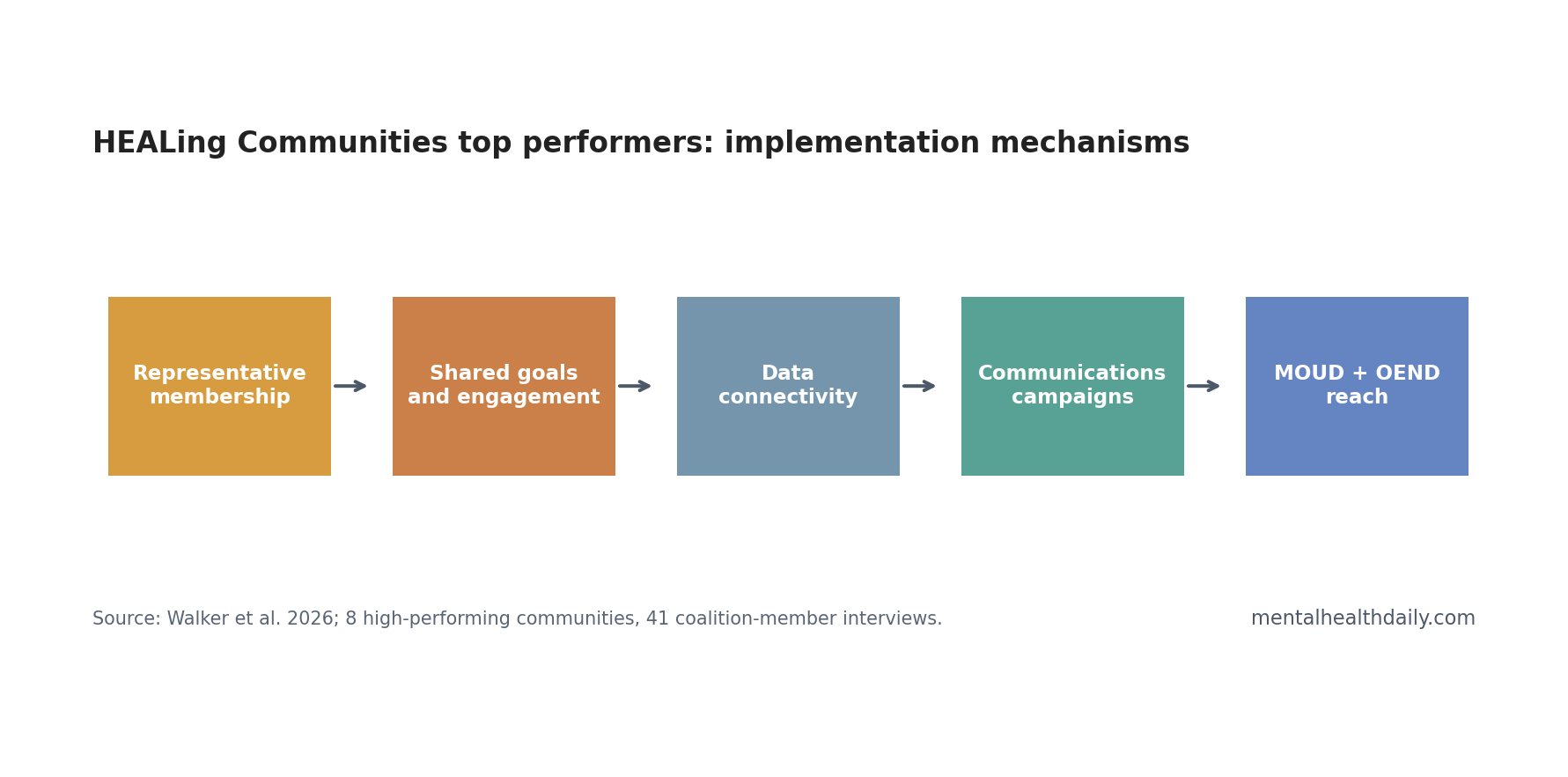
A 2026 qualitative case study of 8 top-performing HEALing Communities Study communities linked opioid-response implementation success to representative coalition membership, shared goals, data connectivity, and communications campaigns, not to a simple urban-vs.-rural split.1 The useful lesson is operational: coalitions worked when collaboration was turned into service reach for medication for opioid use disorder and overdose education and naloxone distribution.
Research Highlights
- 8 high-performing communities: Researchers selected the top urban and rural waitlist-control community within each of 4 HEALing Communities Study sites.1
- 41 coalition interviews: The qualitative analysis drew on 41 coalition-member interviews conducted after the implementation phase.1
- Membership had to match the work: Representative coalition membership, high engagement, and aligned goals supported implementation across settings.1
- Data made strategy selection concrete: Structured data connectivity and sharing helped coalitions choose and adjust MOUD and OEND strategies.1
- Urban/rural status did not explain themes: No major qualitative theme differed by urban vs. rural classification in these high-performing communities.1
Medication for opioid use disorder (MOUD) refers to evidence-based medications such as buprenorphine, methadone, or extended-release naltrexone that reduce opioid-use-disorder morbidity and mortality. Overdose education and naloxone distribution (OEND) means training people to recognize overdose and distributing naloxone, the opioid-overdose reversal medication.
Those interventions already have strong evidence. The harder public-health question is implementation: how communities make MOUD and naloxone available, acceptable, and reachable across health systems, jails, emergency services, harm-reduction programs, and local organizations.
Top Performers Were Selected by MOUD and OEND Implementation Metrics
Walker et al. used a positive deviance design. Positive deviance means studying unusually successful cases to identify what they did differently, rather than averaging across all cases. The researchers selected 8 high-performing waitlist-control communities from the HEALing Communities Study: the top-performing urban and rural community within each of 4 study sites.1
Performance was based on average ranking across 4 implementation metrics: percentage of selected OEND strategies implemented, percentage of selected MOUD strategies implemented, population-adjusted reach of OEND, and population-adjusted reach of MOUD.1
The analysis then used 41 coalition-member interviews. Seventeen interviewees represented rural communities and 24 represented urban communities. Most interviewees were female, non-Hispanic, White, and college-educated, which matters for interpreting representativeness.1
Representative Membership Was a Working Mechanism
The first internal coalition theme was representative membership plus high engagement aligned with coalition goals. This was not a vague diversity claim. Interviewees described coalitions that included physicians, shelters, churches, hospitals, housing, law enforcement, emergency medical services, health departments, and people connected to local substance-use-disorder work.1
That breadth matters because MOUD and naloxone do not move through one channel. Naloxone may need pharmacies, jails, emergency responders, syringe-service programs, shelters, and family networks. MOUD may need prescribers, referral systems, transportation, stigma reduction, and follow-up.
Implementation mechanism: representative membership gave the coalition access to more settings, more relationships, and more practical knowledge about where service delivery was stuck.
Shared Goals Reduced Fragmentation Across Agencies
The second internal theme was collaboration and shared vision. Coalition members described limited friction and a sense that individual evidence-based practices were part of a larger structural response, not isolated projects.1
That distinction is important in opioid-response work. A county can have naloxone boxes, MOUD prescribers, jail programs, peer outreach, and media campaigns while still failing if those efforts do not connect. Shared goals make the system legible: who does what, which population is being reached, where referrals go, and which gap remains.
The practical value is coordination. If emergency medical services distribute naloxone but treatment referral is weak, overdose reversal becomes disconnected from continuing care. If MOUD capacity exists but stigma blocks uptake, capacity does not translate into use.
Data Connectivity Turned Coalition Energy Into Strategy
The Communities That HEAL process used facilitation, data-driven decision making, and a communications campaign to support community implementation. Walker et al. found that top-performing communities used structured data connectivity and data sharing to guide strategy selection.1
Data connectivity means more than having a dashboard. It means coalitions can see where overdoses, service gaps, naloxone distribution, referral bottlenecks, and MOUD reach are occurring, then adjust strategies in response.
That mechanism helps explain why generic coalition enthusiasm is not enough. Without data, the coalition may choose visible but low-yield activities. With usable data, it can aim resources toward the settings and populations where MOUD or OEND reach is actually missing.
Communications Campaigns Worked as Implementation Support
Multi-channel communications campaigns were another intervention-linked theme. The campaigns increased awareness, acceptance, and uptake of opioid-use-disorder and MOUD services.1
Communications campaigns are sometimes treated as soft add-ons, but in opioid work they can change the operating environment. People need to know where naloxone is available, which organizations provide treatment, whether MOUD is legitimate care, and whether local services are safe to approach.
- Awareness: residents and service providers know what exists.
- Acceptance: stigma around MOUD and naloxone is reduced enough for uptake.
- Navigation: people can move from overdose risk or crisis contact into continuing care.
- Sustainability: community partners see the work as part of local infrastructure rather than a temporary study activity.
Parent HEALing Communities Results Keep the Case Study Grounded
The qualitative paper sits inside a larger intervention program. The HEALing Communities Study tested a community-based intervention to reduce opioid overdose deaths across Kentucky, Massachusetts, New York, and Ohio.2 Related analyses examined mortality including polysubstance overdose deaths and community stigma outcomes.34
The 2026 case study answers a different question from those trial analyses: among communities that performed well on implementation metrics, what local mechanisms helped?
That pairing is valuable. Quantitative trial outcomes tell whether an intervention moved endpoints. Qualitative positive-deviance work helps explain how implementation actually happened on the ground.
Urban vs. Rural Was Not the Main Divide
The study included both urban and rural high-performing communities, but the researchers reported no major theme differences by that dichotomy.1 Geography still shapes implementation, but the common mechanisms in top performers cut across the urban-rural label.
The paper also cautioned that the classification could miss cultural and practical differences. Some communities labeled urban had relatively small populations or functioned more like rural environments. For implementation planning, service topology may matter more than a binary urban/rural code.
Operational read: ask whether the coalition has the right members, shared goals, data access, service partners, and communication channels. Do not assume that geography alone predicts implementation capacity.
Evidence Strength: Useful Mechanisms, Not Causal Proof
Evidence-strength note: this was a qualitative analysis of top performers. It can identify plausible implementation mechanisms and transferable design principles. It cannot prove that any single coalition feature caused higher MOUD or OEND reach, and it cannot show whether lower-performing communities lacked the same themes.
The interview sample also limits interpretation. Interviewees were mostly non-Hispanic White, highly educated, and coalition-connected. The analysis may underrepresent people with opioid use disorder, families, unaffiliated community members, or people who avoided services because of stigma or prior harm.
Those limits do not weaken the practical message. They keep it honest: the paper is a playbook generator, not a causal trial.
Equity of access still has to be measured directly. A coalition can look organized while people at highest overdose risk still face transportation gaps, clinic-hour barriers, fear of police contact, or medication stigma. Future implementation audits should compare coalition membership against who actually starts MOUD, receives naloxone, and remains reachable after an overdose event.
Outcome discipline matters. Naloxone distribution, MOUD referrals, treatment starts, retention, and overdose deaths are related but not interchangeable. A coalition may improve one step while failing another. The useful version of this model tracks the whole pathway, so outreach wins do not hide initiation gaps and treatment starts do not hide poor follow-up.
That pathway view is the main reason the qualitative themes are useful. They point to where implementation can break across referral, initiation, medication access, follow-up, and overdose-prevention handoff.
Each handoff needs an owner, a metric, and a repair plan.
What Opioid Coalitions Should Copy Carefully
The safest takeaway is a checklist of implementation conditions:
- Map the service pathway: identify where people encounter overdose risk, naloxone, referral, MOUD initiation, and follow-up.
- Recruit by function: coalition seats should match service gaps more than institutional prestige.
- Use current data: overdose, naloxone, referral, and MOUD-reach data should shape strategy choice.
- Build shared goals: partners need a common definition of what counts as progress.
- Communicate repeatedly: campaigns should reduce stigma and tell people where help actually is.
The calibrated claim is not that coalitions automatically work. Coalitions work when they become a delivery system for evidence-based practices.
Questions About Opioid Coalition Implementation
What did this case study measure?
It analyzed interviews from 41 coalition members in 8 high-performing HEALing Communities Study communities selected by MOUD and OEND implementation metrics.
Did the study prove coalitions reduced overdose deaths?
No. The parent HEALing Communities trial and related analyses address outcome effects. This qualitative paper explains mechanisms in top-performing implementation cases.
Which coalition feature was most actionable in the HEALing Communities case study?
Coalitions need representative membership, shared goals, data connectivity, and communications campaigns that directly support MOUD and naloxone reach.
References
- Walker DM, et al. The role of external and internal context on adoption and implementation of evidence-based practices: a serial case study qualitative analysis of top performers in the HEALing Communities Study. Implementation Science Communications. 2026. https://doi.org/10.1186/s43058-026-00952-9
- HEALing Communities Study Consortium. Community-Based Cluster-Randomized Trial to Reduce Opioid Overdose Deaths. New England Journal of Medicine. 2024. doi:10.1056/nejmoa2401177
- Freisthler B, et al. Communities That HEAL Intervention and Mortality Including Polysubstance Overdose Deaths. JAMA Network Open. 2024. https://doi.org/10.1001/jamanetworkopen.2024.40006
- Davis A, et al. Effects of the Communities that Heal intervention on perceived opioid-related community stigma in the HEALing Communities Study. The Lancet Regional Health – Americas. 2024. https://doi.org/10.1016/j.lana.2024.100710