A 2026 behavioral-variant frontotemporal dementia MRI study found that simple visual ratings of orbitofrontal and frontoinsular brain atrophy helped separate probable from possible bvFTD, with baseline left orbitofrontal atrophy predicting 3.77-fold higher odds of probable bvFTD classification.1
Research Highlights
- 143 people were rated: the study included 93 probable bvFTD cases, 15 possible bvFTD cases, and 35 healthy controls.1
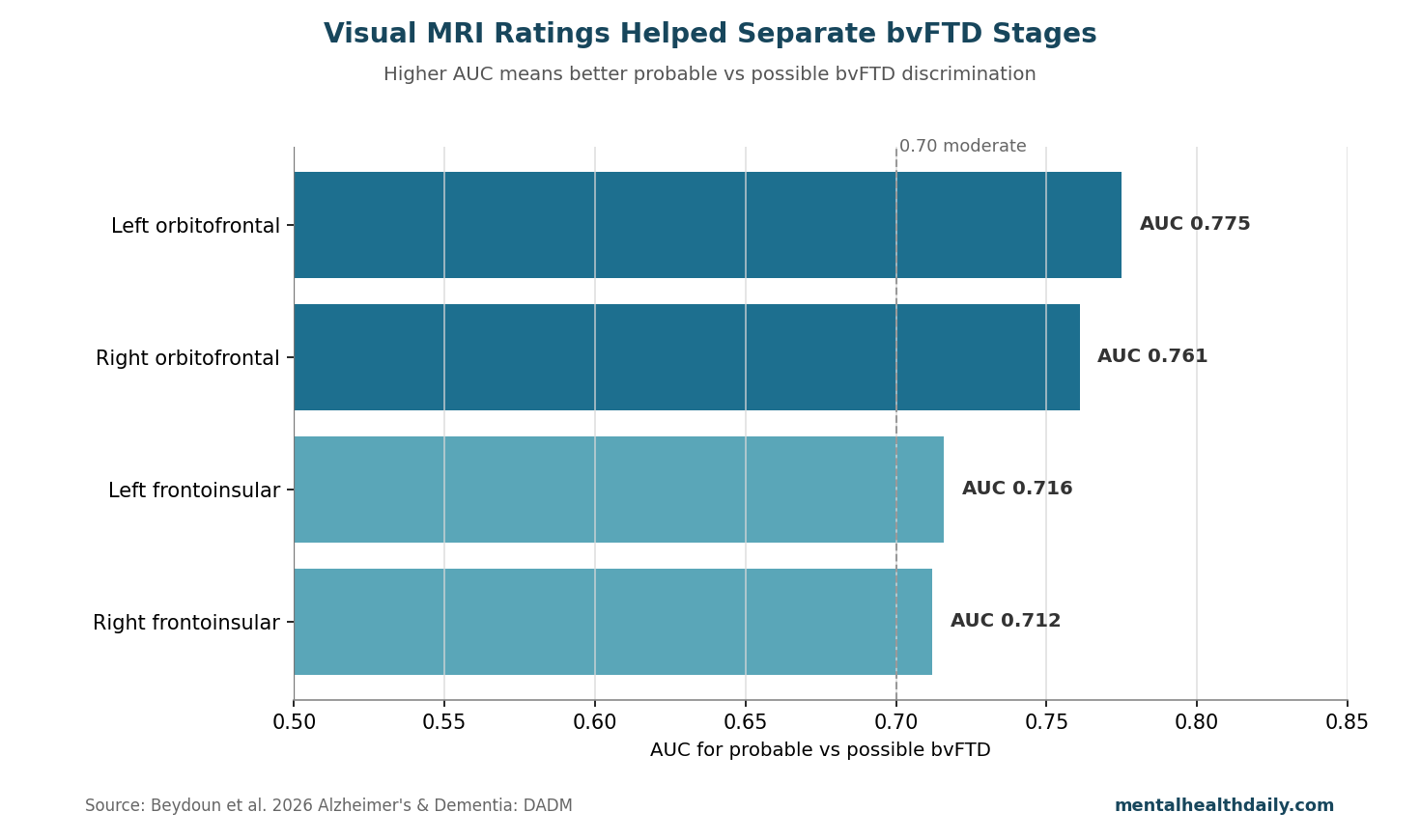
- Orbitofrontal atrophy carried the strongest diagnostic signal: left orbitofrontal visual rating had AUC = 0.775 for probable vs possible bvFTD, and right orbitofrontal rating had AUC = 0.761.1
- Frontoinsular atrophy also helped: left and right frontoinsular ratings had AUC values of 0.716 and 0.712 for probable vs possible bvFTD.1
- Left orbitofrontal score predicted probable classification: each higher baseline left orbitofrontal rating was associated with odds ratio 3.77, 95% CI 1.61–8.84, p = .002.1
- Visual MRI supports clinical diagnosis: the 5 rating scales can add confidence, but they do not replace history, behavior, neuropsychology, longitudinal change, or differential diagnosis.
Behavioral-variant frontotemporal dementia, or bvFTD, is a neurodegenerative syndrome marked by progressive changes in personality, inhibition, empathy, compulsive behavior, eating patterns, and executive function. It often affects frontal and anterior temporal brain networks before memory becomes the dominant complaint.
Visual Ratings Targeted Orbitofrontal and Frontoinsular Atrophy
Beydoun et al. evaluated 5 MRI visual rating scales in people with probable bvFTD, possible bvFTD, and healthy control participants. Blinded raters scored regional atrophy, meaning visible tissue loss, on routine structural MRI.1
- Orbitofrontal cortex: a frontal region involved in reward, social behavior, impulse control, and flexible updating when consequences change.
- Frontoinsular cortex: a region involved in salience detection, interoception, emotion, and switching between internal and external demands.
- Visual rating scale: a structured clinician-readable score based on visible MRI atrophy rather than automated volumetric software.
- AUC: area under the receiver operating characteristic curve; 0.50 is chance-level discrimination, and 1.00 is perfect separation.
Probable bvFTD requires stronger clinical and functional evidence than possible bvFTD. MRI atrophy is especially useful when behavior suggests bvFTD but psychiatric illness, Alzheimer's disease, vascular disease, substance effects, medication effects, or atypical mood disorders remain plausible alternatives.
Orbitofrontal Ratings Separated Probable From Possible bvFTD
Left orbitofrontal atrophy had the highest discrimination for probable vs possible bvFTD, with AUC = 0.775. Right orbitofrontal atrophy followed closely, with AUC = 0.761. Frontoinsular ratings were also above the usual 0.70 threshold for moderate discrimination: left frontoinsular AUC = 0.716, and right frontoinsular AUC = 0.712.1
Group separation: right orbitofrontal atrophy differed strongly across probable bvFTD, possible bvFTD, and controls, with F(2,140) = 34.822, p < .001, and η2 = .332. Left orbitofrontal atrophy was similar, with F(2,140) = 35.041, p < .001, and η2 = .334.1
Left Orbitofrontal Atrophy Predicted 3.77x Odds
Prediction result: in logistic modeling, baseline left orbitofrontal visual rating predicted probable bvFTD classification with odds ratio = 3.77, 95% CI 1.61–8.84, and p = .002.1 This means a higher left orbitofrontal atrophy score was associated with markedly higher odds of falling into the probable bvFTD group rather than the possible bvFTD group.
Conversion subset: among possible bvFTD cases with follow-up classification, 5 of 10 converted to probable bvFTD. Converters had higher baseline left orbitofrontal visual ratings than non-converters, with Mann-Whitney U = 5 and p = .053. The p value was just above the usual .05 threshold, and the subset was very small.
Left orbitofrontal atrophy is clinically believable because bvFTD often disrupts reward-guided behavior, disinhibition, social judgment, compulsive behavior, and emotional regulation. Those symptoms map more naturally onto fronto-orbitofrontal and salience-network degeneration than onto a memory-first hippocampal pattern.
Adjacent bvFTD Research Supports MRI as a Confidence Tool
Rascovsky et al. established revised diagnostic criteria that distinguish possible bvFTD from probable bvFTD partly by requiring functional decline and imaging evidence compatible with frontal or anterior temporal involvement.2 That framework makes MRI a confidence layer, not the whole diagnosis.
Imaging utility: later work has shown that structural atrophy patterns can improve diagnostic classification in frontotemporal dementia, especially when combined with clinical phenotype and longitudinal progression.3 Visual rating scales are less precise than automated volumetry, but they are faster, cheaper, and easier to use in ordinary radiology and neurology workflows.
- Best use: support bvFTD diagnosis when behavior is progressive and regional atrophy fits the syndrome.
- Weak use: rule bvFTD in or out from one MRI score without clinical trajectory.
- Common pitfall: overcalling psychiatric bvFTD mimics when frontal atrophy is mild, nonspecific, or age-related.
Evidence-Strength Note for This Cohort Study
What the cohort supports: this study can support diagnostic association and prediction within a specialized cohort. It shows that visual MRI ratings, especially left orbitofrontal ratings, tracked probable bvFTD status and may help identify possible bvFTD cases more likely to convert.
Design limits: possible bvFTD cases were few, only 10 had conversion information in the highlighted follow-up subset, and diagnostic categories can shift as clinical information accumulates. Visual ratings also depend on scanner quality, rater training, age norms, vascular burden, and the presence of psychiatric or neurodegenerative mimics.
Routine MRI can miss early bvFTD, especially when atrophy is subtle or symptoms are dominated by behavior before visible structural change. A normal or mildly abnormal scan does not settle a difficult case when progressive behavioral change continues.
MRI Ratings Add Confidence When bvFTD Symptoms Are Ambiguous
Visual MRI ratings are most useful for triage and diagnostic confidence. When a person has progressive disinhibition, apathy, loss of empathy, compulsions, hyperorality, or executive dysfunction, visible orbitofrontal and frontoinsular atrophy should raise confidence that the pattern is neurodegenerative rather than purely psychiatric.
Clinical implication: higher left orbitofrontal visual rating should prompt careful longitudinal follow-up, caregiver collateral, functional assessment, medication review, neuropsychological testing, and consideration of frontotemporal dementia specialty evaluation. It should not be used as a single-score diagnosis.
Psychiatric Mimics Are the Hardest Use Case
bvFTD can resemble late-life bipolar disorder, major depression with apathy, obsessive-compulsive disorder, personality change after trauma, medication effects, substance-related frontal impairment, sleep disorders, and autism-spectrum traits that became more visible under stress. MRI atrophy ratings help most when they are interpreted against a clear timeline of progressive decline.
Collateral history: caregiver reports often carry more diagnostic weight than a brief office impression. New loss of empathy, social rule-breaking, compulsive routines, dietary change, financial recklessness, or loss of insight over years is different from a lifelong interpersonal style or an episodic mood disorder.
- Stronger bvFTD pattern: progressive behavioral change plus orbitofrontal or frontoinsular atrophy.
- Weaker bvFTD pattern: nonspecific symptoms, stable function, and mild age-compatible atrophy.
- Follow-up value: repeat clinical assessment can separate progressive degeneration from static traits or treatable psychiatric illness.
Why left orbitofrontal signal is clinically plausible: left frontal and orbitofrontal degeneration can disrupt language-mediated social judgment, impulse control, and flexible decision-making. A higher visual atrophy rating in that region should raise suspicion when the behavioral history already points toward progressive social and executive change.
Visual ratings also make MRI interpretation more transparent. Instead of saying that an MRI is “consistent with atrophy” in vague terms, the clinician can name the region, explain what that region helps regulate, and connect the imaging pattern to observed behavior. That improves caregiver understanding without turning the score into a diagnosis.
Workflow fit: a reasonable pathway is baseline MRI rating, structured neuropsychological testing, collateral interview, reversible-cause review, and repeat assessment when the diagnosis remains possible rather than probable. The rating helps decide how aggressively to follow the case.
For families, that distinction can change planning. A probable neurodegenerative syndrome prompts driving review, financial safeguards, work decisions, caregiver support, home-safety changes, advance-care conversations, supervision planning, medication-safety review, earlier legal planning, and genetic counseling when family history suggests inherited frontotemporal dementia risk.
The same caution protects patients from overdiagnosis. A visual atrophy score should not turn social awkwardness, depression, irritability, or lifelong impulsivity into dementia by itself. The score becomes meaningful when it lines up with new progressive behavior change, loss of everyday function, informant concern, and regional MRI change that fits the syndrome.
Questions About MRI Ratings in bvFTD
Can MRI diagnose bvFTD by itself?
No. MRI supports diagnosis when symptoms and progression fit bvFTD, but diagnosis still depends on clinical history, behavior, function, and differential diagnosis.
Which MRI region looked strongest?
Left orbitofrontal atrophy had the strongest discrimination and predicted probable bvFTD classification with odds ratio 3.77.
Why use visual ratings instead of automated brain volume?
Visual ratings are easier to deploy in ordinary clinical practice. Automated volumetry may be more precise, but it is not always available or standardized.
What should a possible bvFTD label trigger?
Possible bvFTD should trigger follow-up rather than diagnostic closure. Repeat history, informant reports, neuropsychological testing, medication review, and interval MRI can show whether the pattern is progressive degeneration or a psychiatric, vascular, sleep, substance, or medication mimic.
The practical value is disciplined surveillance: track change over time, then update confidence as behavior, function, and imaging either converge or separate.
References
- Quantitative assessment of brain atrophy in bvFTD: Implications for diagnostic conversion. Beydoun S, Polverino F, Miller BL, et al. Alzheimer's & Dementia: Diagnosis, Assessment & Disease Monitoring. 2026;18:e70307. doi:10.1002/dad2.70307
- Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia. Rascovsky K, Hodges JR, Knopman D, et al. Brain. 2011;134:2456–2477. doi:10.1093/brain/awr179
- Diagnostic utility of measuring cerebral atrophy in the behavioral variant of frontotemporal dementia. Illan-Gala I, Montal V, Borrego-Ecija S, et al. JAMA Network Open. 2021;4:e211290. doi:10.1001/jamanetworkopen.2021.1290
- The diagnosis of young-onset dementia. Rossor MN, Fox NC, Mummery CJ, Schott JM, Warren JD. Lancet Neurology. 2010;9:793–806. doi:10.1016/S1474-4422(10)70159-9