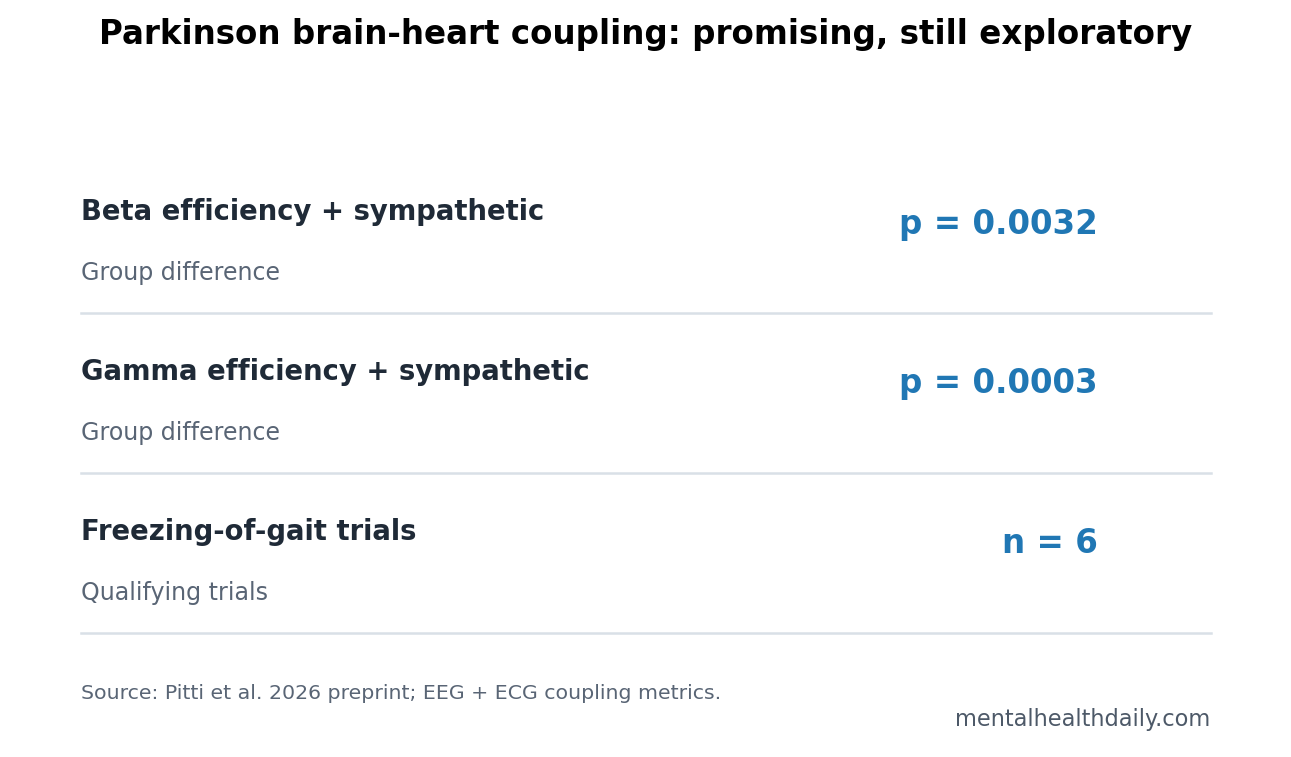
A 2026 EEG-ECG preprint reported that beta efficiency-sympathetic coupling differed across healthy young adults, healthy older adults, and Parkinson’s disease patients, p = 0.0032, while gamma efficiency-sympathetic coupling differed at p = 0.0003.1 The main claim is that motor, cognitive, and autonomic physiology may be coupled tightly enough to deserve biomarker-level study.
Research Highlights
- Brain-heart coupling separated groups: Beta efficiency-sympathetic coupling differed across the 3 comparison groups, p = 0.0032, and gamma efficiency-sympathetic coupling differed at p = 0.0003.1
- Small Parkinson sample: The aging comparison used 15 Parkinson’s disease patients, 16 healthy older adults, and 32 healthy young adults, so the signal is exploratory.1
- MMSE range was narrow: Parkinson’s patients scored 26 to 30 on the Mini-Mental State Examination, meaning the cognitive analysis mostly tested subtle variation inside the normal screening range.1
- Freezing analysis was tiny: The freezing-of-gait dataset included 12 Parkinson’s patients, but only 6 trials had enough freezing episodes for the cluster analysis.1
- Clinical status is early: A 2026 preprint can justify expanded EEG-ECG studies before individual prediction of freezing, cognition, or autonomic failure.
Brain-heart coupling means synchronized information between brain network activity and cardiac autonomic signals. In this analysis, researchers combined EEG network metrics with ECG-derived sympathetic-vagal dynamics, then asked whether the combined physiology changed with aging, Parkinson’s disease, cognitive screening scores, and freezing of gait.
Freezing of gait is a Parkinson’s symptom in which walking briefly stalls even though the person intends to move. It is dangerous because it increases falls, and it is biologically interesting because it can involve motor control, attention, anxiety, posture, and autonomic arousal at the same time.
Beta and Gamma Coupling Differed Across Aging and Parkinson’s Groups
Pitti et al. used 3 comparison groups for the main aging/Parkinson’s analysis: 32 healthy young participants, 16 healthy older participants, and 15 people with Parkinson’s disease.1 EEG supplied network organization in delta, theta, alpha, beta, and gamma frequency ranges. ECG supplied cardiac sympathetic and vagal dynamics.
EEG beta activity refers to roughly 12 to 30 Hz brain rhythms often discussed in movement control. Gamma activity refers to faster 30 to 45 Hz rhythms often linked to local cortical processing and network coordination. Those labels are not diagnostic by themselves, but they give a frequency-specific way to test whether brain organization and autonomic state move together.
The strongest group-level results were coupling metrics rather than brain-only or heart-only variables. Beta efficiency-sympathetic coupling differed across groups, p = 0.0032, chi-square = 11.0034. Gamma efficiency-sympathetic coupling differed at p = 0.0003, chi-square = 13.9019.1
MMSE Correlations Were Interesting but Ceiling-Limited
The Parkinson’s subgroup also completed the Mini-Mental State Examination (MMSE), a brief cognitive screening test scored from 0 to 30. Scores from 26 to 30 usually sit in the normal range, so this was not a dementia or mild cognitive impairment analysis.
What the cognitive result can mean: within a small Parkinson’s sample, stronger coupling between alpha-band network organization and cardiac dynamics appeared alongside better MMSE scores. The 2026 preprint reported positive correlations for alpha modularity/cardiac coupling, including R = 0.5311 and R = 0.6428 in the displayed metrics.1
What it cannot mean: MMSE-linked coupling does not prove that EEG-ECG measures predict cognitive decline. A 15-person Parkinson’s sample with scores packed near the top of the scale can generate promising correlations while still being vulnerable to ceiling effects and outliers.
Freezing-of-Gait Clusters Need Replication Before Prediction
The freezing-of-gait analysis used a separate dataset involving 12 Parkinson’s patients performing a walking task designed to induce freezing. Only 6 trials contained enough freezing episodes for the cluster-level analysis.1
That small number matters. Freezing is episodic, context-dependent, and affected by task design, medication state, anxiety, dual-task load, and walking environment. A cluster found around the moment of freezing can guide physiology hypotheses, but it is not yet a deployable warning signal.
Adjacent work makes the general direction plausible. Heart-rate variability has been studied as a marker of freezing predisposition, and autonomic dysfunction is a long-standing part of Parkinson’s disease rather than a side problem.2 Brain-connectivity studies also show that Parkinson’s disease alters distributed networks before simple motor descriptions capture the whole picture.3
The important methodological move is the pairing itself. EEG alone can show altered network organization, and ECG alone can show autonomic change, but freezing of gait often appears when movement, attention, arousal, and posture collide. A combined EEG-ECG feature asks whether those systems shift together around vulnerable moments instead of treating motor and body-state signals as unrelated measurements.
Autonomic Dysfunction Makes the Signal Biologically Plausible
Autonomic dysfunction means impaired control of automatic body functions such as blood pressure, heart rate, sweating, digestion, and bladder function. Parkinson’s disease can affect those systems through peripheral and central nervous-system pathways, which is why ECG-linked brain measures are not a random add-on.
- Motor link: beta-band network organization is relevant to Parkinson’s movement physiology.
- Body-state link: cardiac sympathetic-vagal measures reflect arousal and autonomic regulation.
- Cognitive link: MMSE correlations suggest the brain-heart signal may track more than movement, but the evidence is early.
- Freezing link: gait freezing can involve attention, arousal, posture, and motor planning at once.
Evidence-strength note: this was an exploratory preprint combining small datasets. It can show that integrated EEG-ECG metrics are worth testing in Parkinson’s disease. It cannot diagnose Parkinson’s disease, predict freezing in real time, or replace validated cognitive assessment.
Why Combined EEG-ECG Measures Beat Isolated Signals
Brain-only measures can miss body-state changes that shape gait and cognition. Heart-only measures can miss the neural context that makes a sympathetic surge clinically meaningful. The integrated approach is useful because Parkinson’s freezing often appears at the intersection of posture, attention, anxiety, and motor planning.
Global efficiency describes how efficiently information can move across a network. Modularity describes how strongly a network separates into communities. When those EEG-derived measures are paired with sympathetic-vagal dynamics, the output asks whether brain organization and autonomic tone are changing as a coupled system.
The coupling metric tries to quantify whether cortical network structure and cardiac autonomic outflow share information. That distinction helps explain why the paper emphasizes systemic physiology instead of treating Parkinson’s disease as only a basal-ganglia movement disorder.
That is especially relevant for freezing of gait. A person can freeze during doorway crossing, turning, dual-task walking, or stressful movement. Those situations are not pure motor events. They load attention, visual processing, threat response, posture, and cardiovascular regulation at the same time.
Methodologically, the next step is not to add more exotic variables. It is to test whether a small set of interpretable EEG-ECG features predicts clinically defined freezing episodes better than gait sensors, heart-rate variability alone, or EEG alone.
Clinical Use Would Require Prospective Freezing Prediction
A clinically useful freezing marker would need to work before the freeze and stay reliable during or after it. It would also need to hold up across home walking, medication states, turning, fatigue, anxiety, and assistive-device use.
Validation burden: a wearable or clinic-based signal would need at least 4 tests before it should influence care:
- Episode timing: the signal should appear before freezing often enough to guide prevention.
- Specificity: the same pattern should not fire constantly during ordinary stress, effort, or standing.
- Medication robustness: the signal should be tested during on and off medication states.
- Outcome relevance: acting on the signal should reduce falls, fear of walking, or freezing frequency.
Until those tests exist, the result is best treated as physiology mapping. It helps define what to measure in future Parkinson’s studies, but it should not make patients or clinicians trust a brain-heart number over observed gait, falls history, cognition, and autonomic symptoms.
Replication should include home walking and clinic walking, because freezing often changes across settings.
Medication state also needs explicit handling. Parkinson’s gait, autonomic tone, and beta-band motor physiology can change across on-medication and off-medication periods, so a marker that works in only 1 medication context may fail during the part of the day when freezing is most disabling.
Future studies should predefine medication timing, walking triggers, and whether the signal is meant to detect freezing as it happens or predict it early enough to prevent a fall.
A clinically useful version would also need transparent failure cases. False alarms could make patients anxious or discourage walking; missed warnings could create false confidence. Replication should therefore report sensitivity, specificity, lead time before freezing, and whether the signal adds anything beyond simpler measures such as step timing, turn speed, falls history, and patient-reported freezing frequency.
Questions About Parkinson Brain-Heart Coupling
Could EEG and ECG eventually help monitor freezing of gait?
Possibly, but not from this study alone. A real monitoring tool would need larger prospective datasets, medication-state control, wearable validation, and prediction of freezing before it happens.
Why use MMSE if the scores were mostly normal?
MMSE gave a quick cognitive anchor inside the available dataset. More sensitive Parkinson-specific cognitive batteries would be needed to test whether coupling tracks early executive or visuospatial decline.
Does this support a brain-first vs. body-first Parkinson split?
Only indirectly. The data fit a broader view in which Parkinson’s disease affects distributed brain and body physiology, but the analysis did not classify patients into brain-first or body-first disease subtypes.
References
- Pitti A, et al. Assessing aging, cognitive ability and freezing of gait in Parkinson’s disease through integrated brain-heart network dynamics. medRxiv. 2026. doi:10.64898/2026.04.22.26351482
- Heimler B, et al. Heart-rate variability as a new marker for freezing predisposition in Parkinson’s disease. Parkinsonism & Related Disorders. 2023. doi:10.1016/j.parkreldis.2023.105476
- Conti M, et al. Brain functional connectivity in de novo Parkinson’s disease patients based on EEG. Human Brain Mapping. 2024. doi:10.1002/hbm.26689
- Jain S. Multi-organ autonomic dysfunction in Parkinson disease. Parkinsonism & Related Disorders. 2011. doi:10.1016/j.parkreldis.2010.08.025