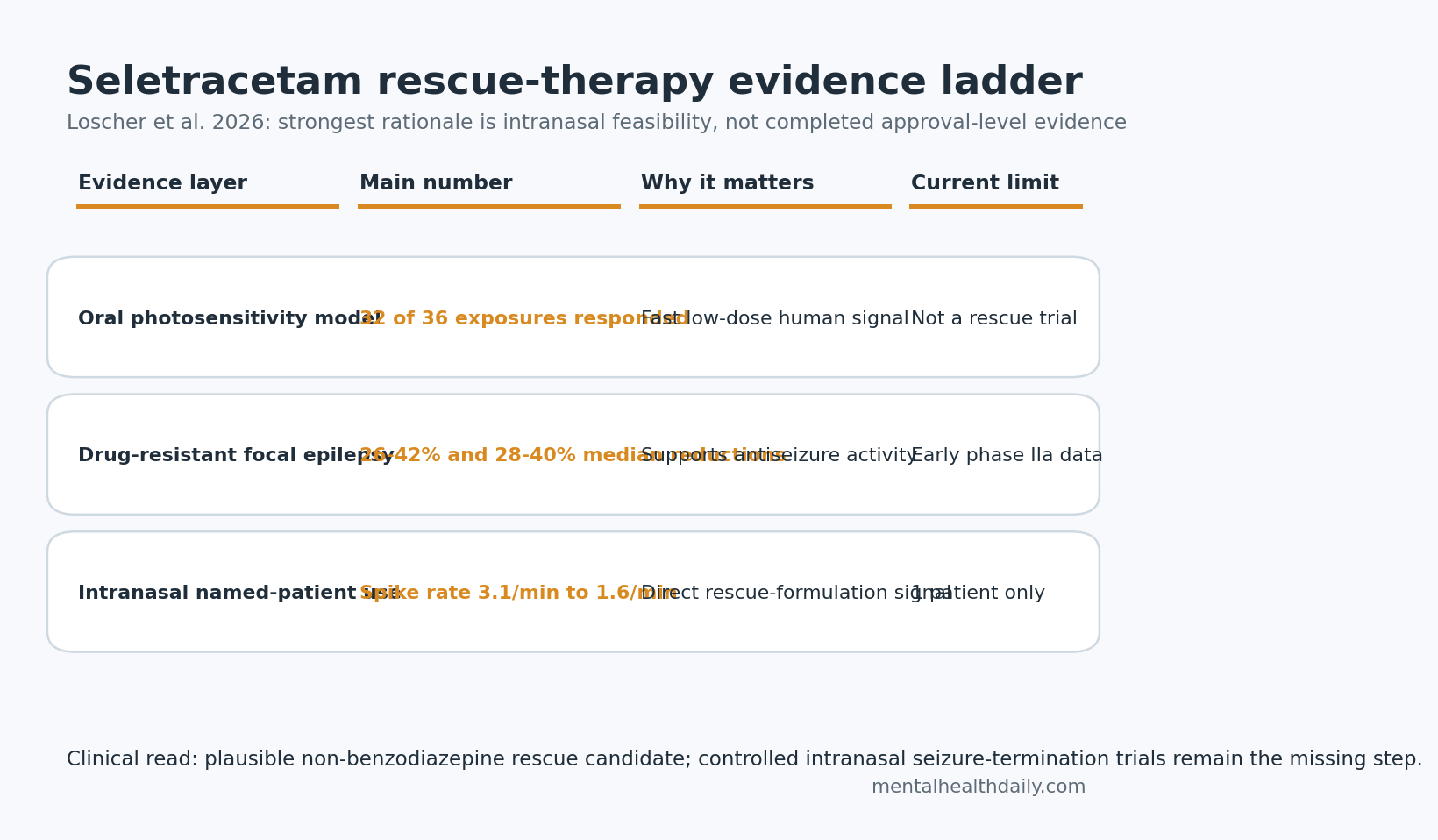
A 2026 CNS Drugs review argues that seletracetam, an abandoned second-generation racetam antiseizure drug, may be unusually well suited for seizure rescue: early oral studies involved 171 participants, photosensitivity responses occurred in 32 of 36 exposures, and one intranasal named-patient use reduced reading-induced spike rate from 3.1/min to 1.6/min without sedation.
Research Highlights
- Rescue-therapy rationale: seletracetam combines high antiseizure potency with water solubility, allowing a proposed 10-40 mg intranasal dose per nostril rather than an oral tablet.
- Photosensitivity signal: a phase IIa proof-of-concept study reported partial or complete photoparoxysmal-response suppression in 32 of 36 exposures across 0.5-20 mg oral doses.
- Focal-epilepsy data: 2 early add-on studies in drug-resistant focal epilepsy reported median seizure-frequency reductions of 26-42% and 28-40% across 20-160 mg/day dose periods.
- Benzodiazepine contrast: seletracetam is proposed as a non-benzodiazepine rescue option because approved intranasal benzodiazepines carry strict limits such as no more than 5 episodes per month.
- Evidence limit: intranasal seletracetam is not an approved rescue medication; the current human intranasal evidence is 1 named-patient use plus older oral early-phase datasets.
Seizure rescue therapy means medication used outside the daily maintenance schedule to stop seizure clusters, prolonged seizures, or predictable reflex seizures before they become emergencies. Current rescue care still leans heavily on benzodiazepines such as intranasal midazolam and diazepam, which work quickly but can bring sedation, respiratory caution, dependence concerns, and dosing-frequency restrictions.
Synaptic vesicle glycoprotein 2A (SV2A) is a protein on presynaptic vesicles that helps regulate neurotransmitter release. Levetiracetam, brivaracetam, and seletracetam all bind SV2A, but the 2026 review makes a narrower claim: seletracetam may be rescue-relevant because it is potent enough, soluble enough, and apparently tolerable enough to fit into an intranasal formulation.
Seletracetam Was Dropped for Chronic Epilepsy, Not Because It Looked Inactive
Seletracetam came from the same racetam-development program that produced levetiracetam and brivaracetam. UCB advanced brivaracetam into phase III trials and eventual US Food and Drug Administration approval for focal-onset seizures, while seletracetam stayed behind as a backup compound and its original patent expired in 2021.
That history can make seletracetam look like a failed drug. Loscher et al. read it differently. The compound showed stronger potency than levetiracetam and brivaracetam in several acquired and genetic epilepsy models, especially amygdala-kindled rats, where the minimum active dose for focal and secondary generalized seizure thresholds was 0.0074 mg/kg. In the same review’s comparative table, levetiracetam and brivaracetam required much higher doses in that model.
Mechanistic profile: seletracetam pairs higher SV2A affinity with several additional pharmacologic signals. The review describes SV2A binding, inhibition of high-voltage-activated calcium channels, reversal of zinc inhibition at glycine-gated currents, and possible glutamate-transporter effects. Those mechanisms do not prove clinical superiority, but they explain why the drug could behave differently from levetiracetam even when both target SV2A.
Photosensitive Epilepsy Data Showed a Fast Low-Dose Human Signal
Photosensitive epilepsy is a reflex-epilepsy model in which intermittent light stimulation can trigger a photoparoxysmal electroencephalographic response, or abnormal EEG activity provoked by flashing light. Drug developers use this model because suppression of that response can give an early human signal for antiseizure activity before large clinical trials are run.
The seletracetam proof-of-concept study tested single oral doses from 0.5 mg to 20 mg in 27 evaluable participants, with 9 participants reentering for a second exposure. Across 36 exposures, the review reports a response in 32 exposures. Complete suppression occurred in 40-71% of participants, depending on dose.
Low-dose potency: some participants showed photoparoxysmal-response suppression at 0.5 mg, where maximal plasma concentration was around 13 ng/mL. The review states that seletracetam was at least 1500 times more potent than levetiracetam and 10-20 times more potent than brivaracetam in this photosensitivity model.
Levetiracetam comedication: the response did not disappear in participants already taking levetiracetam. Complete suppression was numerically lower with levetiracetam comedication than with no antiseizure comedication, but the difference was not statistically confirmed, and 78% of exposures on levetiracetam still had a partial or complete response.
Focal-Epilepsy Studies Were Promising, But Not Pivotal Evidence
The review summarizes 2 phase IIa add-on studies in adults with drug-resistant focal epilepsy. Drug-resistant focal epilepsy means seizures that start in one brain network or region and persist despite antiseizure medication; these are exactly the patients in whom rescue medication may be needed even when maintenance treatment continues.
The first available focal-epilepsy study enrolled 59 adults and tested oral seletracetam capsules as adjunctive therapy over an 11-week period after a 4-week baseline. Median seizure-frequency reductions during up-titration were 26% at 20 mg/day, 32% at 40 mg/day, 42% at 80 mg/day, and 32% at 160 mg/day.
A second study involving 31 participants reported median seizure-frequency reductions of 40%, 37%, 28%, and 40% across the same 20-160 mg/day dose range. During week 8, 3% of participants had more than 75% but less than 100% seizure-frequency reduction, and 6.5% were seizure-free.
Evidence-strength note: these were early phase IIa/open-label or incompletely published datasets, not definitive modern registration trials. They support biological plausibility and dose-range selection. They do not establish seletracetam as an approved chronic antiseizure medication or as a proven rescue substitute.
Intranasal Seletracetam Is the Real Revival Argument
The strongest reason to revisit seletracetam is not chronic oral therapy. It is formulation. Intranasal rescue drugs must fit meaningful doses into roughly 100-150 microliters per nostril. Many antiseizure medications are either not potent enough or not soluble enough for that route.
Loscher et al. report that PrevEp developed a mucoadhesive phosphate-buffered aqueous intranasal formulation using hydroxyethylcellulose as a gel-forming agent. At 200 mg/mL, the selected solution could deliver 30 mg in 150 microliters, with the review describing a target intranasal range of 10-40 mg per nostril.
- Volume fit: the proposed dose fits the small volume the nasal cavity can tolerate.
- Solubility fit: high water solubility allows a concentrated aqueous spray rather than a bulky suspension.
- Rescue fit: potency at low doses is the reason an intranasal route is plausible for a non-benzodiazepine antiseizure drug.
Named-patient signal: the first described intranasal use involved a 42-year-old man with reading epilepsy, a reflex epilepsy in which reading triggered facial myoclonic seizures. After placebo nasal administration, the first seizure occurred at 1:56 after reading began, and reading was stopped after the third clear seizure around 4 minutes.
After 30 mg intranasal seletracetam in the left nostril, the first reading-induced seizure was delayed to 4:17. After a second 30 mg dose in the right nostril, the patient read for another 25 minutes without self-reported seizures.
Magnetoencephalography showed spike rate declining from 3.1/min after placebo to 1.9/min after the first dose and 1.6/min after the second dose. Activity also stayed more localized after seletracetam instead of propagating through the broader epileptic network.
The tolerability signal was narrow but clean: transient mild bitter taste after the first dose, no other adverse events, and no sedation. Serum levels rose from 70 ng/mL to 260 ng/mL immediately after the second dose and 500 ng/mL around 27 minutes later.
Benzodiazepines Remain the Benchmark Seletracetam Has to Beat
Benzodiazepines enhance GABAA receptor signaling, increasing inhibitory tone in the brain. That mechanism can terminate seizures quickly, which is why intranasal midazolam and diazepam are established rescue options. The same pharmacology also explains sedation and respiratory caution.
Seletracetam’s proposed advantage is different pharmacology rather than faster proof of efficacy. It has no known addictive potential in the way benzodiazepines do, and the review emphasizes the absence of respiratory depression and only moderate sedation even at the highest oral doses tested. That profile would matter most for patients who need repeated rescue dosing or who are vulnerable to benzodiazepine adverse effects.
A fair comparison has to stay calibrated:
- Benzodiazepines: approved, clinically familiar, and fast-acting, but limited by sedation, respiratory-risk warnings, dependence concerns, and monthly use limits.
- Seletracetam: pharmacologically attractive and formulation-compatible, but still unapproved and not yet tested in controlled intranasal rescue trials.
- Optimal next test: randomized rescue-therapy studies measuring seizure termination, recurrence, sedation, respiratory outcomes, caregiver usability, and need for emergency escalation.
Development read: the strongest near-term niche is seizure clusters or predictable reflex seizures where a patient needs fast rescue without benzodiazepine-level sedation. That niche still needs pharmacokinetic data, dose-ranging, caregiver administration testing, and controlled comparison against approved intranasal benzodiazepines.
A rescue program should also report practical outcomes: time to usable dosing, repeat-dose need, emergency-service use, and whether patients stay alert enough to recover safely.
Questions About Seletracetam for Seizure Rescue
Is seletracetam available as a seizure rescue medication?
No. Seletracetam has not been approved for human use. The 2026 review argues for renewed development, especially intranasal rescue development, but clinical use still requires controlled trials and regulatory review.
Why was seletracetam not developed earlier?
UCB developed seletracetam and brivaracetam in parallel, then moved brivaracetam forward into larger phase III trials. The review presents seletracetam as a drug left behind by portfolio strategy, not as a compound abandoned because early data showed no antiseizure activity.
Would seletracetam replace intranasal midazolam or diazepam?
Not on current evidence. The practical target is a non-benzodiazepine alternative for seizure clusters or rapid seizure termination, especially where sedation and repeated benzodiazepine exposure are problems. Replacement claims require head-to-head rescue trials.
References
- Loscher W, Rundfeldt C, Trinka E, Koepp M, Klein P. Seletracetam Revisited: A Missed Opportunity for Effective Epilepsy Therapy. CNS Drugs. 2026;40:603-622. doi:10.1007/s40263-026-01281-0
- Bennett B, Matagne A, Michel P, Leonard M, Cornet M, Meeus MA, et al. Seletracetam (UCB 44212). Neurotherapeutics. 2007;4:117-122. PubMed
- Matagne A, Margineanu DG, Potschka H, Loscher W, Michel P, Kenda B, et al. Profile of the new pyrrolidone derivative seletracetam (ucb 44212) in animal models of epilepsy. European Journal of Pharmacology. 2009;614:30-37. PubMed
- Klitgaard H, Matagne A, Nicolas JM, Gillard M, Lamberty Y, De Ryck M, et al. Brivaracetam: rationale for discovery and preclinical profile of a selective SV2A ligand for epilepsy treatment. Epilepsia. 2016;57:538-548. PubMed
- Schmitz A. Benzodiazepine use, misuse, and abuse: a review. Mental Health Clinician. 2016;6:120-126. doi:10.9740/mhc.2016.05.120
- Mohammed MZ, Elagouza I, El Gaafary M, El Garhy R, El Rashidy O. Intranasal versus buccal versus intramuscular midazolam for the home and emergency treatment of acute seizures in pediatric patients: a randomized controlled trial. Pediatric Neurology. 2024;158:135-143. PubMed