
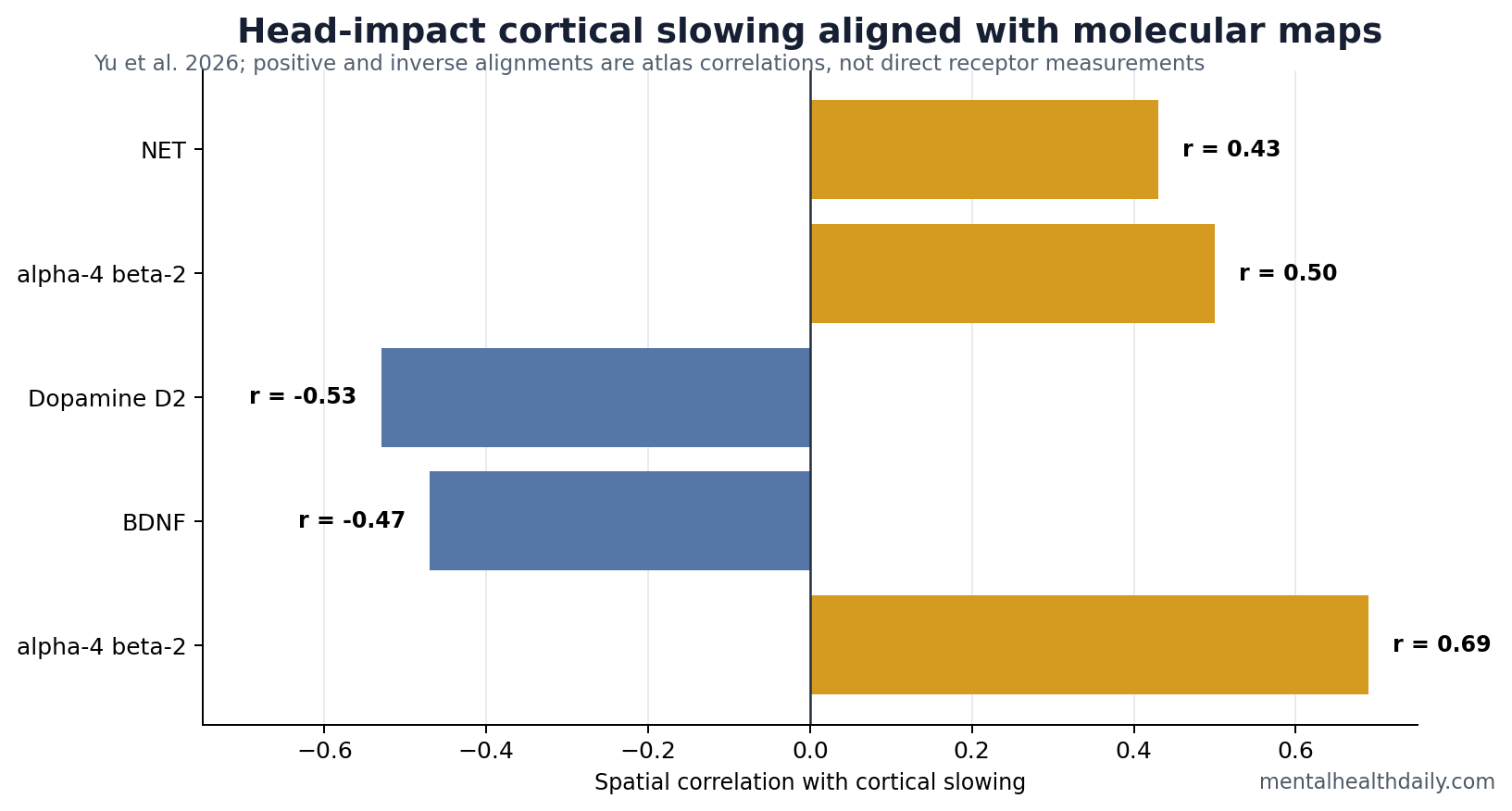
A 91-player adolescent football preprint mapped head-impact-related cortical slowing onto brain receptor and gene-expression maps: concussion-related slowing aligned with norepinephrine transporter density, r = 0.43, and alpha-4 beta-2 nicotinic receptor density, r = 0.50, while aligning inversely with dopamine D2, BDNF, and APOE maps.1 The result is a mechanistic clue about where head-impact physiology may land in the cortex, not a ready clinical test for individual players.
Research Highlights
- Concussion slowing tracked arousal maps: Diagnosed-concussion cortical slowing aligned with norepinephrine transporter density, r = 0.43, pFDR = 0.001.1
- Nicotinic receptor alignment reached r = 0.50: Alpha-4 beta-2 nicotinic receptor density aligned with concussion-related slowing, r = 0.50, pFDR = 0.001.1
- Dopamine and serotonin maps pointed the other way: Dopamine D2 alignment was inverse, r = −0.53, pFDR = 0.001, with several serotonin maps also inverse.1
- BDNF and APOE were inverse signals: BDNF expression aligned inversely with concussion slowing, r = −0.47, and APOE also showed an inverse relationship, r = −0.26.1
- Symptom-linked slowing had its own map: Cognitive-symptom slowing aligned with alpha-4 beta-2 receptors at r = 0.69, pFDR = 0.001.1
Aperiodic cortical activity is the broadband background slope of brain electrical or magnetic signals. In plain language, it describes a general slowing or shifting of population-level brain activity rather than a single named rhythm such as alpha or beta.
Yu et al. used magnetoencephalography, or MEG, which records magnetic fields generated by neural activity. The researchers then compared pre-to-post-season cortical slowing patterns with published maps of neurotransmitter receptors and gene expression. That method can suggest which biological systems live in affected cortical territories, but it does not directly measure norepinephrine, dopamine, BDNF, or APOE inside the players’ brains.
91 Players Created 2 Injury Questions
The study followed 91 adolescent male football players. Ten had a diagnosed concussion, while 71 non-concussed players had complete imaging and exposure data for non-concussive head-impact analyses.1
Those 2 groups answer different questions. Diagnosed concussion asks what happens around clinically recognized injury. Non-concussive exposure asks whether repeated impacts below the diagnostic threshold leave a measurable cortical signature.
Evidence-strength note: the diagnosed-concussion subgroup was small, and all players were adolescent males in football. The paper is valuable for mechanistic mapping, but it should not be stretched into universal return-to-play guidance.
Concussion Slowing Aligned With Norepinephrine and Nicotine-Receptor Maps
The strongest positive alignments were with receptor systems involved in arousal, attention, and cortical state regulation. Norepinephrine transporter density aligned with concussion-related slowing at r = 0.43, pFDR = 0.001. Alpha-4 beta-2 nicotinic receptor density aligned at r = 0.50, pFDR = 0.001.1
Norepinephrine transporters help regulate norepinephrine signaling, a system involved in alertness and stress arousal. Alpha-4 beta-2 nicotinic receptors respond to acetylcholine and nicotine and are involved in attention networks. The spatial result points toward cortical systems that help set vigilance and attention.
Inverse Dopamine, Serotonin, BDNF, and APOE Maps Complicate the Read
Several alignments ran in the negative direction. Dopamine D2 receptor density showed an inverse relationship with concussion slowing, r = −0.53, pFDR = 0.001. Serotonin 5-HT4, 5-HT1A, serotonin transporter, and 5-HT2A maps were also inverse.1
BDNF (brain-derived neurotrophic factor) is a growth-support factor for neurons and synapses. BDNF expression was inversely related to concussion slowing, r = −0.47, pFDR = 0.001. APOE is a lipid-transport gene with known relevance to brain injury and neurodegenerative vulnerability; APOE expression also showed an inverse relationship, r = −0.26, pFDR = 0.029.1
Inverse alignment means slowing was spatially stronger where those atlas measures were lower. The biological interpretation still needs experimental work beyond spatial correlation.
Head-Impact Exposure Without Concussion Had a Smaller Signature
Non-concussive exposure still produced map relationships, but the pattern was narrower. Non-concussive head-impact-related slowing aligned inversely with 5-HT1A receptor density, r = −0.36, pFDR = 0.034, APOE, r = −0.26, pFDR = 0.040, and BDNF, r = −0.24, pFDR = 0.040.1
That pattern fits the broader sports-concussion literature: biomechanical exposure may produce functional brain changes before structural scans show obvious injury, but the clinical meaning of those changes depends on symptoms, recovery trajectory, and repeated assessment.2
Neurometabolic models of concussion already emphasize ionic shifts, energy demand, neurotransmitter disturbance, and vulnerability during recovery.3 The Yu study adds a spatial molecular hypothesis: the cortical territories that slow after impact may overlap with specific arousal, cholinergic, serotonin, dopamine, neurotrophic, and genetic landscapes.
Atlas Colocalization Is a Hypothesis Generator
Supported: cortical slowing after diagnosed concussion and repeated head-impact exposure was not randomly distributed across the cortex. It aligned with several published molecular maps.
Not supported: individual diagnosis, direct receptor measurement, medication targeting, or return-to-play decisions based on atlas correlations. Aperiodic spectral measures are useful, but they are still indirect markers of neural population activity.4
Best next test: larger longitudinal samples should combine MEG, symptoms, blood or imaging biomarkers, sex-inclusive cohorts, and recovery follow-up to test whether these map alignments predict persistent cognitive or mood outcomes.
Cognitive Symptoms May Track Arousal-State Networks
The symptom-linked analysis is clinically relevant because cognitive complaints after concussion often sound diffuse: slowed thinking, fogginess, poor concentration, fatigue, and trouble keeping up in school. Yu et al. found that cognitive-symptom-linked slowing aligned with several systems involved in cortical state regulation, including NET, VAChT, 5-HT1B, alpha-4 beta-2 nicotinic receptors, and H3 maps.1
VAChT is the vesicular acetylcholine transporter, a marker related to acetylcholine signaling. Histamine H3 receptors help regulate wakefulness and neurotransmitter release. These systems fit the subjective symptom cluster better than a purely structural injury model because attention, alertness, and mental energy are state-dependent functions.
The data do not identify a treatment target. They suggest that post-impact cognitive symptoms may involve arousal and neuromodulatory systems alongside local tissue injury. That framing could help explain why sleep, exertion, school load, mood, and symptom provocation often interact during recovery.
Exposure Mapping Needs Symptom and Recovery Follow-Up
Non-concussive impact findings are the easiest part of this literature to overstate. A spatial correlation between exposure-related slowing and BDNF, APOE, or serotonin maps does not tell a parent, coach, or clinician whether one player will have persistent symptoms. It says repeated exposure can leave a measurable group-level cortical pattern that deserves follow-up.
Better outcome anchors: days to symptom resolution, school accommodations, exertion tolerance, sleep change, headache persistence, mood symptoms, and objective cognitive recovery. Without those anchors, atlas maps remain mechanistic context rather than clinical prediction.
Future studies should also include female athletes and non-football sports. The biology of impact exposure may overlap across sports, but helmeted male football is not the full adolescent concussion population. Sex, sport, impact direction, prior concussion history, and recovery management can all affect the final clinical picture.
Study timing also needs sharper resolution. Pre-season and post-season MEG can show that a cortical state changed, but it cannot fully separate acute injury, cumulative exposure, recovery, sleep loss, and practice load. More frequent measurement after diagnosed concussion would show whether receptor-map alignment fades with recovery or persists in players with prolonged symptoms.
Clinical bridge: MEG slowing should be paired with school performance, symptom diaries, exertion testing, and sleep metrics. If cortical slowing aligned with arousal-state maps also predicts slow return to learning, the molecular-map result becomes more than an atlas observation. It becomes a candidate pathway for why some adolescents feel cognitively stuck after head impacts.
The receptor-map layer also needs guardrails around medication inference. Norepinephrine, nicotinic, serotonin, dopamine, BDNF, and APOE maps are anatomical reference surfaces, separate from treatment-response experiments. A positive or inverse spatial alignment leaves unanswered whether a drug acting on that receptor system would improve recovery, worsen recovery, or target the same biology in an injured adolescent brain.1
For now, the actionable signal stays behavioral and operational: reduce avoidable head impacts, report symptoms early, track cognitive load during school return, and use repeated clinical assessment when recovery is slow. The molecular atlas helps explain where to look next; lower-tech safeguards remain the practical layer.
The safest public-health interpretation is therefore cautious but concrete. Repeated head impacts may affect cortical state systems even when diagnosed concussion is absent, and diagnosed concussion may engage arousal and cholinergic territories that fit cognitive symptoms. Prevention, reporting, recovery monitoring, and honest symptom tracking remain more actionable than trying to medicate a receptor-map correlation.
This is also where school context belongs. Adolescents recover inside classrooms, homework schedules, sleep restriction, screens, social pressure, and sport identity. A brain-state marker that ignores those recovery conditions will have limited clinical value even if the atlas correlation is statistically strong.
Recovery is biological and operational.
Questions About Football Head Impacts and Cortical Slowing
Does this prove football changes neurotransmitters?
No. The study mapped MEG slowing onto published receptor and gene maps. It did not directly measure neurotransmitter levels in the players.
Why does aperiodic slowing matter?
Aperiodic slowing can reflect broad changes in neural population state. In head injury research, it may capture functional brain disturbance that conventional structural imaging misses.
Can this guide return-to-play decisions?
No. The sample and method are not ready for individual clearance decisions. Clinical recovery still requires symptom, neurologic, cognitive, and medical assessment.
References
- Yu X, et al. Neurochemical and genetic organization of cortical slowing following head impact exposure in adolescent football players. medRxiv. 2026. doi:10.64898/2026.04.09.26350342
- McCrory P, Meeuwisse W, Dvorak J, et al. Consensus statement on concussion in sport. British Journal of Sports Medicine. 2017. doi:10.1136/bjsports-2017-097699
- Giza CC, Hovda DA. The new neurometabolic cascade of concussion. Neurosurgery. 2014. doi:10.1227/neu.0000000000000505
- Voytek B, Kramer MA, Case J, et al. Age-related changes in 1/f neural electrophysiological noise. Journal of Neuroscience. 2015. doi:10.1523/jneurosci.2332-14.2015