
A 2026 retrospective ICU study found that 24-hour family visiting was associated with lower delirium in chronic critical patients than 1-hour restricted visiting: 11.36% vs. 25.76%.1 The same open-visiting group also had lower discharge HADS anxiety-depression scores, shorter ventilation, and no measurable worsening in sampled ICU air quality, but the time-based single-center design keeps the finding in the “promising policy signal” category rather than the “settled causal rule” category.
Research Highlights
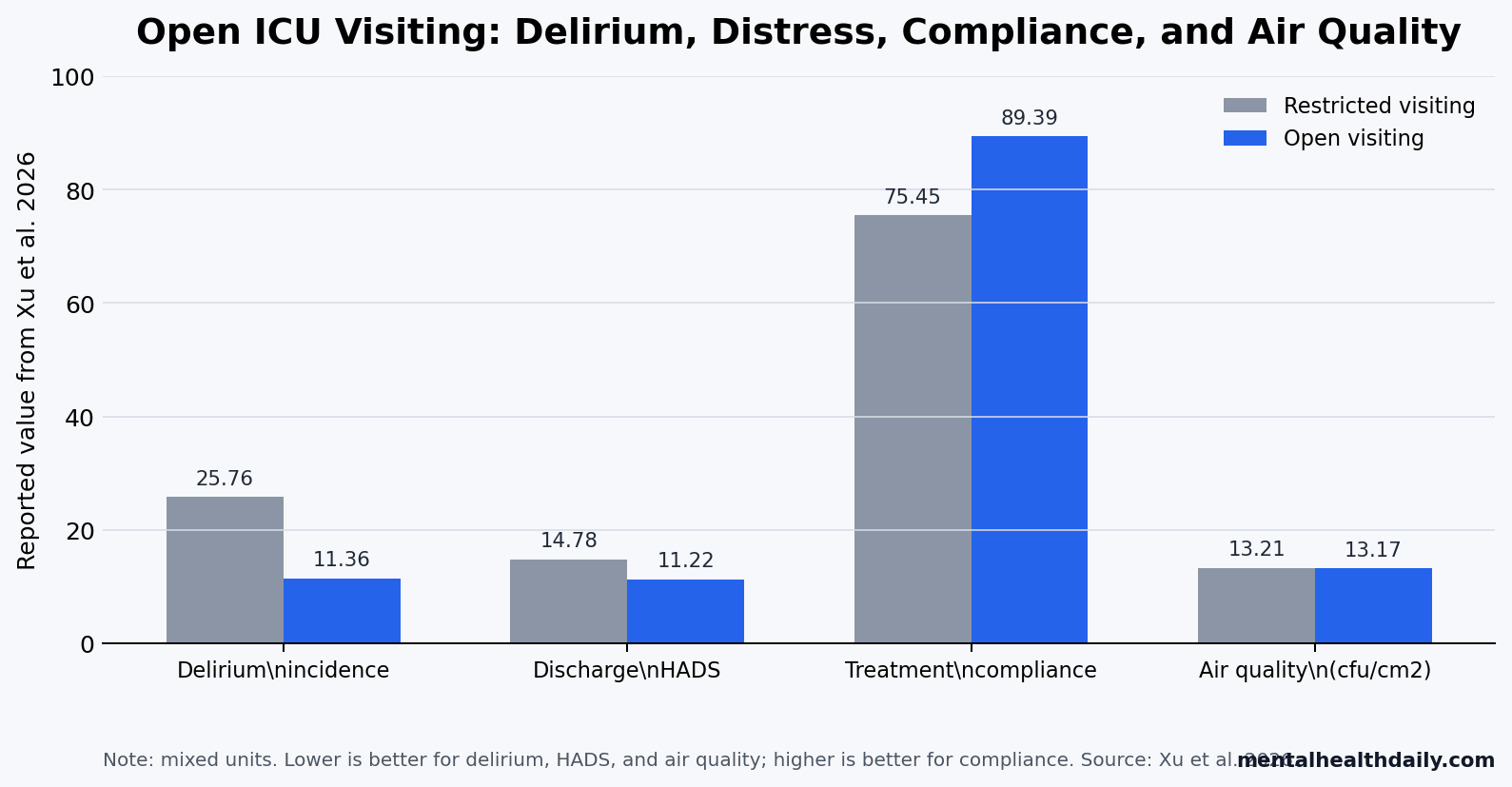
- Delirium was lower with open visiting: 15 of 132 open-visiting patients had delirium vs. 34 of 132 restricted-visiting patients, or 11.36% vs. 25.76%.
- Patient distress moved in the same direction: discharge HADS scores were 11.22 ± 1.96 with open visiting vs. 14.78 ± 2.25 with restricted visiting.
- Family anxiety also fell: family state-anxiety scores were 44.23 ± 2.17 vs. 56.89 ± 2.88, and trait-anxiety scores were 44.18 ± 1.89 vs. 57.54 ± 3.11.
- Clinical recovery markers favored open access: ventilation averaged 15.44 vs. 18.88 days, ICU stay averaged 12.17 vs. 15.91 days, and treatment compliance was 89.39% vs. 75.45%.
- Infection-control concern was not confirmed by air sampling: measured ICU air quality was 13.17 vs. 13.21 cfu/cm², a nonsignificant difference under strict hand-hygiene and masking rules.
Open ICU visiting means allowing family members to visit beyond a short fixed window, usually with infection-control screening, protective equipment, and bedside rules. In Xu et al., the restricted group had a daily 15:00 to 15:30 visiting period, while the open group allowed family access at any time over 24 hours, usually 1 visitor at a time and not during invasive procedures.1
Chronic critical illness refers to a prolonged ICU state with persistent organ dysfunction, extended dependence on intensive support, and high exposure to sleep disruption, sedation, immobility, fear, and family separation. That population is psychologically different from a short postoperative ICU stay: delirium risk, family distress, and rehabilitation cooperation can become part of the treatment environment itself.
Open Visiting Cut Delirium From 25.76% to 11.36%
Xu et al. analyzed 264 chronic critical ICU patients admitted between January 2025 and January 2026 at a tertiary hospital in Foshan, China. The restricted-visiting control group included 132 patients, and the open-visiting group included 132 patients after the ICU changed its visiting policy in December 2025.1
Baseline severity looked similar. Mean age was about 53 years in both groups, sex distribution was similar, APACHE II scores were 30.54 vs. 30.71, and recorded underlying disease categories did not differ significantly.
Delirium measurement: nurses assessed delirium twice daily with the Confusion Assessment Method for the ICU (CAM-ICU), a bedside tool for detecting acute attention and consciousness changes in critically ill patients. A senior intensivist verified positive findings, and the paper reported an inter-rater kappa of 0.85, which suggests strong agreement among assessors.
Delirium incidence was 11.36% in the open-visiting group and 25.76% in the restricted-visiting group. Framed as absolute risk, the difference was about 14.4 percentage points. Framed as relative risk, open visiting was associated with roughly 56% lower observed delirium incidence.
That is a large policy signal, but not a clean randomized effect. Because the groups were separated by implementation time, any unmeasured change in staffing, sedation practice, case mix, family behavior, or documentation could have contributed. The article’s useful claim is narrower: chronic critical patients did not obviously need family restriction to protect ICU stability, and the measured neuropsychiatric outcomes favored structured access.
HADS and Family Anxiety Scores Favored Open Access
HADS is the Hospital Anxiety and Depression Scale, a 14-item symptom scale often used in medical settings because it avoids many somatic symptoms that overlap with physical illness. Admission HADS scores were similar in the 2 groups: 17.85 ± 1.25 with restricted visiting vs. 17.94 ± 1.31 with open visiting.
By discharge, HADS scores separated. Open-visiting patients averaged 11.22 ± 1.96 points, compared with 14.78 ± 2.25 points in the restricted-visiting group. That pattern fits the simple psychological pathway: familiar people can reduce threat, confusion, loneliness, and helplessness in an ICU environment that otherwise strips patients of normal cues.
Family anxiety moved even more visibly. State anxiety, which captures current anxiety, averaged 44.23 ± 2.17 in the open-visiting group vs. 56.89 ± 2.88 in the restricted-visiting group. Trait anxiety, which reflects more stable anxiety tendency, averaged 44.18 ± 1.89 vs. 57.54 ± 3.11.
de Souza et al. reported 12-month family mental-health follow-up after flexible ICU visitation, which keeps the family side of visitation from being a soft endpoint. A visiting policy changes the patient’s sensory and emotional environment, but it also changes the family’s exposure to uncertainty, helplessness, and post-ICU psychological burden.3
Clinical Recovery Markers Also Moved With Visitation
Open visiting was associated with shorter ICU recovery markers:
- Mechanical ventilation: 15.44 ± 1.28 days with open visiting vs. 18.88 ± 3.47 days with restricted visiting.
- ICU stay: 12.17 ± 3.33 days vs. 15.91 ± 3.78 days.
- Total hospital stay: 20.22 ± 3.16 days vs. 25.11 ± 5.11 days.
- Treatment compliance: 89.39% vs. 75.45%, using an 80% completion threshold across medication administration, early mobilization, and respiratory therapy sessions.
The compliance endpoint is clinically plausible. Family presence can help patients understand where they are, tolerate respiratory therapy, cooperate with mobilization, and accept unpleasant but necessary care. It can also give staff a better source of patient-specific behavioral cues.
Rosa et al. provide the necessary counterweight. In the ICU Visits randomized clinical trial, flexible family visitation did not significantly reduce delirium among a broader ICU population.2
That does not erase the Xu et al. result; it calibrates it. The stronger interpretation is not “open visiting always prevents delirium,” but “the effect may depend on population, protocol, family participation, baseline restriction, and how much the visiting policy changes daily care.”
Air Quality Did Not Worsen Under Structured Infection Control
The common argument for ICU visitor restriction is not irrational. ICU patients are medically fragile, procedures are frequent, privacy matters, and uncontrolled traffic can make work harder. Infection risk is the most obvious concern.
Xu et al. directly measured airborne bacterial counts twice weekly. Air quality was statistically similar: 13.17 ± 1.05 vs. 13.21 ± 1.11 cfu/cm². That finding only applies under the protocol they used: masks, shoe covers, hand disinfection, daily nursing supervision, twice-weekly infection-control spot checks, and a reported hand-hygiene compliance rate of 94.8%.1
Implementation boundary: “open visiting” in this study did not mean unlimited unmanaged bedside traffic. It meant broad access inside a controlled procedure. ICUs with weak staffing, poor hand-hygiene monitoring, crowding, or high-transmission outbreaks should not treat this paper as a license to ignore local infection-control constraints.
The Evidence Supports Structured Access, Not a Universal Mandate
Sahawneh and Boss reviewed nonpharmacologic ICU delirium-prevention approaches, reinforcing the broader point that delirium is a systems problem: sleep, orientation, mobility, pain, sedation, communication, and family engagement can all shape risk.4 Kotfis et al. similarly framed ICU delirium as a preventable and manageable problem rather than an unavoidable side effect of critical illness.5
Family presence fits that prevention model because it adds orientation, emotional safety, behavioral interpretation, and early recognition of mental-status changes. The effect should be strongest where patients are conscious enough to perceive family presence, family members can follow infection-control rules, and staff can integrate visitors without losing clinical control.
Evidence-strength note: Xu et al. used a retrospective single-center design with a before-after policy boundary. The data can support a strong local association and a policy hypothesis. It cannot prove that visitation alone caused the lower delirium rate, and it cannot prove that every ICU in every culture will reproduce the same effect.
Default restriction now carries its own burden of proof. If an ICU limits family presence to a narrow daily window, the reason should be specific: outbreak control, procedure privacy, staffing constraints, patient preference, safety, or a clearly defined operational problem. “Families are disruptive” is too broad when structured open visiting correlated with better delirium and anxiety outcomes without worse measured air quality in this chronic critical cohort.
Questions About ICU Open Visiting, Delirium, and Anxiety
Did open ICU visiting prevent delirium in this study?
Open visiting was associated with lower delirium incidence, but the design cannot prove prevention. The open group had 15 delirium cases among 132 patients, compared with 34 among 132 restricted-visiting patients.
Was the open-visiting policy uncontrolled?
No. Visitors used masks, shoe covers, hand hygiene, nursing supervision, infection-control spot checks, and usually 1 visitor at a time. The policy was open in time access, not loose in infection-control rules.
Does this mean every ICU should allow 24-hour visiting?
No. The result supports structured family access as a serious delirium and anxiety intervention, especially for chronic critical patients. Local staffing, infection-control capacity, procedure privacy, patient preference, and outbreak status still matter.
Why did family anxiety matter in a patient-outcome article?
Family members often become interpreters, motivators, and post-discharge caregivers for chronic critical patients. Lower family anxiety may improve bedside communication and care participation, while also reducing the psychological burden that continues after ICU discharge.
What would make the evidence stronger?
A multicenter prospective trial with concurrent randomization, long-term cognitive and quality-of-life follow-up, sedation exposure tracking, staffing measures, infection events, and a virtual-visiting comparison would separate the visitation effect from time trends and local ICU culture.
References
- Xu C, Zhao C, Deng C, Jin Z. Comparison of open visiting and restricted visiting in ICU chronic critical patients: effects on negative emotions and delirium. International Journal of General Medicine. 2026;19. doi:10.2147/IJGM.S595535
- Rosa RG, Falavigna M, da Silva DB, et al. Effect of flexible family visitation on delirium among patients in the intensive care unit: the ICU Visits randomized clinical trial. JAMA. 2019;322(3):216-228. doi:10.1001/jama.2019.8766
- de Souza JMB, Miozzo AP, Da Rosa Minho Dos Santos R, et al. Long-term effects of flexible visitation in the intensive care unit on family members’ mental health: 12-month results from a randomized clinical trial. Intensive Care Medicine. 2024;50(10):1614-1621. doi:10.1007/s00134-024-07577-3
- Sahawneh F, Boss L. Non-pharmacologic interventions for the prevention of delirium in the intensive care unit: an integrative review. Nursing in Critical Care. 2021;26(3):166-175. doi:10.1111/nicc.12594
- Kotfis K, van Diem-Zaal I, Williams Roberson S, et al. The future of intensive care: delirium should no longer be an issue. Critical Care. 2022;26(1):200. doi:10.1186/s13054-022-04077-y
- Mart MF, Williams Roberson S, Salas B, et al. Prevention and management of delirium in the intensive care unit. Seminars in Respiratory and Critical Care Medicine. 2021;42(1):112-126. doi:10.1055/s-0040-1710572