Major upper-extremity amputation was linked to substantially higher odds of new mental-health diagnosis, antidepressant initiation, and psychotherapy claims than minor upper-extremity amputation in a matched national database study. The clearest clinical implication is early mental-health screening after major limb loss, not waiting for distress to surface months later.1
Research Highlights
- 2,452 matched patients were analyzed: the PearlDiver study compared 1,226 major and 1,226 minor upper-extremity amputations after excluding recent mental-health diagnoses or antidepressant records.1
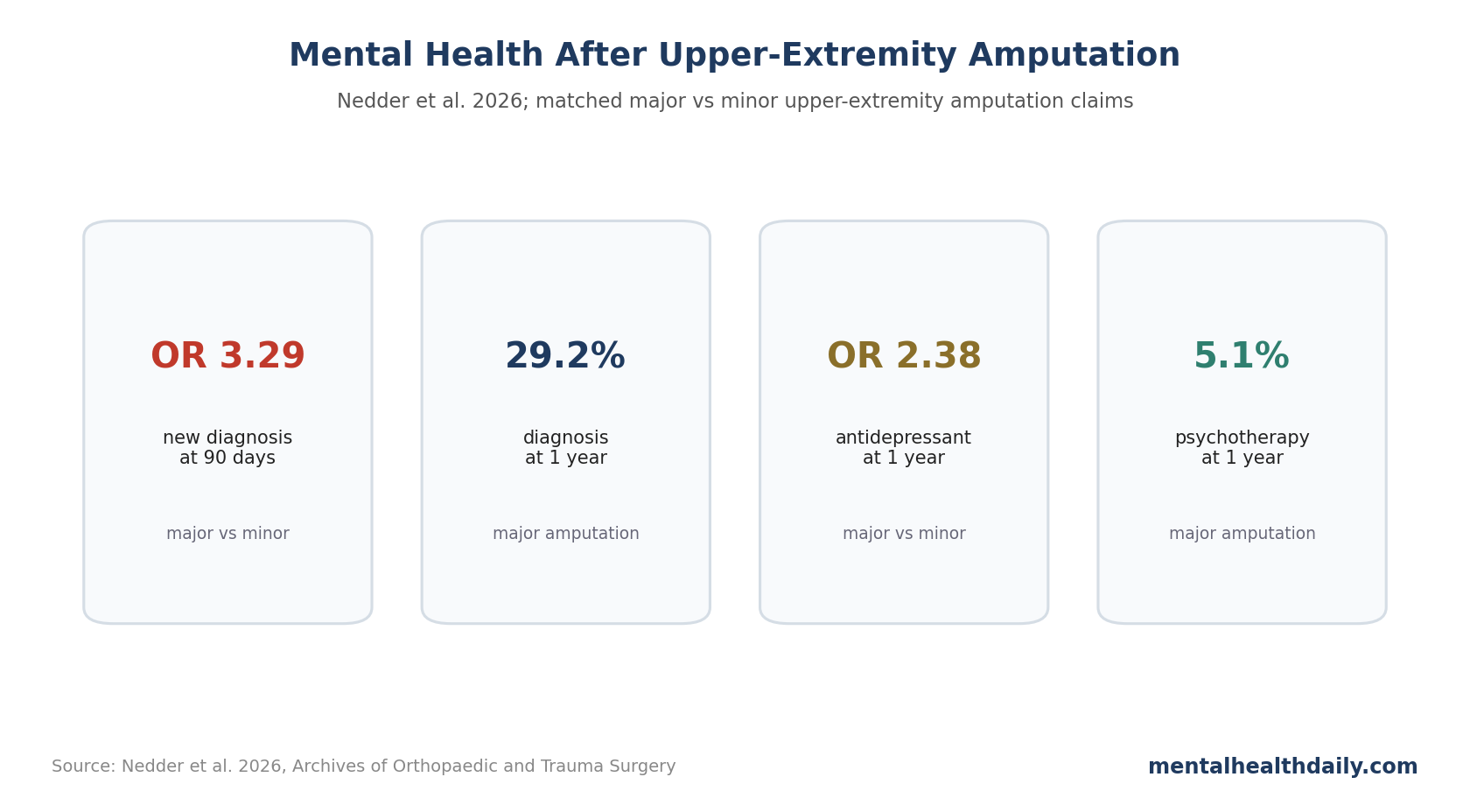
- Major amputation raised 90-day diagnosis odds: new mental-health diagnoses occurred in 18.5% vs. 6.9%, with OR = 3.29, 95% CI 2.52-4.34, p < 0.001.1
- The 1-year gap persisted: new diagnoses were 29.2% vs. 17.7%, with OR = 2.01, 95% CI 1.65-2.45, p < 0.001.1
- Treatment markers moved too: major amputation increased odds of antidepressant initiation and psychotherapy use at both 90 days and 1 year.1
- Psychotherapy looked underused: even major-amputation psychotherapy claims were only 5.1% at 1 year, despite a 29.2% new-diagnosis rate.1
This analysis connects depression prevalence with claims-based treatment behavior. It compares amputation level and then follows diagnosis, medication, and psychotherapy records, giving a rough view of how often distress is recognized and acted on in medical care.
Major vs. Minor Amputation Was Defined Anatomically
Nedder et al. used PearlDiver claims data from 2010 to 2022. Major amputations included shoulder disarticulation, arm, forearm, wrist, and transmetacarpal amputations. Minor amputations included single metacarpal, digit, and phalanx amputations.1
- Matching: groups were matched 1:1 by age range, sex, Elixhauser Comorbidity Index, and smoking history.
- Exclusions: patients with a mental-health diagnosis or antidepressant record in the prior year were excluded.
- Outcomes: new mental-health diagnoses, antidepressant prescriptions, and psychotherapy claims at 90 days and 1 year.
- Common diagnoses: depression and anxiety were the most prominent diagnosis categories after major amputation.
The exclusion rule makes the result cleaner for new-onset or newly documented care needs. It also means the study does not describe people with known preexisting mental-health conditions, who may need even more proactive support.
90-Day Mental-Health Diagnosis Odds Were 3.29x Higher
At 90 days, 18.5% of the major-amputation group had a new mental-health diagnosis, compared with 6.9% of the minor-amputation group. The adjusted odds ratio (OR) was 3.29, 95% confidence interval (CI) 2.52 to 4.34, p < 0.001.1
Depression was the most common diagnosis after major amputation, followed by anxiety. Post-traumatic stress disorder (PTSD), sleep disorder, alcohol-related disorder, and drug-related disorder also showed 90-day differences.
Antidepressant and Psychotherapy Claims Also Increased
At 90 days, antidepressant initiation was 11.7% after major amputation vs. 3.7% after minor amputation: OR = 3.82, 95% CI 2.70 to 5.53, p < 0.001.1
At 1 year, antidepressant initiation was 21.3% vs. 10.7%, OR = 2.38, 95% CI 1.89 to 3.02, p < 0.001. Selective serotonin reuptake inhibitors (SSRIs) were the most common antidepressant class in both groups.
Psychotherapy claims showed the largest relative difference but low absolute use. At 90 days, psychotherapy was 3.0% vs. 0.7%, OR = 5.47. At 1 year, it was 5.1% vs. 1.5%, OR = 4.18.1
Diagnosis Rates Rose More Than Psychotherapy Use
The 1-year pattern is clinically uncomfortable: 29.2% of major-amputation patients had a new mental-health diagnosis, but only 5.1% had psychotherapy claims. Medication use was more common than therapy, but still did not cover the full diagnosis group.
Claims data cannot tell whether patients declined therapy, lacked access, were referred but never scheduled, received non-billed support, or were treated outside the captured database. Still, the gap supports routine referral pathways instead of leaving psychological care to chance.
Hand and upper-extremity injuries affect identity, work, independence, body image, and pain. Prior literature has linked psychological distress after upper-extremity injury with poorer functional outcomes, return-to-work difficulty, and worse recovery experience.3
Screening Should Be Built Into Surgical Follow-Up
The data support a practical workflow: mental-health screening should not be treated as optional after major upper-extremity amputation. It should be embedded into postoperative care at predictable intervals.
A reasonable schedule would include screening before discharge when possible, then again around early wound follow-up, prosthetic planning, return-to-work discussions, and 3- to 12-month adaptation. Distress may not peak immediately; body image, phantom pain, disability claims, employment disruption, and family strain can evolve over months.
Screening should include more than depression. Anxiety, PTSD symptoms, sleep disruption, substance use, pain catastrophizing, suicidal thoughts, and functional avoidance can each affect recovery. The claims study captured some of those categories, but clinical screening can be more granular.
The psychotherapy gap points to a care-pathway problem. If diagnosis rates are high but therapy claims are low, surgical teams may need default referral pathways, warm handoffs, embedded psychologists, teletherapy options, or rehabilitation-based mental-health support.
The goal is not to pathologize grief after limb loss. The goal is to catch treatable distress early enough that it does not compound pain, prosthetic adaptation, work loss, and isolation.
Claims Data Capture Care, Not the Full Experience of Distress
Claims studies are powerful for scale, but they only see what gets coded, prescribed, or billed. A person may have severe grief, fear, anger, or trauma symptoms without receiving a diagnosis code.
The opposite can also happen. A diagnosis code may be used for administrative reasons, medication continuation, or brief symptoms that later resolve. Claims data give a health-system footprint, not a structured interview.
That limitation makes the psychotherapy finding more concerning, not less. If even billed diagnoses outnumber therapy claims by a wide margin, then the unmet support need may be larger than the database can show.
A better care model would connect surgery, rehabilitation, prosthetics, pain care, and mental health. Major amputation changes body function, identity, work capacity, and daily independence.
Major and Minor Amputation Capture Different Functional Burdens
The major/minor distinction captures more than anatomical level. It also approximates visibility, functional loss, prosthetic complexity, work disruption, trauma severity, and the amount of rehabilitation needed. Those downstream factors likely mediate some of the mental-health difference.
Future work should measure pain, phantom-limb symptoms, hand dominance, employment, social support, prosthetic access, legal or workers’ compensation stress, and rehabilitation intensity. Those variables would help identify which major-amputation patients need the most proactive mental-health support.
Minor Amputation Still Carried Elevated Need
The comparison emphasizes major amputation, but the minor-amputation group was still affected. At 1 year, 17.7% had a new mental-health diagnosis and 10.7% had antidepressant use. Those rates are clinically relevant.
Digit and phalanx loss can still change work capacity, hand appearance, dexterity, chronic pain, and trauma memories. Major amputation deserves the most proactive pathway, and minor amputation still warrants mental-health attention when pain, function, work, or sleep deteriorate.
Pain and Sleep May Be Key Bridges to Psychiatric Symptoms
The claims study counted sleep-disorder diagnoses, but pain and sleep likely deserve deeper measurement. Acute pain, chronic residual-limb pain, phantom-limb pain, and disturbed sleep can amplify depression, anxiety, irritability, and PTSD symptoms.
Practical screening: follow-up should ask about pain quality, nighttime awakenings, nightmares, medication side effects, opioid exposure, sedative exposure, and whether pain or sleep is blocking prosthetic training. These questions belong beside wound healing and range-of-motion checks because untreated pain and insomnia can keep depression or PTSD symptoms active even when surgical recovery looks technically successful.
Integrated follow-up should therefore connect pain care, sleep assessment, and mental-health referral instead of treating them as separate problems. Treating pain and sleep well may reduce psychiatric burden even when formal psychotherapy is delayed.
A final practical detail is documentation. If screening is done but not connected to referral, follow-up, or rehabilitation planning, it becomes a checkbox. The care pathway should specify who reviews results, who contacts the patient, and how urgent risks are escalated.
The same pathway should include families when patients want them involved. Family members often notice avoidance, sleep loss, alcohol escalation, irritability, or hopelessness before those problems appear in a claims database.
Referral timing also matters. A same-day handoff during surgical or rehabilitation follow-up is more actionable than telling a distressed patient to find outpatient mental-health care alone.
Embedding support inside rehabilitation can also normalize help-seeking: mental health becomes part of recovery training, not a separate admission of weakness.
That framing can reduce avoidance during a high-risk adjustment period.
Questions About Mental Health After Upper-Extremity Amputation
Should everyone receive mental-health screening after major amputation?
Yes. Screening is low-risk, and the claims pattern supports checking early and again over the first year, especially for depression, anxiety, PTSD, sleep problems, and substance-related distress.
Does this prove major amputation causes depression?
It strongly supports association after matching, but claims data cannot prove causality. Trauma severity, pain, work disruption, medical complications, and social support likely interact with the amputation level.
Why include antidepressant and psychotherapy claims?
Diagnosis alone can miss whether the system responds. Treatment claims show that major amputations were associated with documented distress plus increased medication and therapy use.
References
- Analysis of mental health outcomes in major versus minor upper extremity amputations. Nedder et al. doi:10.1007/s00402-026-06319-y
- Upper-extremity amputation and mental health outcomes. PubMed search. PubMed search
- Upper-extremity injury, psychological distress, and functional outcomes. PubMed search. PubMed search
- Psychological interventions after upper-extremity injury. PubMed search. PubMed search