A 2026 real-world study involving 1,174 children with epilepsy proposed a levetiracetam therapeutic drug monitoring range of 2.82-24.37 mcg/mL, much lower than commonly cited adult-style ranges, but the same data also warned against treating a drug level as a stand-alone seizure-control predictor.
Research Highlights
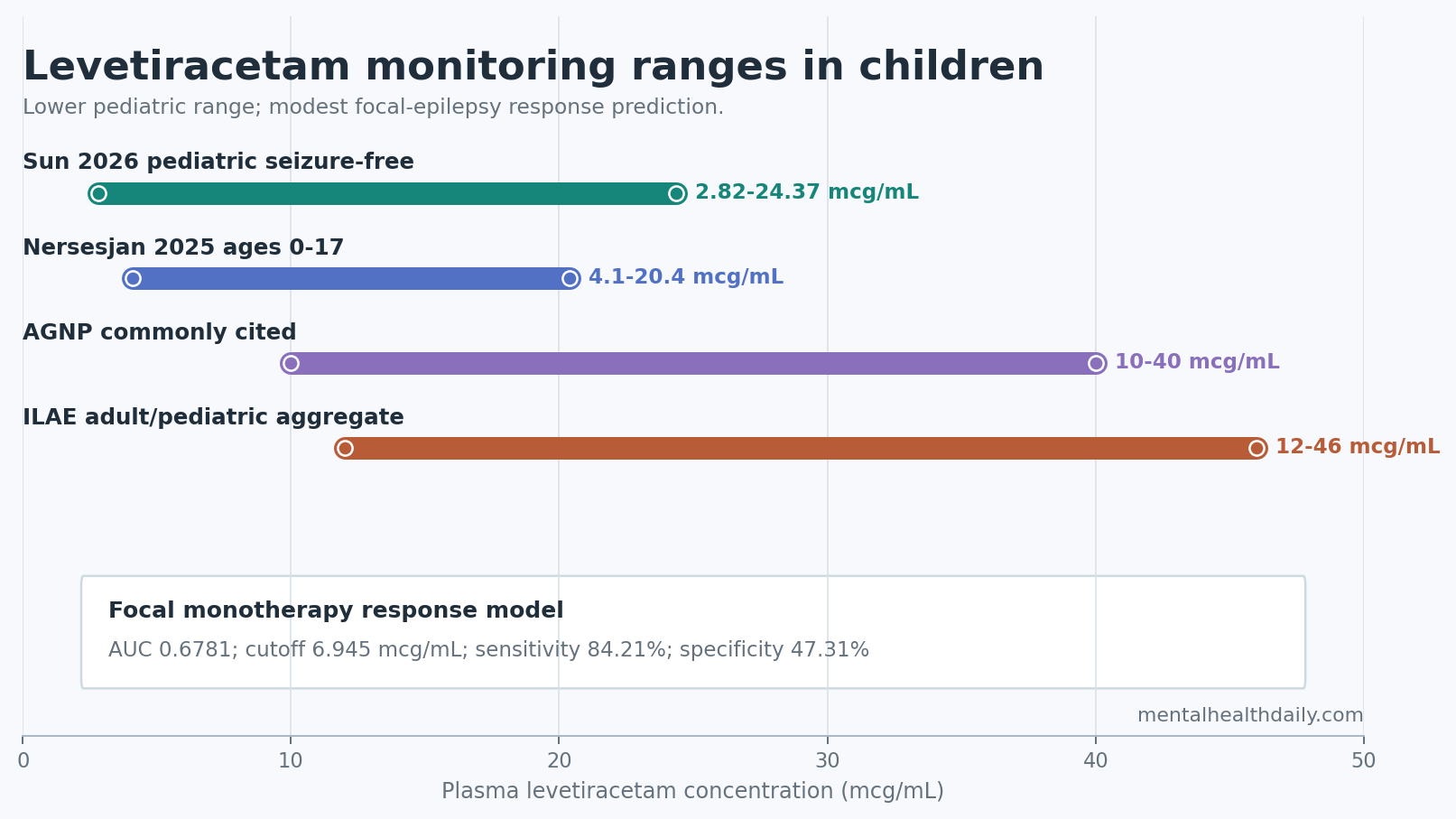
- Lower pediatric range: Sun et al. proposed an observational levetiracetam range of 2.82-24.37 mcg/mL from 401 seizure-free monotherapy patients and 1,119 samples.
- Adult targets look too high: the proposed upper boundary sits far below the ILAE-listed 12-46 mcg/mL range, supporting pediatric-specific interpretation rather than adult-range copy-paste.
- Response was not level-driven overall: concentration separated responders from non-responders only in focal epilepsy, with modest ROC performance of AUC 0.5832 overall and 0.6781 in focal monotherapy.
- Polytherapy marked harder epilepsy: 12-month response was 90.89% with monotherapy vs. 70.78% with polytherapy, and 2 or more added antiseizure medications carried OR 16.4067 for ineffective outcome.
- Safety monitoring cannot stop early: adverse events had median onset at 196.5 days, with 33.1% recorded after 360 days, so late behavioral and neurologic changes still belong in levetiracetam review.
Levetiracetam is a broad-spectrum antiseizure medication that binds synaptic vesicle protein 2A (SV2A), a vesicle protein involved in neurotransmitter release. It is widely used in children because it has few classic liver-enzyme interactions, comes in child-friendly formulations, and usually avoids the cognitive slowing associated with some older antiseizure drugs.
Therapeutic drug monitoring (TDM) means measuring blood drug concentration to help interpret dose, adherence, drug interactions, and toxicity risk. The hard part with levetiracetam is that a blood level often explains exposure better than outcome: 2 children can have similar concentrations and different seizure control, adverse effects, or comedications.
2.82-24.37 mcg/mL Was a Pediatric Observational Range, Not a Universal Target
Sun et al. analyzed 3,280 plasma levetiracetam concentrations from 1,174 children treated at Children’s Hospital of Nanjing Medical University from 2021 through 2023. The study used generalized additive models for location, scale, and shape (GAMLSS), a distributional modeling method that estimates how the spread of concentrations changes across patient strata rather than forcing one simple average.
The main range came from children who did well on levetiracetam monotherapy. Among 401 children who were seizure-free for 12 months on monotherapy, the modeled 2.5th to 97.5th percentile range was 2.82-24.37 mcg/mL. Among 560 children who had at least a 50% seizure-frequency reduction or seizure freedom, the parallel range was 3.11-24.29 mcg/mL.
Clinical read: this is a reference interval for observed successful exposure, not a proof that every child should be pushed into that window. The paper itself emphasized that the range is observational and should be interpreted alongside seizure control, adverse effects, age, weight, renal status, formulation, and comedications.
The range is still useful because older reference intervals were not pediatric-specific. The ILAE position paper listed 12-46 mcg/mL, while AGNP guidance moved between 10-40 and 20-40 mcg/mL before returning to 10-40 mcg/mL. A lower pediatric range fits adjacent pharmacokinetic work: children can clear levetiracetam faster than adults, and pediatric outcome studies have often found wide variability rather than one clean concentration-response threshold.
Focal Epilepsy Showed the Only Clear Concentration-Response Signal
Across the full cohort, plasma levetiracetam concentration did not clearly separate responders from non-responders. The p-value was 0.0856, which is not a statistically confirmed overall association. Subgroup analysis changed the picture: in focal epilepsy, concentrations differed between responders and non-responders (p = 0.0242), and the signal became stronger when the analysis was restricted to focal epilepsy treated with levetiracetam monotherapy (p = 0.0099).
Receiver operating characteristic analysis tests how well a marker separates 2 groups across possible cutoffs. In all focal epilepsy cases, levetiracetam concentration produced AUC 0.5832 (95% CI 0.5095-0.6569), which is only slightly better than chance. In focal monotherapy, AUC rose to 0.6781 (95% CI 0.5669-0.7894), with an optimal cutoff of 6.945 mcg/mL, sensitivity 84.21%, and specificity 47.31%.
That pattern argues for calibrated use. If a child with focal epilepsy has poor seizure control, a very low levetiracetam trough may be a useful clue. But low specificity means many children above or below the cutoff will not behave as predicted. TDM can support decision-making; it cannot replace a seizure diary, tolerability review, developmental context, or medication-history review.
Oxcarbazepine Lowered Exposure and Topiramate Raised It
The study’s mixed-effects model separated within-child repeated measurements from between-child differences. Age and body weight were both negatively associated with concentration-to-dose ratio, meaning older or heavier children tended to show lower concentration per mg/kg dose after adjustment.
Comedications also mattered:
- Oxcarbazepine: concentration-to-dose ratio was lower with oxcarbazepine (beta = −0.1824, p = 0.0012), consistent with the practical problem of enzyme-inducing antiseizure medication reducing exposure.
- Topiramate: concentration-to-dose ratio was higher with topiramate (beta = 0.2516, p = 0.0401), a directionally opposite interaction that should be interpreted cautiously but not ignored.
- Developmental delay: children with developmental delay showed a higher concentration-to-dose ratio (beta = 0.0674, p = 0.0481), suggesting that some neurodevelopmental subgroups may need closer level review.
Intraclass correlation coefficient (ICC) is the share of total variation attributable to stable differences between people. Sun et al. estimated ICC at 0.3846, so around 38% of levetiracetam concentration variability came from persistent individual differences rather than the measured dose or visit-level factors alone.
Monotherapy Response Was High, But Polytherapy Was a Severity Flag
At 12 months, 750 of 1,174 children were seizure-free, and 951 met the study’s response definition of seizure freedom or at least 50% seizure-frequency reduction. That produced an overall response rate of 81.01%.
Monotherapy looked much better than polytherapy: 90.89% response with levetiracetam alone vs. 70.78% response when levetiracetam was part of a combination regimen. The seizure-free rates showed the same pattern, 78.11% vs. 52.26%.
Those numbers should not be read as proof that adding drugs worsened outcomes. Children receiving combination therapy usually have more refractory epilepsy, prior medication failure, genetic or structural causes, and more complex baseline risk. The multivariable model made that severity signal visible: compared with no added antiseizure medication, 1 concomitant medication carried OR 3.2982 for ineffective outcome, while 2 or more carried OR 16.4067.
The same caution applies to comorbid ADHD. After propensity-score matching, children with epilepsy and ADHD had 92.7% response vs. 83.3% in children without ADHD (OR 0.39, 95% CI 0.18-0.78; p = 0.0149). That is an antiseizure-response signal, not proof that levetiracetam improves attention. Prior ADHD-epilepsy literature still includes concern about irritability, anger, and attention symptoms in some children.
Adverse Events Were Often Behavioral and Sometimes Late
Sun et al. recorded 248 adverse events. Nervous-system abnormalities were most common at 6.98%, followed by psychiatric abnormalities at 6.3% and skin or subcutaneous abnormalities at 4.26%.
Psychiatric adverse events included aggressiveness, emotional instability, and irritability. This matches the clinical reputation of levetiracetam: it is often cognitively clean compared with many antiseizure drugs, but behavioral side effects can be the limiting problem for some children and families.
Timing was not limited to the first few weeks. Median time to adverse-event onset was 196.5 days. Early onset still occurred, with 17.25% of patients affected within the first month, and gastrointestinal or systemic reactions followed an early-failure pattern. But 33.1% of adverse events were documented after 360 days.
Practical implication: behavioral changes after months on levetiracetam should not be dismissed just because the starting period was uneventful. A delayed school-behavior shift, irritability change, sleep disruption, or new family conflict can still justify checking dose, timing, trough level, comedications, and alternative causes.
The Evidence Supports Selective TDM, Not Blood-Level Medicine
The strongest use case for levetiracetam monitoring is not routine level chasing in every stable child. It is targeted interpretation when the clinical picture is unclear.
- Poor seizure control: a low trough can expose underdosing, nonadherence, rapid clearance, or interaction with oxcarbazepine-like comedication.
- Possible toxicity: a high or rising level can support dose review when drowsiness, dizziness, irritability, appetite loss, or other adverse effects appear.
- High-variability children: infants, rapidly growing children, children with developmental delay, children on polytherapy, and children with complex neurologic disease may not map cleanly onto adult reference intervals.
Evidence-strength note: this was a retrospective single-center study, not a prospective dosing trial. The proposed range is a useful pediatric calibration point, especially because it triangulates with selected-population TDM reviews and newer concentration-range work. It does not prove that changing a child’s dose to hit 2.82-24.37 mcg/mL will improve seizures or behavior.
Questions About Levetiracetam TDM in Children
Does a levetiracetam level below 10 mcg/mL mean the dose is too low?
Not automatically. Sun et al. found successful pediatric monotherapy exposures down to 2.82 mcg/mL in seizure-free children. A low level matters most when it appears alongside breakthrough seizures, suspected nonadherence, rapid growth, interacting medication, or a formulation change.
Should the 2.82-24.37 mcg/mL range replace older adult ranges?
It should not be treated as a universal replacement. It is a pediatric observational range from one large Chinese hospital cohort. It is more relevant to children than adult-derived intervals, but it still needs clinical context and prospective validation.
What result should change practice fastest?
Oxcarbazepine coadministration is the most actionable pharmacokinetic signal. If a child taking levetiracetam plus oxcarbazepine has poor seizure control, the lower concentration-to-dose ratio gives a concrete reason to check a trough level before assuming levetiracetam has failed.
References
- Sun XL, Zhang YY, Liu YJ, Guo HL, Li Y, Lu XP, et al. Defining the Therapeutic Range of Levetiracetam for Personalized Treatment in Pediatric Epilepsy: Insights from a Large Real-World Study. Drug Design, Development and Therapy. 2026;20:593587. doi:10.2147/DDDT.S593587
- Patsalos PN, Berry DJ, Bourgeois BF, Cloyd JC, Glauser TA, Johannessen SI, et al. Antiepileptic drugs–best practice guidelines for therapeutic drug monitoring: a position paper by the subcommission on therapeutic drug monitoring, ILAE Commission on Therapeutic Strategies. Epilepsia. 2008;49:1239-1276. doi:10.1111/j.1528-1167.2008.01561.x
- Sourbron J, Chan H, Wammes-van der Heijden EA, Klarenbeek P, Wijnen BFM, Schaper NC, et al. Review on the relevance of therapeutic drug monitoring of levetiracetam. Seizure. 2018;62:131-135. doi:10.1016/j.seizure.2018.09.004
- Jarvie D, Mahmoud SH. Therapeutic Drug Monitoring of Levetiracetam in Select Populations. Journal of Pharmacy and Pharmaceutical Sciences. 2018;21:149s-176s. doi:10.18433/jpps30081
- Yamamoto Y, Ohta A, Usui N, Neshige S, Nishida T, Matsuura M, et al. Clinical value of therapeutic drug monitoring for levetiracetam in pediatric patients with epilepsy. Brain and Development. 2023;45:285-292. doi:10.1016/j.braindev.2023.01.007
- Nersesjan M, Hoffmann-Lucke E, Greibe E, Johannessen Landmark C, Sabers A, Beniczky S. Evaluation of antiseizure medication concentration ranges in blood samples using an automated big data approach. Epilepsia. 2025;66:1888-1898. doi:10.1111/epi.18330