The depression-inflammation literature has firmly established that elevated inflammatory markers track with mood symptoms, but a 2026 study of 14,419 postpartum women from Xie et al. found the opposite pattern for postpartum anxiety: women with higher second-trimester platelet-neutrophil products and related immune-inflammation indices had substantially lower postpartum anxiety risk.1
Research Highlights
- Higher second-trimester PPN was associated with 79% lower odds of postpartum anxiety symptoms. Adjusted OR 0.21 (95% CI 0.10–0.45) for the platelet-neutrophil product after propensity-score matching and confounder adjustment.1
- SII and PIV showed similar protective associations. Systemic immune-inflammation index aOR 0.34 (95% CI 0.16–0.72); pan-immune-inflammation value aOR 0.44 (95% CI 0.26–0.75) in the second trimester.1
- The pattern held across all three time points. Second trimester, third trimester, and postpartum 5–8 weeks all showed the same direction. Consistent inverse associations between immune-inflammation indices and PPA symptoms with PFDR < 0.05.1
- Discrimination was modest for single biomarkers, robust for machine-learning ensembles. Single-marker PPN AUC 0.65–0.67 across time points. SVM-Radial model AUC 0.73–0.86.1
- Postpartum anxiety affects 7–28% of women. The Xie cohort drew from 14,419 mothers at a Nanjing women’s hospital, with 113 PPA cases (SAS ≥ 50) propensity-matched to 113 asymptomatic controls.1
Postpartum anxiety has been studied less than postpartum depression but produces measurable harm to maternal breastfeeding, mother-child bonding, infant mental development, and adolescent behavior outcomes.1
The inflammation-mood pathway has been mapped extensively in non-pregnancy populations, with elevated IL-6, CRP, and TNFα consistently linked to depression and anxiety symptoms.2
Pregnancy is its own immunological state. Maternal physiology shifts toward immune tolerance to support fetal development, and the markers that predict mood symptoms outside pregnancy may behave differently inside it.
Xie 2026: 14,419 Women, Three Time Points, Composite Inflammation Indices
The cohort drew from postpartum care visits at the Women’s Hospital of Nanjing Medical University.1
Eligibility required complete blood-test data at three time points: second trimester, third trimester, and postpartum 5–8 weeks. After exclusions for missing data, prior mental disorders, multiple pregnancies, and other criteria, 14,419 women were retained.
Anxiety was assessed at 5–8 weeks postpartum using the Self-Rating Anxiety Scale (SAS), with PPA defined as SAS ≥ 50. Propensity score matching paired 113 PPA cases 1:1 with 113 asymptomatic controls on age, BMI, parity, gestational age, preterm birth, gestational diabetes, and other potential confounders.
The inflammation panel relied on routine peripheral blood counts to derive composite indices:
- NLR (neutrophil-to-lymphocyte ratio) and LMR (lymphocyte-to-monocyte ratio): standard immune-balance metrics.
- PPN (platelet-neutrophil product): platelets multiplied by neutrophil count, capturing combined cellular activation.
- SII (systemic immune-inflammation index): platelets × neutrophils ÷ lymphocytes.
- SIRI (systemic inflammatory response index): neutrophils × monocytes ÷ lymphocytes.
- PIV (pan-immune-inflammation value): platelets × neutrophils × monocytes ÷ lymphocytes.
These composites were chosen because they integrate multiple cell types into a single number and are routinely available from standard blood tests — cheap, scalable, and already part of pregnancy care.
Multivariable logistic regression with FDR correction across markers and time points adjusted for demographic and obstetric covariates.
Higher Inflammation in Pregnancy Was Protective Against PPA Symptoms
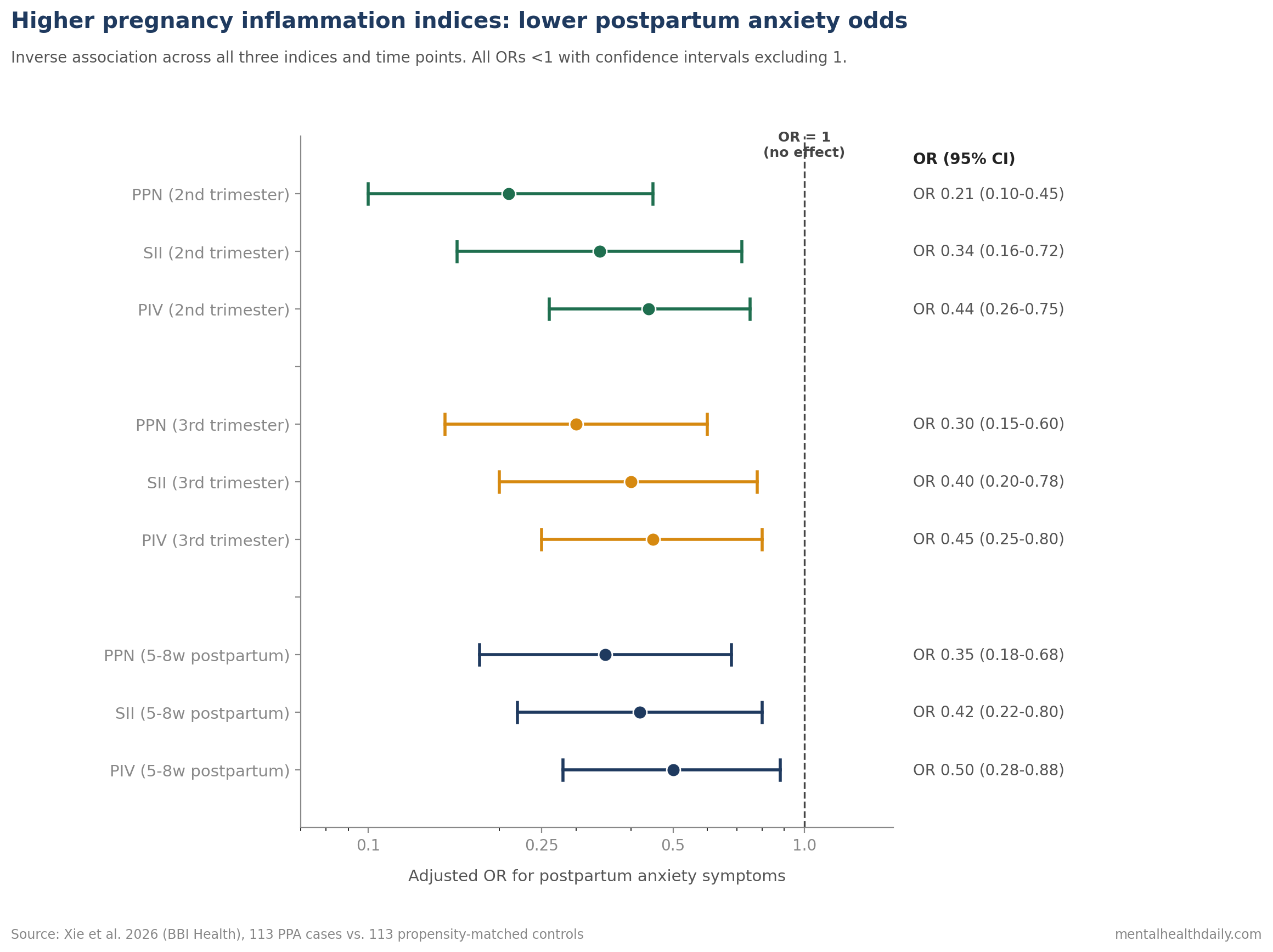
The second-trimester results are the most striking.1
PPN (platelet-neutrophil product): aOR 0.21 (95% CI 0.10–0.45). Women with higher second-trimester PPN had 79% lower odds of postpartum anxiety symptoms.
SII (systemic immune-inflammation index): aOR 0.34 (95% CI 0.16–0.72).
PIV (pan-immune-inflammation value): aOR 0.44 (95% CI 0.26–0.75).
The same direction held in the third trimester and the 5–8 week postpartum period, with PFDR-corrected p-values remaining below 0.05.
Discrimination was modest for single markers (PPN AUC 0.65–0.67), reflecting that inflammation explains only part of PPA risk. The SVM-Radial machine-learning model integrating multiple markers achieved AUC 0.73–0.86 across time points.
Pregnancy Immune Tolerance Makes the Inverse Anxiety Link Plausible
The depression-inflammation literature in non-pregnancy populations consistently shows the opposite direction: elevated IL-6, CRP, and TNFα track with worse mood symptoms.2
So why would pregnancy show inflammation as protective?
Pregnancy is a controlled immunological state. Maternal physiology actively shifts the immune balance to tolerate the genetically half-foreign fetus. Healthy pregnancy is associated with measurable elevation of certain immune markers and shifts in cell ratios that look pro-inflammatory by non-pregnancy standards but reflect normal adaptive physiology.3
Two reasonable mechanistic interpretations of the Xie findings emerge:
Adaptive immune competence as a marker of well-regulated pregnancy. Women with healthy pregnancy-specific immune adaptation have higher composite inflammation indices, robust placental function, and lower stress-axis dysregulation — all of which protect against postpartum anxiety.
Lower-than-expected inflammation as a marker of dysregulation. The inverse pattern may flag an immune-suppressive phenotype that correlates with stress-axis dysregulation, anxious temperament, or other PPA risk factors. Lower platelet-neutrophil products in pregnancy could indicate physiological subtle blunting of normal pregnancy-immune adaptation.
Either interpretation is consistent with the Xie data; the cross-sectional design does not separate them.
Do Not Treat Inflammation Biomarkers as a Postpartum Anxiety Screen Yet
- Routine pregnancy blood counts already contain potential PPA risk information. Composite indices like PPN, SII, and PIV can be calculated from existing complete blood count data without additional testing.
- Single-marker discrimination is modest. AUC 0.65–0.67 for PPN means the marker is not a clinical screener on its own. Multivariable models combining inflammation indices with demographic and obstetric risk factors achieved better performance.
- Don’t generalize from depression-inflammation findings. The inverse pattern in pregnancy means that the standard “elevated inflammation = mood symptoms” framework does not apply directly to PPA. Pregnancy-specific immunology is different.
- Standard PPA screening still matters more than biomarkers. Validated postpartum anxiety screening (GAD-7, PASS, or SAS as in this study) at the postpartum visit remains first-line. Inflammation indices may eventually augment screening; they do not replace it.
- Replication in non-Chinese cohorts is the next step. The Nanjing population may have specific dietary, demographic, or healthcare-access patterns that influence the result. Generalizability to Western populations is untested.
Single-Hospital Case-Control Data Cannot Prove Protection
The case-control sample is small. 113 PPA cases and 113 matched controls were the analytic sample after propensity-score matching. The 14,419 figure refers to the eligible cohort from which cases were drawn; the effect-size estimates rest on the matched 226-woman analysis.
The single-time-point assessment misses dynamics. Women were assessed for anxiety at one postpartum window (5–8 weeks). Anxiety symptoms that emerge later or fluctuate may not be captured.
The SAS is not the gold standard for postpartum anxiety. Validated postpartum-specific instruments (Postpartum Specific Anxiety Scale [PSAS], for example) might produce different prevalence and association patterns. The SAS ≥ 50 cutoff is conservative.
Causality is not established. Whether immune dysregulation contributes to PPA risk, or whether anxious temperament influences immune-cell counts, or whether both share upstream causes (sleep, stress, social support) is not separable in this design.
Other inflammatory markers (IL-6, CRP, TNFα) were not measured. The study used composite indices derived from blood-cell counts. Whether soluble cytokines show the same inverse pattern, or the conventional positive pattern, is untested here.
Questions About Pregnancy Inflammation and Postpartum Anxiety
Does this mean inflammation protects against postpartum anxiety?
The data show that women with higher composite inflammation indices in pregnancy had lower postpartum anxiety risk after adjustment for confounders.1
The interpretation is more nuanced than “inflammation is protective.” The pattern more likely reflects healthy pregnancy-specific immune adaptation, with low values flagging a subtle immune dysregulation that tracks with anxiety vulnerability.
Why is this opposite to the depression-inflammation pattern?
Pregnancy is an immunologically distinct state. Maternal physiology shifts toward tolerance of the fetus, and certain cell-count ratios shift in directions that would look pro-inflammatory outside pregnancy but reflect normal adaptive change inside it.3
The depression-inflammation findings in non-pregnant adults may not translate directly to the postpartum context.
Can my obstetrician test for this risk?
Composite indices like PPN, SII, and PIV can be calculated from routine complete blood counts (CBC) that pregnancy care typically already includes.1
The clinical use of these markers as PPA risk-stratification tools is not yet established. Single-marker AUC 0.65–0.67 is too modest for screening on its own. Replication and validation in Western cohorts and in larger samples are needed.
What’s the best way to identify postpartum anxiety risk?
Validated screening at postpartum visits using instruments like the GAD-7 or PASS remains the first line.4
Established risk factors include personal or family history of anxiety or depression, prior PPA, traumatic delivery, NICU admission of the infant, lack of social support, and ongoing stressors. Inflammation markers may eventually augment but not replace clinical assessment.
What treatments work for postpartum anxiety?
CBT and interpersonal therapy have the strongest evidence base for PPA. SSRIs are commonly prescribed and have established safety in lactation for sertraline and other lactation-compatible agents. Behavioral interventions including peer support and structured maternal-care groups also help.4
Treatment choice depends on severity, breastfeeding status, prior medication response, and patient preference.
References
- Association of inflammatory biomarkers during pregnancy and the postpartum period with the risk of postpartum anxiety symptoms. Xie K et al. Brain, Behavior, & Immunity – Health. 2026;53:101214. doi:10.1016/j.bbih.2026.101214
- A meta-analysis of cytokines in major depression. Dowlati Y et al. Biological Psychiatry. 2010;67(5):446-457. doi:10.1016/j.biopsych.2009.09.033
- Immunological adaptation in pregnancy. Mor G & Cardenas I. American Journal of Reproductive Immunology. 2010;63(6):425-433. doi:10.1111/j.1600-0897.2010.00836.x
- Postpartum-specific anxiety as a predictor of infant-feeding outcomes and perceptions of infant-feeding behaviours: findings from the Born in Bradford cohort study. Fallon V et al. Maternal & Child Nutrition. 2018;14(2):e12491. doi:10.1111/mcn.12491
- Inflammation: depression fans the flames and feasts on the heat. Miller AH & Raison CL. American Journal of Psychiatry. 2015;172(11):1075-1091. doi:10.1176/appi.ajp.2015.15020152