A 2026 systematic review found 15 clinical reports of deep brain stimulation for cerebellar ataxia, covering only 27 human patients across heterogeneous targets, causes, and outcome measures.
Research Highlights
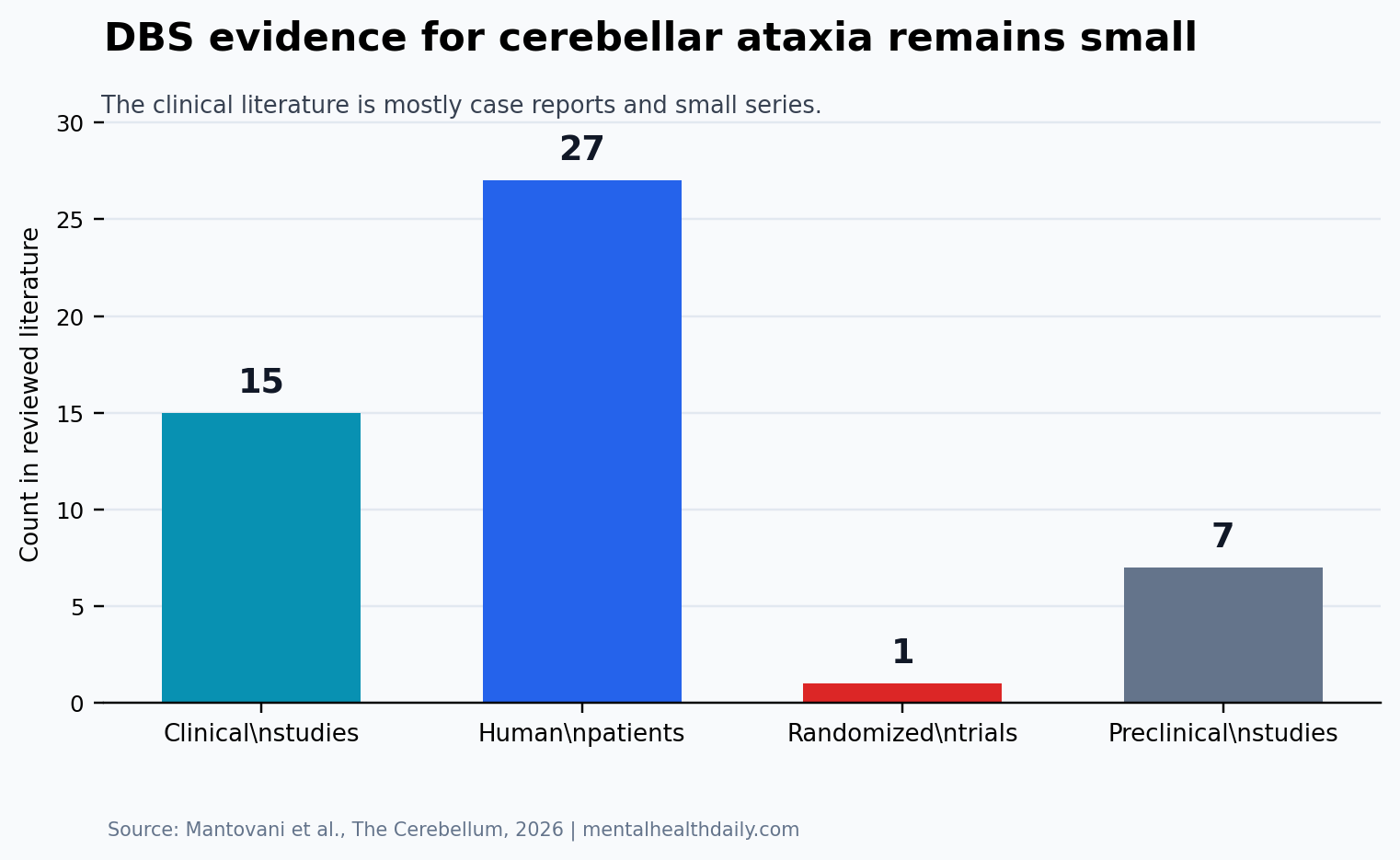
- The human evidence base was tiny: the review found 27 patients across 15 clinical studies, including 10 case reports, 4 case series, and 1 randomized trial.
- The dentate nucleus was the main target: stimulation of this deep cerebellar output hub showed the most coherent signal, including a 5-patient randomized crossover trial with a 21.02% mean SARA decrease.
- Thalamic stimulation was more tremor-weighted: among 7 reported stimulation targets, ventral intermediate and ventral oral thalamic targets helped some tremor-dominant presentations, but gait and speech could worsen in vulnerable patients.
- The evidence is still exploratory: 27 patients, scattered diagnoses, short follow-up, and probable publication bias prevent a durable estimate of benefit.
DBS mechanism: deep brain stimulation uses implanted electrodes to deliver adjustable electrical pulses to a specific brain target. In Parkinson’s disease and essential tremor, DBS can reduce abnormal motor-circuit firing.
Ataxia challenge: in cerebellar ataxia, the logic is harder because the problem is often degeneration or injury inside the cerebellum and its output pathways, not a single overactive circuit that can simply be quieted.
Cerebellar ataxia means impaired coordination from cerebellar dysfunction. Patients can have unstable gait, slurred speech, poor limb coordination, tremor, abnormal eye movements, and difficulty with precise movements. The Scale for the Assessment and Rating of Ataxia, or SARA, is a common clinician-rated severity scale; lower scores mean less ataxia.
Only 27 Human Patients Have Been Reported Across 15 DBS Studies
Mantovani et al. searched MEDLINE/PubMed and Scopus for DBS studies in cerebellar ataxia. The search returned 567 records: 202 from PubMed and 365 from Scopus. After 156 duplicates were removed, 411 titles and abstracts were screened. The researchers assessed 26 full-text articles and included 15 clinical studies plus 7 preclinical animal studies.
Study Snapshot
- Review type: systematic review of DBS for cerebellar ataxia.
- Clinical evidence: 15 human studies involving 27 patients.
- Study designs: 10 case reports, 4 case series, and 1 randomized trial.
- Preclinical evidence: 7 animal studies of DBS or cerebellar-circuit stimulation.
- Main limitation: the review could not run a meta-analysis because diagnoses, targets, stimulation settings, and outcomes differed too much.
The diagnoses were scattered across spinocerebellar ataxia types, Friedreich ataxia, mitochondrial epilepsy with ragged-red fibers, fragile X-associated tremor/ataxia syndrome, post-stroke ataxia, traumatic ataxia, and other acquired or hereditary presentations. That variety is clinically honest, but it makes the evidence hard to compress into a single expected benefit.
Seven stimulation targets appeared in the clinical literature. The list included the dentate nucleus, thalamic targets such as the ventral intermediate nucleus and ventral oral nucleus, the globus pallidus internus, the subthalamic nucleus, and posterior subthalamic area or zona incerta regions. The dentate nucleus was the most biologically direct target because it is a major output node from the cerebellum to motor-planning circuits.
Dentate Nucleus DBS Had the Most Coherent Ataxia Signal
Target logic: the dentate nucleus is a deep cerebellar structure that helps route cerebellar output toward the thalamus and motor cortex. Stimulating it is meant to modulate cerebellar outflow rather than only suppress tremor downstream.
Randomized-trial signal: in the randomized crossover trial by Cury et al., 5 patients received dentate nucleus stimulation. SARA scores decreased by a mean of 21.02%, but that change did not reach statistical significance, with p = 0.223. Tremor scores on the Fahn-Tolosa-Marin Tremor Rating Scale decreased by 23.74%, with p = 0.039. Patient Global Impression of Change improved, with a score of 6 and p = 0.038.
Endpoint split: the tremor and patient-global measures separated more clearly than the ataxia scale. A 5-person randomized trial can reveal a signal worth pursuing, but it cannot define patient selection, durability, or surgical risk for a broad cerebellar ataxia population.
Case-series signal: Diniz et al. reported larger descriptive gains after dentate nucleus DBS, including a 27.8% decrease in SARA scores and a 47.6% decrease in tremor scores. Other case reports described SARA decreases ranging from roughly 16% to 45% in selected patients. Those numbers look clinically interesting, but case reports overrepresent patients who received an unusual intervention and then had a result worth publishing.
Thalamic DBS May Help Tremor More Than Gait or Speech
Thalamic stimulation has a different rationale. The ventral intermediate nucleus is a standard target for medication-refractory tremor because it sits in a motor relay pathway. In ataxia patients whose most disabling symptom is tremor, thalamic DBS can reduce oscillatory motor output without directly repairing cerebellar degeneration.
The review reported improvement in some tremor-dominant cases, but thalamic stimulation also carried a practical warning: gait and speech can worsen when stimulation spreads into circuits that already compensate poorly. For cerebellar ataxia, the tradeoff directly affects walking, swallowing, speech clarity, and fall risk, so tremor improvement alone is an incomplete benefit measure.
Target choice: dentate nucleus stimulation is the more direct ataxia-circuit strategy, while thalamic stimulation is closer to a tremor-control strategy. A patient with severe action tremor and relatively preserved gait may face a different risk-benefit calculation than a patient with disabling gait ataxia and only mild tremor.
Phenotype choice: cerebellar ataxia is not one disease. Hereditary spinocerebellar ataxia, post-stroke ataxia, mitochondrial disease, and fragile X-associated tremor/ataxia syndrome can share coordination problems while differing in progression rate, affected pathways, and response to stimulation.
Noninvasive Cerebellar Stimulation Is Safer but Shallower
Surface stimulation: transcranial direct current stimulation and repetitive transcranial magnetic stimulation deliver weak electrical current or magnetic pulses through the scalp to modulate cortical or cerebellar excitability. They are lower risk than DBS because no electrodes are implanted, but they cannot stimulate deep cerebellar nuclei with the precision of a surgical lead.
Expected effect size: recent meta-analytic work on noninvasive stimulation in degenerative cerebellar ataxia reported short-term improvements of roughly 1.5 to 2 points on ataxia scales in some pooled analyses. The effects looked more plausible with repeated sessions and milder disease. Those results support cerebellar neuromodulation as a concept, while also showing why surface stimulation and implanted dentate nucleus stimulation answer different clinical questions.
Risk tradeoff: DBS carries surgical risks including hemorrhage, infection, hardware complications, stimulation side effects, and the long-term burden of programming visits. Noninvasive stimulation has a better safety profile but may produce smaller or less durable effects. The decision depends on deep target access, expected symptom domain, durability, and patient-specific risk.
Evidence-Strength Note for DBS in Cerebellar Ataxia
What the review can support: the 2026 systematic review can identify promising targets, summarize reported effect sizes, and expose clinical patterns that deserve better trials.
What the review cannot support: DBS is not an established treatment for cerebellar ataxia. The human evidence includes only 27 patients, the clinical literature is dominated by case reports and case series, and publication bias is likely because unsuccessful surgical cases are less likely to appear as detailed reports.
Durability gap: a short-term SARA decrease does not prove that stimulation slows disease progression, preserves independence, reduces falls, improves swallowing, or maintains benefit across years. Future trials need standardized ataxia scales, gait and speech endpoints, adverse-event reporting, stimulation programming details, and prespecified patient-selection rules.
What DBS for Cerebellar Ataxia Can Support Right Now
- Research referral in selected severe cases: DBS may be reasonable to discuss in specialized centers for patients with disabling ataxia or tremor who have no adequate standard treatment and a phenotype matching prior reports.
- Dentate nucleus trials: the most coherent ataxia-directed pathway is stimulation of the dentate nucleus, especially when studies measure SARA, gait, tremor, speech, and quality-of-life outcomes together.
- Tremor-specific thalamic DBS caution: thalamic targets can reduce tremor but may worsen gait or speech, so tremor improvement alone is an incomplete success metric in cerebellar ataxia.
- No routine-care shortcut: the current literature does not justify presenting DBS as a standard treatment for the broad cerebellar ataxia population.
Mantovani et al. made the DBS literature look less mysterious and more fragile. Dentate nucleus stimulation may be the target to watch, but 27 human patients across 15 clinical studies cannot carry a routine-treatment claim.
Trial priority: the field needs multi-center protocols that separate tremor relief from gait, speech, swallowing, falls, and independence outcomes.
Questions About DBS for Cerebellar Ataxia
Is DBS approved as a standard treatment for cerebellar ataxia?
No. DBS for cerebellar ataxia remains experimental and should be considered only in specialized contexts or research settings.
Which DBS target looks most promising for ataxia itself?
The dentate nucleus looks most relevant for ataxia because it is a major cerebellar output hub. The evidence is still based on very small human samples.
Can thalamic DBS help patients with cerebellar ataxia?
Thalamic DBS may help tremor-dominant symptoms in some patients. It can also worsen gait or speech, so the target is not interchangeable with dentate nucleus stimulation.
How is DBS different from noninvasive cerebellar stimulation?
DBS uses implanted electrodes to reach deep targets with programmable stimulation. Noninvasive methods stimulate through the scalp, which reduces surgical risk but limits depth and targeting precision.
References
- Mantovani A, Moscano F, Gan J, et al. Deep brain stimulation for cerebellar ataxia: emerging potential and future directions. The Cerebellum. 2026. https://doi.org/10.1007/s12311-026-01999-z
- Teixeira MJ, Cury RG, Galhardoni R, et al. Deep brain stimulation of the dentate nucleus improves cerebellar ataxia after cerebellar stroke. Neurology. 2015;85(24):2075–2076. https://doi.org/10.1212/wnl.0000000000002204
- Cury RG, Fraix V, Castrioto A, et al. Safety and outcomes of dentate nucleus deep brain stimulation for cerebellar ataxia. The Cerebellum. 2022;21(5):861–865. https://doi.org/10.1007/s12311-021-01326-8
- Kim WS, Jung SH, Oh MK, Min YS, Lim JY, Paik NJ. Effect of repetitive transcranial magnetic stimulation over the cerebellum on patients with ataxia: a systematic review and meta-analysis. Brain Sciences. 2022;12(5):648. https://doi.org/10.3390/brainsci12050648
- Du J, Yang F, Hu J, et al. Effects of non-invasive brain stimulation for degenerative cerebellar ataxia: a systematic review and meta-analysis. Movement Disorders Clinical Practice. 2024;11(8):949–961. https://doi.org/10.1002/mdc3.14205