
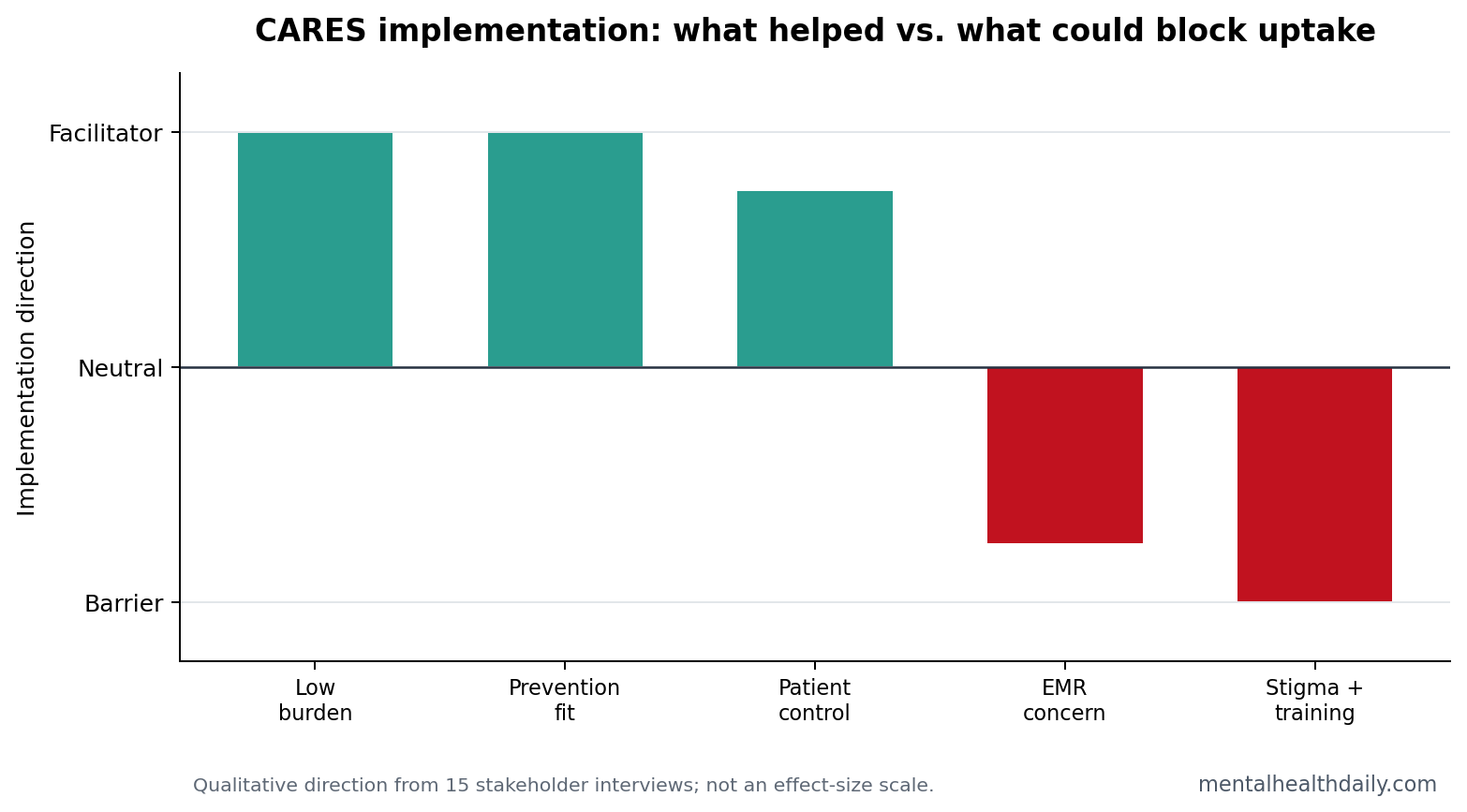
A 2026 medRxiv preprint interviewed 15 health-system stakeholders about CARES, a freestanding addiction-risk screening platform, and found a clear implementation split: people wanted better substance-use prevention tools than current clinic screening, but provider burden, stigma, knowledge gaps, and medical-record liability could block uptake.1
Research Highlights
- Stakeholders saw a screening gap: all 15 interviewees held leadership roles, 75% were patient-facing, and many described current substance-use screening as inconsistent or too focused on already visible problems.1
- Provider burden was the main threat: interviewees wanted a tool that required minimal training, little appointment time, and low clinician administration burden.1
- Freestanding design looked safer: a majority preferred keeping CARES separate from the medical record because integration could increase liability, stigma concerns, and workflow friction.1
- Younger populations were the clearest fit: stakeholders especially saw utility in adolescents and young adults, where prevention can start before substance-use disorder is established.1
- Evidence is still implementation-stage: this was a 15-person needs assessment, not proof that CARES changes substance use, treatment entry, or long-term addiction outcomes.1
Substance use disorder (SUD) means a pattern of alcohol or drug use that causes clinically significant impairment, loss of control, risky use, craving, or continued use despite harm. Clinical systems are supposed to screen for it, but the practical reality is uneven: time, stigma, uncertainty about follow-up, and provider discomfort often decide whether screening happens.
CARES stands for Comprehensive Addiction Risk Evaluation System. In this study, CARES was described as a freestanding platform that gives personalized information about genetic and behavioral/environmental risk for substance-use problems, then connects the person to resources matched to the risk profile.1
The platform is trying to solve a different problem than classic screening tools. AUDIT, TAPS, and other structured tools ask whether current use is risky or already harmful. CARES tries to move upstream by combining risk information with prevention resources before a person meets full SUD criteria.
That upstream approach creates its own implementation burden. Prevention tools have to explain risk without fatalism, avoid stigmatizing adolescents, and give clinicians a clear next step when a patient screens high risk but does not yet need specialty addiction treatment.
15 Stakeholders Wanted Prevention Before SUD Is Obvious
Dash et al. interviewed 15 stakeholders in Rutgers-affiliated health systems using the Consolidated Framework for Implementation Research, a framework for mapping what helps or blocks a clinical tool from becoming routine practice.1 The sample was implementation-heavy: 100% held leadership roles, 75% had patient-facing roles, 53% had administrative roles, and 40% had SUD-focused positions.
The core appeal was prevention. Existing screening often asks about current use, current impairment, or already visible disorder. CARES aimed at a different moment: identify elevated risk before substance-use problems are entrenched and offer tailored resources without making the primary care visit carry the whole intervention.
The stakeholder mix also affects interpretation. These were not 15 randomly selected clinicians. The sample included leaders, administrators, patient-facing clinicians, and people with or without SUD-focused roles. That is exactly the group that can say whether a tool fits a health system, but it is not the same as asking patients whether they trust risk feedback.
Workflow Burden Can Defeat a Good Screening Tool
Stakeholders were not hostile to screening. The problem was that a new tool becomes another task unless it reduces work somewhere else. The same concern appears in McNeely et al.’s primary-care study, where patients, providers, and staff described workflow, stigma, confidentiality, and treatment-referral uncertainty as barriers to substance-use screening.2
The practical threshold is simple: a screening tool has to be easier than avoidance. If clinicians need extensive training, extra charting, complex interpretation, or a long discussion they do not feel equipped to handle, screening will stay inconsistent even when everyone agrees it is important.
That is why the study’s freestanding design is more than a technical detail. If CARES can be introduced by a clinician but completed by the patient with minimal clinician administration, the provider becomes a doorway rather than the whole intervention. That design directly targets the burden problem interviewees described.
Freestanding CARES May Reduce Liability and Stigma Concerns
One notable finding was the preference for keeping CARES separate from the electronic medical record. That might sound counterintuitive because integration usually helps clinical tools become routine. Here, stakeholders worried that putting addiction-risk information into the medical record could create new burden, liability, stigma, or privacy concerns.1
Genetic risk feedback means using inherited variants to estimate vulnerability, not diagnosing a disorder or predicting destiny. In addiction prevention, that distinction is crucial. A person can hear “you are high risk” as useful prevention information, but also as a label, a warning that could be misused, or a reason to avoid care if privacy is unclear.
The medical-record question is especially sensitive for adolescents. A parent, school, insurer, future clinician, or legal system may interpret addiction-risk information differently from the patient. Keeping the platform freestanding may protect privacy during early implementation, but it also creates a handoff problem: the patient still needs a way to bring results into care when help is wanted.
Adolescents and Young Adults Were the Clearest Prevention Target
Stakeholders repeatedly viewed younger populations as the natural fit. The logic is not that older adults do not need screening. It is that adolescent and young-adult risk feedback can land before years of heavy exposure, social reinforcement, tolerance, withdrawal, or legal and occupational consequences accumulate.
That emphasis lines up with risk-factor research. Childhood externalizing and internalizing problems predict earlier substance use in longitudinal work, and impulsivity/urgency models connect affect regulation with later substance-use risk.5,6 CARES tries to turn that risk science into a patient-facing prevention pathway.
Adolescent implementation: risk feedback has to be paired with resources that do not feel like punishment. Practical options include family conversation prompts, brief counseling pathways, harm-reduction education, mental-health resources, and follow-up choices that let the patient decide how much information to share with a provider.
Risk Feedback Needs a Clear Next Prevention Step
A prevention platform can fail even when its risk model is technically sound. Patients need plain-language interpretation, boundaries around the result, and an action available today. A high-risk CARES result should land as a prompt for earlier support: safer-use education, family conversation, mental-health care when distress is driving risk, or a low-friction referral when substance use has already started.
That distinction is especially important because the study centered implementation stakeholders, not patient outcomes. Clinicians and administrators can identify workflow hazards, but patients decide whether the feedback feels useful, frightening, stigmatizing, or worth acting on. A tool aimed at adolescents and young adults has to preserve trust while still being direct about risk.
Practical implementation tests: the next CARES studies should measure more than completion. Useful endpoints include whether patients understood the result, whether they clicked or used recommended resources, whether they discussed the result with a clinician or family member, and whether high-risk users were connected to prevention support without unnecessary chart labeling.
Workflow test: a freestanding platform reduces chart burden only if staff can introduce it quickly, patients can complete it without hand-holding, and clinicians receive a simple summary when follow-up is needed. If the output creates a vague alert with no referral pathway, the platform shifts burden rather than solving it.
The Tool Still Needs Outcome Evidence
Evidence-strength note: this study was a qualitative preprint and was not certified by peer review at the time captured in the PDF. It measured stakeholder views in one academic-linked health system. It did not test whether CARES changes substance use, prevents SUD, improves treatment entry, or reduces overdose risk.
That does not make the study useless. Implementation failures usually happen before an outcome trial can matter. If clinicians see a tool as burdensome, stigmatizing, legally awkward, or poorly matched to clinic flow, the intervention never reaches enough patients to test its clinical promise.
Dash et al. reported several changes made after stakeholder feedback: a Spanish-language version, translated resources, handouts connecting patients to substance-use and mental-health resources, conversation starters for family or provider discussion, and access to a genetic counselor. Those modifications show the right implementation sequence: listen to workflow and equity concerns before testing whether the tool changes behavior.
That modification list also makes the platform easier to evaluate. If patients decline CARES, researchers can ask whether the barrier was language, privacy, risk interpretation, resource quality, or clinician introduction rather than treating nonuse as generic disinterest.
Evidence gap: the platform still needs patient-level completion, satisfaction, behavior-change, and follow-up data. Stakeholder acceptability can open the door, but prevention credibility requires showing that high-risk users understand the feedback, use resources, and do not experience avoidable stigma or anxiety.
Questions About CARES Addiction-Risk Screening
Does CARES diagnose addiction?
No. CARES is described as a risk-screening and feedback platform. It is meant to identify elevated vulnerability and connect people to resources, not to diagnose SUD by itself.
Why not put CARES directly into the medical record?
Stakeholders worried that integration could increase provider burden, legal responsibility, stigma, and patient privacy concerns. A freestanding platform may be easier to introduce while the outcome evidence is still developing.
What evidence would make CARES clinically stronger?
CARES needs patient-level pilot data: completion rates, perceived usefulness, resource use, family/provider discussion, behavior change, and whether high-risk users actually receive prevention support. A prevention tool earns clinical trust when patients understand the feedback and can act on it without being pushed into stigma, surveillance, or a dead-end referral.
References
- Dash GF, et al. Stakeholder views on implementing a novel substance use risk screening tool in healthcare. medRxiv. 2026. doi:10.64898/2026.04.14.26350880
- McNeely J, et al. Barriers and facilitators affecting the implementation of substance use screening in primary care clinics: a qualitative study of patients, providers, and staff. Addiction Science & Clinical Practice. 2018. https://doi.org/10.1186/s13722-018-0110-8
- Wu LT, et al. Design of the NIDA clinical trials network validation study of tobacco, alcohol, prescription medications, and substance use/misuse (TAPS) tool. Contemporary Clinical Trials. 2016. https://doi.org/10.1016/j.cct.2016.07.013
- Reilly J, et al. Substance use disorder screening and brief intervention in routine clinical practice in specialist adult mental health services: A systematic review. Australian & New Zealand Journal of Psychiatry. 2023. https://doi.org/10.1177/00048674221148394
- King SM, et al. Childhood externalizing and internalizing psychopathology in the prediction of early substance use. Addiction. 2004. https://doi.org/10.1111/j.1360-0443.2004.00893.x
- Smith GT, Cyders MA. Integrating affect and impulsivity: The role of positive and negative urgency in substance use risk. Drug and Alcohol Dependence. 2016. https://doi.org/10.1016/j.drugalcdep.2015.08.038