Community forensic mental health services are supposed to bridge secure hospitals, prisons, community psychiatry, and risk management. A 2026 mapping study of England found that these services still vary substantially in structure, referral routes, psychological treatments, and the way they handle restricted patients.1
Research Highlights
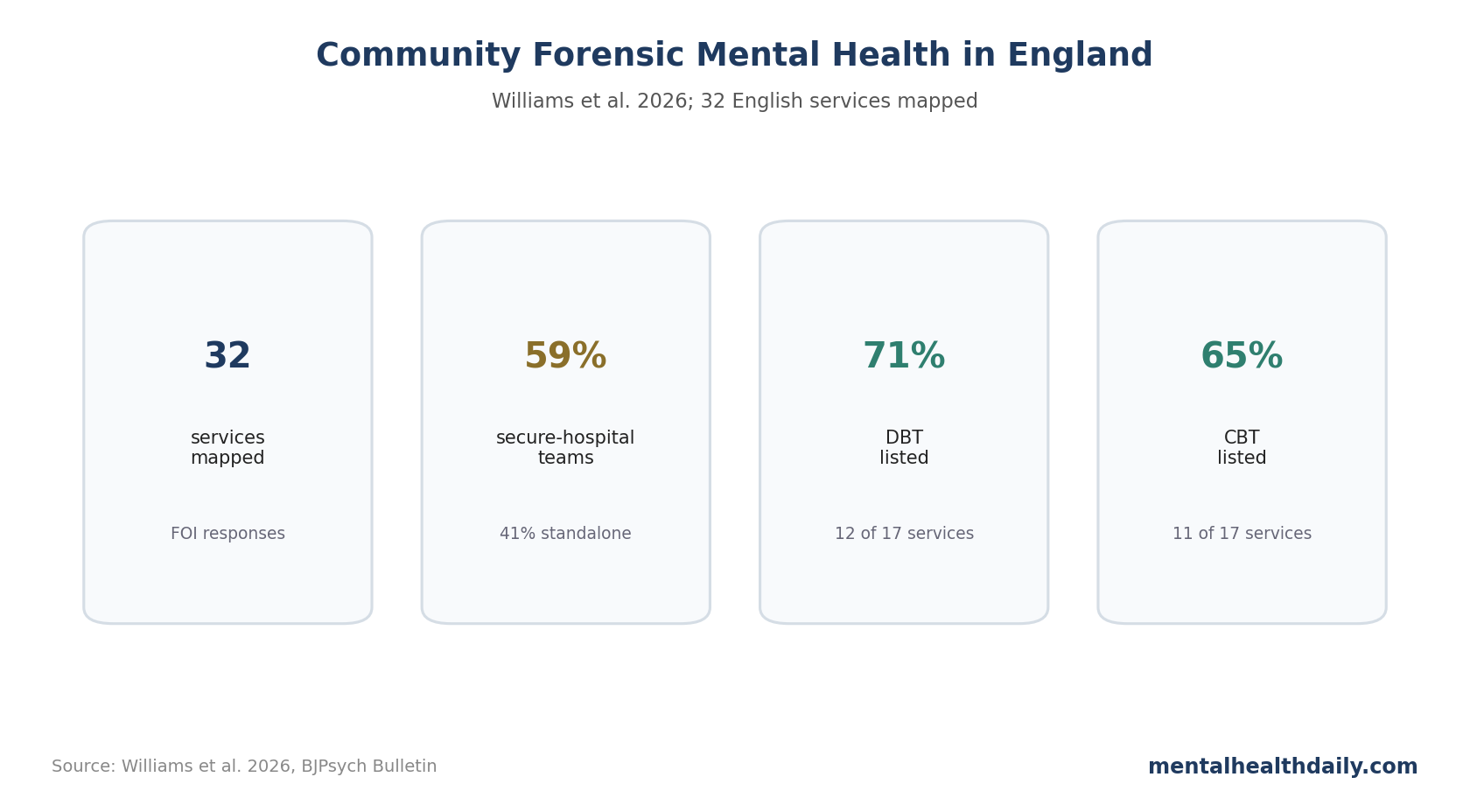
- 32 services were mapped: Freedom of Information responses from NHS Trusts identified service names, structures, referral routes, staffing patterns, psychological interventions, and operating arrangements.1
- Secure-hospital extension was common: 59% of services were linked to secure hospital-based teams, while 41% operated as standalone teams working in parallel with general services.1
- Referral access was uneven: some services accepted referrals from secure hospitals, general adult services, prisons, and community teams, while others excluded key routes that often matter for serious mental illness and violence-risk care.1
- Therapy provision existed but varied: among 17 services reporting therapy details, dialectical behavior therapy was listed by 71%, cognitive behavioral therapy by 65%, and schema therapy by 47%.1
- The clinical problem is identity: the 32-service map points to a model with shared aims but no fully standardized operating core across England.
The sharpest distinction is how community forensic mental health services function: secure-hospital outreach arm, standalone community team, or hybrid service with local variations. That functional difference determines who owns transitions, crisis planning, and specialist advice.
If referrers cannot predict who is accepted, what help is offered, and how risk is shared, patients can fall between secure care, prison release, general adult psychiatry, and crisis systems.
FOI Requests Captured 32 English CFMHS Teams
Williams et al. sent Freedom of Information requests to 50 NHS Trusts and received usable information from 80% of them. The analysis focused on community forensic mental health services (CFMHS), which support people whose mental disorder is tied to serious risk of harm, often around discharge from secure care or contact with criminal-justice settings.1
- Service structure: 59% were secure hospital-based teams; 41% were standalone teams working parallel with general services.
- Service names: labels included community forensic team, specialist CFMHS, forensic outreach, outreach/liaison, intensive recovery support, and integrated psychological pathway.
- Operating hours: many worked standard weekday hours, while out-of-hours arrangements differed where reported.
- Referral management: most used referral forms, but acceptance criteria and source settings differed.
The mapping is a service-organization study, not an outcome trial. It cannot identify which model reduces violence, hospitalization, reoffending, or patient distress, but it shows that England’s CFMHS landscape is too heterogeneous to evaluate cleanly until the service product is defined.
Evidence strength: the study is strongest as a national service map. It gives planners a concrete denominator for community forensic mental health provision, but outcome claims still require linked follow-up data that can separate service structure from case mix, local commissioning, staff exposure, and baseline risk.
Secure-Hospital Linkage Was Common but Not Uniform
The older binary of integrated vs. parallel services misses how current services operate. The 2026 study found that secure-hospital linkage was a major organizing feature, but not a complete explanation of service function.
Some teams primarily supported transition out of secure inpatient care. Others had a broader role around advice, liaison, prison interface, general adult services, and community risk formulation. Those secondary functions can affect real care, but they are harder to standardize.
The service-design question is capacity allocation: should CFMHS spend most of its energy on direct case management for high-risk patients leaving secure care, or should it also export forensic expertise into general services before risk escalates?
Referral Routes Varied Across Secure Care, Prisons, and General Services
Referral heterogeneity was one of the clearest service-design findings. A service that does not accept referrals from prisons or non-secure inpatient units will shape a different pathway from one that does.
The transition problem is concrete. People with severe mental illness leaving prison or secure hospital can move between services exactly when continuity is hardest, yet the mapping found that only around half of services accepted referrals directly from integrated mental health teams in prison.1
Conditionally discharged patients under Ministry of Justice restrictions were another key interface. Around 60% of services were geared toward moving this group toward step-down into general mental health services, but the approach was not uniform.
DBT, CBT, and Schema Therapy Appeared in Reported Therapy Menus
Psychological intervention data were available from 17 services. Among those services, therapy menus were diverse:
- Dialectical behavior therapy (DBT): 12 of 17 services (71%).
- Cognitive behavioral therapy (CBT): 11 of 17 services (65%).
- Schema therapy: 8 of 17 services (47%).
- Cognitive analytic therapy: 6 of 17 services (35%).
- Compassion-focused therapy and eye movement desensitization and reprocessing: 5 of 17 services each (29%).
The therapy menu is useful only as a map of stated capacity. A service listing DBT or CBT does not tell us the dose, fidelity, wait time, staff competence, patient selection, or outcome effect.
CFMHS Benchmarking Needs Outcomes and Service Functions
England can call 32 services CFMHS, but the label still covers different clinical products. Useful benchmarking would need consistent referral eligibility, direct-care functions, intervention fidelity, and outcomes such as hospitalization, violence, reoffending, continuity of care, patient experience, and family experience.
- Access: who can refer, from which setting, and how quickly the team responds.
- Clinical work: assessment, formulation, therapy, medication coordination, risk planning, and transition support.
- Outcomes: hospitalization, reoffending, violence, continuity, patient experience, and family experience.
Forensic assertive community treatment in the United States has been studied as one possible model, with some evidence for reduced justice-system outcomes, but the field still struggles with heterogeneity in model definition and implementation.3
Risk Work Needs Clear Tiers Instead of Vague Specialist Ownership
Forensic community work often gets pulled between direct responsibility and advisory responsibility. A patient may be too risky for ordinary services to manage comfortably, but not clearly eligible for specialist forensic case management. That middle zone is where vague referral rules create delays.
A tiered model would make the service easier to understand:
- Full CFMHS care coordination: direct specialist case management for people whose risk profile and transition needs exceed ordinary community-team capacity.
- Time-limited joint formulation: shared risk planning when a general adult, prison mental health, or early intervention psychosis team needs forensic input but not full transfer.
- Advice and consultation: lower-intensity support that clarifies thresholds, referral timing, and safety planning before a crisis forces escalation.
The Williams mapping study does not prescribe the right tiers, but it shows why they are needed. Without a common language for service intensity, 2 regions can both claim to have CFMHS coverage while offering very different practical support.
Risk assessment tools support clinical judgment by making the first referral conversation more consistent. Probabilistic tools can make the threshold more transparent, especially when general teams are deciding whether to ask for forensic input before a serious incident occurs.
The service-development target is earlier clarity. Patients, families, and referrers should not have to discover the true service model only after a referral is rejected.
Outcome Research Will Need to Account for Case Mix
Evaluating CFMHS outcomes is harder than evaluating a single medication trial. Teams may serve different mixes of psychosis, personality disorder, substance use, intellectual disability, acquired brain injury, trauma, homelessness, and justice-system involvement.
That case mix changes what success looks like. For one patient, success may be staying out of secure hospital. For another, it may be stable housing, reduced weapon carrying, improved medication adherence, or fewer emergency contacts.
Outcome research should therefore stratify by referral route and service function. A secure-discharge team should not be benchmarked exactly like an advice-and-liaison team that never holds long-term case responsibility.
The Williams map gives the starting taxonomy. The next generation of work needs linked outcomes, staff exposure, patient experience, and local commissioning context so that service differences can be interpreted rather than merely counted.
Patient and Family Experience Should Be Part of Benchmarking
Forensic service evaluation often focuses on risk, admission, and criminal-justice outcomes. Those are necessary, but they do not capture whether patients and families understand the plan, trust the team, or know who is responsible during a crisis.
Families often sit at the boundary between services. They may notice relapse, substance use, paranoia, threats, disengagement, or housing instability before a team does. If CFMHS roles are unclear to referrers, they are usually even less clear to families. Future benchmarking should include whether families know when and how to contact the right service.
Service clarity: a mapped pathway should tell referrers who holds responsibility, who advises, and who responds when risk changes.
Questions About Community Forensic Mental Health Services
Does this study show which CFMHS model works best?
No. It maps service structure and function. The next step is linking those structures to outcomes that patients, services, and communities care about.
Why does prison referral access matter?
Prison release is a high-risk transition for people with serious mental illness. If specialist forensic community teams are hard to access from prison mental health services, continuity can break at the moment it is most needed.
References
- Community forensic mental health services in England: mapping provision, structure and function. Williams et al. doi:10.1192/bjb.2026.10236
- Community forensic mental health service standards. PubMed search. PubMed search
- Forensic assertive community treatment outcomes. PubMed search. PubMed search
- Severe mental illness, prison release, and continuity of care. PubMed search. PubMed search