A 2026 brain tumor prehabilitation study involving 26 surgical patients found that language-targeted non-invasive stimulation plus intensive language training shifted fMRI language activation away from the stimulation target, while measured language and cognition stayed stable.
Research Highlights
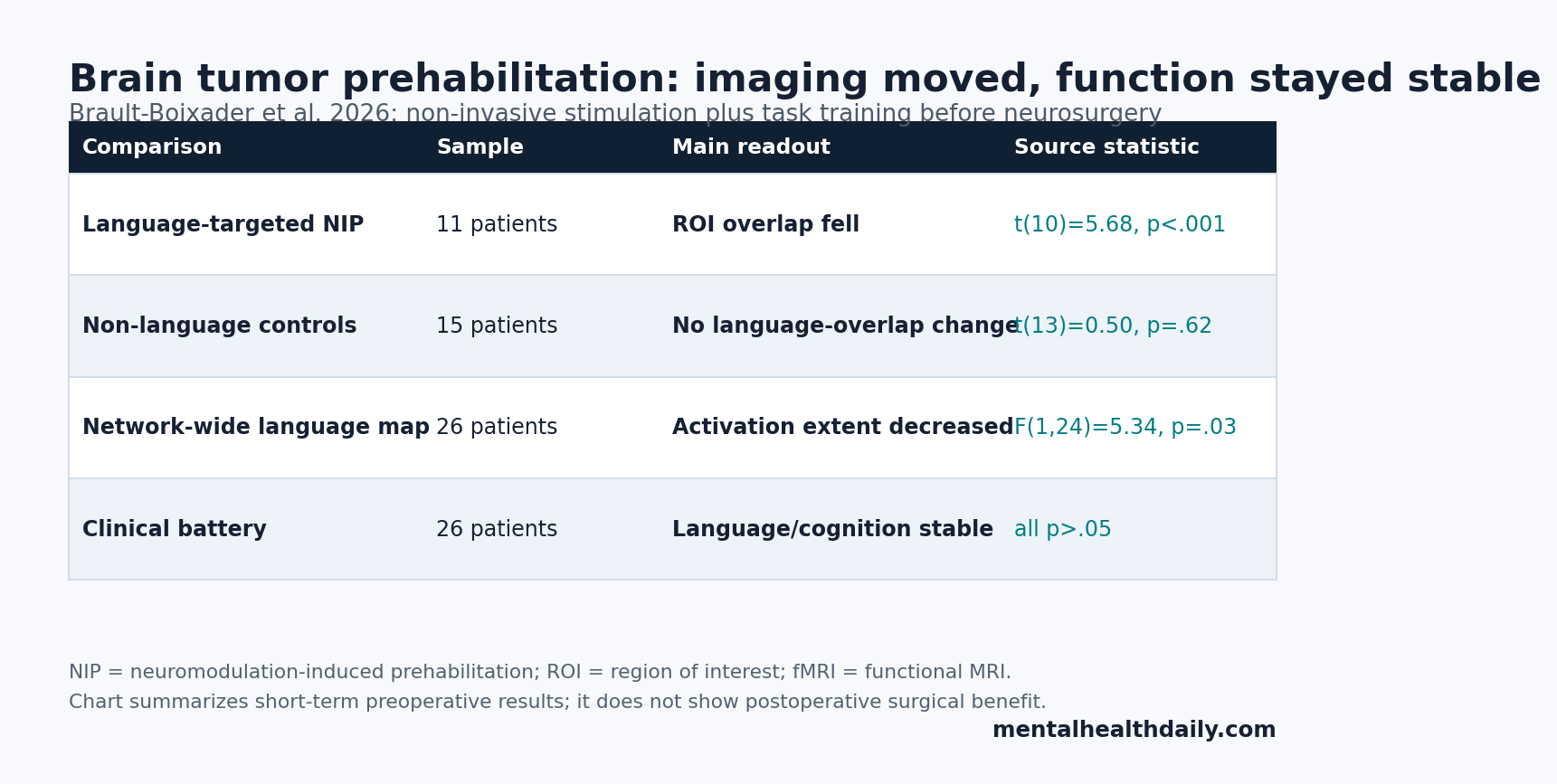
- Language-targeted prehabilitation moved the fMRI signal: the group-by-time interaction for stimulation-target overlap was significant, F(1,23) = 4.61, p = .04, and the 11-patient language group showed a large pre-to-post reduction, t(10) = 5.68, p < .001, d = 1.71.
- Control patients did not show the same language shift: the 15-patient non-language group showed no comparable language-network overlap change, t(13) = 0.50, p = .62, d = 0.14.
- Motor-network effects were not detected: motor ROI overlap did not show a time effect, F(1,21) = 0.13, p = .72, or group-by-time interaction, F(1,21) = 0.62, p = .44.
- Language and cognition stayed stable: Barcelona-Revised language subtests, visuospatial attention, and WAIS-IV block scores showed no significant within-group decline after prehabilitation, with all p values > .05.
- Surgery outcomes remain the missing test: this preprint measured short-term preoperative fMRI and cognition in 26 patients, not postoperative aphasia rates, resection volume, survival, or sham-controlled treatment effects.
Non-invasive prehabilitation means trying to train a vulnerable brain network before surgery so the network depends less on tissue that may need to be resected. In this study, prehabilitation paired non-invasive brain stimulation with intensive task practice before tumor surgery.
Task-based fMRI is functional magnetic resonance imaging collected while a person performs a task, such as phonemic or semantic word generation. For brain tumor surgery, the point is practical: if language activation sits close to tumor tissue, surgeons face a harder tradeoff between removing tumor and preserving speech.
Language-Targeted Stimulation Reduced Peritumoral fMRI Overlap
Brault-Boixader et al. enrolled 30 patients from the Prehabilita program and analyzed 26 after exclusions for imaging or functional-target reasons. The final cohort included 10 women, a mean age of 55.88 years with SD 11.81, and 12 patients with high-grade gliomas.
The language-targeted group included 11 patients whose language-production networks were at surgical risk. Their intervention combined inhibitory-like repetitive transcranial magnetic stimulation or transcranial direct current stimulation with intensive language exercises. Repetitive transcranial magnetic stimulation uses magnetic pulses to change cortical excitability; transcranial direct current stimulation uses weak electrical current to bias neural activity while the person trains the target function.
The main imaging test used a 10 mm region of interest (ROI), a small spherical area centered on each person’s stimulation target. Researchers then measured how much that ROI overlapped with language-related fMRI activation before vs. after prehabilitation.
- Language group: ROI-language activation overlap decreased strongly after prehabilitation, t(10) = 5.68, p < .001, d = 1.71.
- Non-language group: language-network overlap did not significantly change, t(13) = 0.50, p = .62, d = 0.14.
- Post-treatment separation: groups did not differ at baseline, t(23) = 0.57, p = .57, but differed after prehabilitation, t(23) = 2.43, p = .02.
The interpretation is not that language disappeared. It is that measurable task-related activation became less concentrated at the stimulated peritumoral target. For surgical planning, that is the desired direction: less dependence on cortex sitting next to tumor tissue.
Motor-Network Controls Made the Language Result More Specific
The study did not treat every fMRI change as proof of useful plasticity. It used a non-language control group, mostly motor-network prehabilitation, and within-subject motor-network analyses to ask whether stimulation produced a broad nonspecific imaging change.
Motor-network overlap did not show the same pattern. In the non-language group, motor stimulation produced no significant time effect for ROI-cluster overlap, F(1,21) = 0.13, p = .72, and no group-by-time interaction, F(1,21) = 0.62, p = .44. In the language group, the hand-related motor cluster also stayed statistically stable, t(9) = −0.60, p = .56, d = −0.19.
Clinical read: the control pattern supports a targeted language-network effect more than a generic scanner-practice effect. It also fits a plausible biology: language is a distributed association network, while primary motor maps are more spatially constrained and somatotopically organized.
Overall Language Activation Shrank, but Individual Reorganization Varied
Beyond the local ROI test, the study measured the overall volume of task-related language activation. The group-by-time interaction was not significant, F(1,24) = 1.02, p = .32, but there was a main effect of time: language-network size decreased from pre- to post-prehabilitation across participants, F(1,24) = 5.34, p = .03.
That whole-network result is broader and less specific than the ROI result. It says activation extent decreased across the cohort, but it does not by itself prove that language moved to a single safer location.
Descriptive mapping of the 11 language-targeted patients showed why the claim needs calibration. Some patients showed intrahemispheric reorganization, some showed interhemispheric recruitment, and some showed mixed anterior-posterior displacement. Intrahemispheric language-network volume decreased in 9 of 11 patients, while interhemispheric changes were more variable.
Functional reorganization in this context means a change in which brain regions are recruited during a task. It can include local unmasking of nearby tissue, recruitment of distant same-hemisphere regions, or cross-hemisphere compensation. The study’s stronger finding is target overlap reduction; the exact compensatory route varied by patient.
Cognitive Stability Is Encouraging but Not Proof of Surgical Benefit
The safety signal matters because deliberately reducing activation at a language target could be harmful if it weakens the function being trained. In this cohort, language and broader cognitive measures did not show significant decline after prehabilitation.
Clinical testing used the Barcelona-Revised language battery plus non-language measures such as visuospatial attention and WAIS-IV block design. Conversation and narration, picture description, verbal repetition, naming, verbal comprehension, reading comprehension, automatic language, visuospatial attention, and visuoconstruction scores showed no significant within-group worsening after prehabilitation.
Evidence-strength note: this was a small preoperative imaging and neuropsychology study, not a sham-controlled surgical-outcome trial. It can support a claim that language-targeted prehabilitation changed short-term fMRI topography without measurable immediate cognitive decline. It cannot prove that the intervention increases extent of resection, lowers postoperative aphasia risk, improves survival, or replaces awake mapping.
Decision use: the current role is trial planning and risk discussion, especially when language activation sits close to planned resection margins.
A practical trial would also need to record tumor type, lesion location, stimulation target, training dose, and mapping results together.
Earlier Brain Tumor Prehabilitation Evidence Was Mostly Case-Based
The 2026 paper sits on a narrow but coherent prehabilitation literature. Boccuni et al. first described the Prehabilita protocol in 2023, pairing non-invasive brain stimulation with intensive function-specific training before brain tumor surgery. That protocol made the intervention testable, but it did not by itself prove that language-network topography changed.
Subsequent reports moved closer to the current question. A 2024 Journal of Neuro-Oncology case series reported widespread fMRI cortical reorganization after non-invasive prehabilitation, and a 2024 Frontiers in Oncology case report examined language-network plasticity in detail. Dadario et al. also described parcel-guided TMS prehabilitation and rehabilitation in a proof-of-concept brain tumor surgery case.
Compared with those earlier pieces, the 2026 study added 2 useful controls: a non-language comparison group and motor-network analyses. That does not solve every design problem, but it makes the language-network interpretation less dependent on a single spectacular case.
Prehabilitation Should Complement Mapping, Not Replace It
Awake mapping means testing language, movement, or other functions during surgery while stimulating cortical and subcortical tissue. It remains the higher-stakes clinical safety procedure because it tests function directly in the operative field.
Non-invasive prehabilitation has a different role. It may prepare the network before the operation, especially when tumor-adjacent language activity creates a narrow surgical window. The proper clinical sequence is not “train instead of map.” It is closer to: identify risk with MRI and functional testing, try to reduce dependence on the risky region when appropriate, then still map function during surgery if the case requires it.
Several limitations keep the intervention specialized. Tumor growth can itself reshape networks. Stimulation dose, target choice, language-training intensity, and lesion anatomy can all change response. Patients were not randomized to sham stimulation, so task practice and repeated testing remain possible contributors. Postoperative endpoints were outside this paper’s main analysis.
Questions About Brain Tumor Prehabilitation
Did the study prove that non-invasive prehabilitation makes brain tumor surgery safer?
No. It showed short-term preoperative fMRI reorganization with stable measured language and cognition. Surgical safety would require postoperative language outcomes, extent-of-resection data, complications, and ideally sham-controlled or randomized comparisons.
Why combine stimulation with language training?
Stimulation is meant to bias the excitability of the vulnerable region, while task training repeatedly engages the broader language network. Pairing the 2 is supposed to encourage alternative language routes more than passive stimulation alone.
Was the result the same in every patient?
No. The overall direction favored less peritumoral language activation, but individual maps varied. Some patients showed same-hemisphere shifts, some recruited cross-hemisphere regions, and some showed mixed anterior-posterior displacement.
Who might this eventually help?
The most plausible future use is for selected patients whose tumors sit close to language cortex and whose teams have access to advanced fMRI, stimulation targeting, language therapy, and intraoperative mapping. Routine use would need stronger outcome data than this preprint provides.
References
- Brault-Boixader N, Roca-Ventura A, Delgado-Gallen S, Buloz-Osorio E, Boccuni L, Laredo C, et al. Non-invasive prehabilitation before neurosurgery modifies the topography of brain language networks without compromising function. medRxiv. 2026. doi:10.64898/2026.04.13.26350473
- Boccuni L, Roca-Ventura A, Buloz-Osorio E, Leno-Colorado D, Cabello-Toscano M, Delgado-Gallen S, et al. Neuromodulation-induced prehabilitation to leverage neuroplasticity before brain tumor surgery: a single-cohort feasibility trial protocol. Frontiers in Neurology. 2023;14. doi:10.3389/fneur.2023.1243857
- Boccuni L, Roca-Ventura A, Buloz-Osorio E, Leno-Colorado D, Delgado-Gallen S, Cabello-Toscano M, et al. Non-invasive prehabilitation to foster widespread fMRI cortical reorganization before brain tumor surgery: lessons from a case series. Journal of Neuro-Oncology. 2024. doi:10.1007/s11060-024-04774-4
- Boccuni L, Roca-Ventura A, Buloz-Osorio E, Leno-Colorado D, Martin-Fernandez J, Cabello-Toscano M, et al. Exploring the neural basis of non-invasive prehabilitation in brain tumour patients: an fMRI-based case report of language network plasticity. Frontiers in Oncology. 2024;14:1390542. doi:10.3389/fonc.2024.1390542
- Dadario N, Young I, Zhang X, Teo C, Doyen S, Sughrue M. Prehabilitation and rehabilitation using data-driven, parcel-guided transcranial magnetic stimulation treatment for brain tumor surgery: proof of concept case report. Brain Network and Modulation. 2022;1:48. doi:10.4103/2773-2398.340144
- Nieberlein L, Rampp S, Gussew A, Prell J, Hartwigsen G. Reorganization and plasticity of the language network in patients with cerebral gliomas. NeuroImage: Clinical. 2023;37:103326. doi:10.1016/j.nicl.2023.103326
- Hartwigsen G, Volz LJ. Probing rapid network reorganization of motor and language functions via neuromodulation and neuroimaging. NeuroImage. 2021;224:117449. doi:10.1016/j.neuroimage.2020.117449