
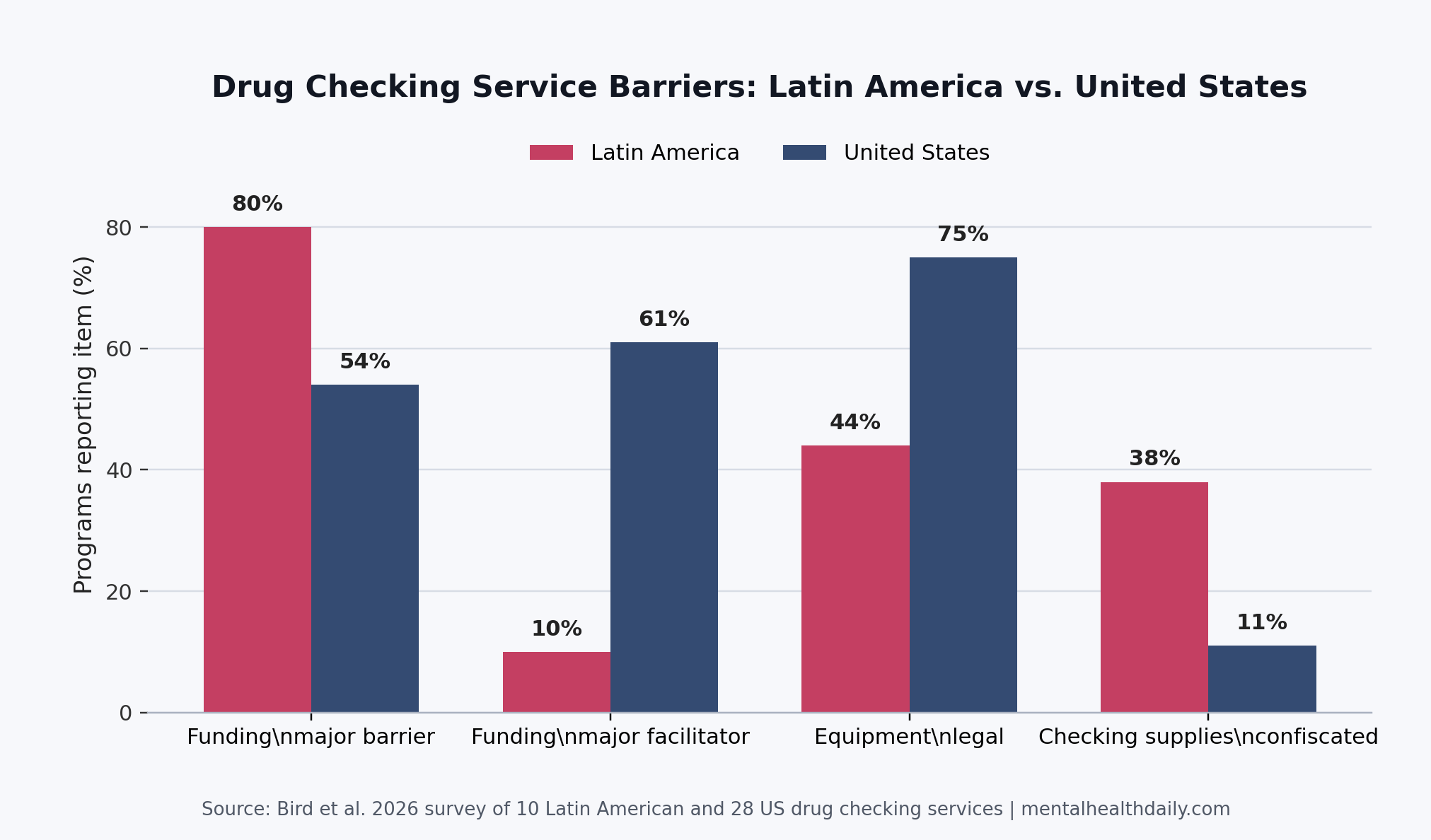
A 2026 survey of 38 drug checking services found that Latin American programs faced a different operating reality than US programs: funding was a major barrier more often (80% vs. 54%), drug checking equipment was legally permitted less often (44% vs. 75%), and law enforcement confiscation of checking supplies was reported more often (38% vs. 11%).
Research Highlights
- Funding was the main implementation gap: 80% of Latin American drug checking services called funding a major barrier, compared with 54% of US services.
- Legal protection lagged behind: 44% of Latin American programs said drug checking equipment was legal in their state or territory, compared with 75% of US programs.
- Confiscation risk was higher: 38% of Latin American respondents reported law enforcement confiscation of drug checking kits, strips, or devices in the past year, compared with 11% of US respondents.
- Service models diverged: Latin American programs were more often mobile (50% vs. 7%) and more often offered supervised drug consumption (30% vs. 4%) and mental health or counseling services (40% vs. 18%).
- Drug markets differed: fentanyl was commonly brought for testing at 20% of Latin American programs and 79% of US programs, while Latin American staff described tusi and nightlife drug checking as separate practical problems.
Drug checking services are harm-reduction programs that chemically test pills, powders, or other drug samples and pair the result with safer-use counseling. In opaque drug markets, the service has 2 jobs at once: help the person in front of the tester make a less blind decision, and turn anonymous samples into public health surveillance.
Bird et al. compared 10 Latin American services with 28 US services and added a 110-minute Spanish-language focus group with staff from 6 Latin American organizations.1 The sample is small and descriptive, but the pattern is clinically relevant because overdose prevention depends on whether a service can legally exist, keep equipment, buy reliable testing technology, and reach people who use drugs.
80% of Latin American Programs Reported Funding as a Major Barrier
Funding produced the sharpest difference in the 2026 survey. Latin American programs reported funding as a major barrier more often than US programs (80% vs. 54%) and reported funding as a major facilitator far less often (10% vs. 61%).
The funding source pattern explained part of that gap. In the US group, 36% of services reported state or provincial health department funding and 25% reported local or regional health department funding. In the Latin American group, both figures were 0%.
Operational consequence: staff described too few paid workers, limited physical space, and difficulty buying equipment such as Fourier-transform infrared spectroscopy (FTIR), a lab method that identifies substances by how they absorb infrared light. Without that kind of technology, programs may rely more heavily on test strips, color reagents, or off-site analysis.
Maghsoudi et al. reviewed drug checking services for people who use drugs and found a broad but uneven evidence base: services can support risk communication and surveillance, but implementation varies by setting, technology, and target population.2 Bird et al. add a simple point to that literature: a service can be conceptually useful and still be structurally fragile if it has no stable funding stream.
Legal Ambiguity Reached the Equipment Itself
Only 44% of Latin American respondents said possession of drug checking equipment was legal in their state or territory, compared with 75% of US respondents. Another 44% of Latin American respondents selected “other,” which in this context signals legal ambiguity rather than confidence.
Confiscation data sharpen that point. Among respondents who answered the confiscation question, 38% of Latin American programs reported that staff, volunteers, or clients had drug checking kits, strips, or devices confiscated by law enforcement in the past year. The corresponding US figure was 11%.
Laing et al. argued that drug checking could be a strategic overdose response in the fentanyl era because it gives people more information in a contaminated drug market.3 That argument only works if the person providing the service is not at risk of losing the very equipment needed to test the drug.
Implementation lesson: decriminalizing personal drug possession is not the whole legal question. Programs also need explicit protection for test strips, color reagents, spectroscopy devices, drug residue handling, and the paraphernalia that often surrounds real-world drug checking.
Latin American Services Were More Mobile and More Mixed in Scope
Service structure differed by region. Latin American programs were more often mobile (50% vs. 7%) or mixed mobile-and-stationary (50% vs. 43%). None of the Latin American programs described themselves as purely stationary, compared with 46% of US programs.
Testing mode also differed. US programs more often offered on-site testing (89% vs. 60%) and off-site laboratory testing (64% vs. 20%). Latin American programs more often offered take-home self-testing kits (50% vs. 43%), although that difference was smaller.
The other-service profile split by service type. US programs more often offered syringe services (75% vs. 30%), naloxone distribution (82% vs. 30%), medications for opioid use disorder (32% vs. 10%), and case management (39% vs. 10%). Latin American programs more often reported supervised drug consumption (30% vs. 4%) and mental health or counseling services (40% vs. 18%).
Two operating worlds: the Mexico-US border services described work with people who inject drugs, unstable housing, migration, sex work, fentanyl, methamphetamine, and supervised consumption. Programs in central Mexico, Colombia, Peru, and Chile described nightlife drug checking for concerts, festivals, raves, MDMA, cocaine, LSD, and tusi.
Tusi and Fentanyl Created Different Testing Problems
Fentanyl was commonly brought for testing at 79% of US drug checking services but only 20% of Latin American services. Xylazine appeared in 25% of US service reports and 0% of Latin American service reports. In Latin America, staff highlighted tusi, a pink powder mixture often sold under a name that implies 2C-B or cocaine but commonly contains ketamine, MDMA, caffeine, or other substances.
Why tusi is difficult: colorimetric tests are designed around expected reactions for specific substances. A mixed powder can contain several psychoactive drugs at once, so a simple positive-or-negative result may not tell the user what they need to know.
Goodman-Meza et al. showed why actionable results can still matter at the individual level. In a northern Mexico safe-consumption setting, 30 women who injected drugs tested samples for fentanyl; when a sample was fentanyl-positive, 14 used less and 1 did not use the sample.4
Behavior-change mechanism: the pilot was small, but it shows how drug checking can change risk when the result arrives in a form people can use.
Park et al. surveyed North American drug checking services operating in 2022 and found wide variation in service setting, technology, and program integration.5 Bird et al. extend that service-level picture southward and show that the hardest constraint may be political economy, not chemistry.
Violence Risk Changes the Meaning of Outreach
The focus group added context the survey could not capture. Staff near the Mexico-US border described fear of organized criminal networks as a barrier to community outreach, especially when fentanyl entered local heroin markets. That is not a standard implementation issue like staffing or training. It changes where outreach can safely happen and what warnings staff can give without exposing clients or workers to retaliation.
That qualitative signal also keeps the policy interpretation grounded. A program can be mobile on paper and still constrained if street outreach places workers at risk. A service can have community trust and still lack permission, money, or safety to operate at useful scale.
Evidence-strength note: this was a preprint, not a randomized intervention study. It cannot prove that funding reform, legal protection, or government support would reduce overdose deaths by a specific percentage. It can support a narrower claim: surveyed Latin American drug checking services reported more legal, funding, and confiscation barriers than US services, and staff accounts made those barriers operational rather than abstract.
Drug Checking Policy Has to Protect the Service Infrastructure
The most useful read is practical. Drug checking is often discussed as a technical intervention: a strip, a reagent, a spectrometer, a mass spectrometry partnership. Bird et al. show the service layer underneath the technology.
- Stable funding: programs need paid staff, space, and testing equipment reliable enough for the local drug supply.
- Explicit legal protection: equipment, samples, residues, and paraphernalia need clear exemptions so police action does not erase the service.
- Local fit: fentanyl-focused border services, nightlife tusi services, and US opioid-overdose programs need different testing tools and counseling scripts.
- Worker safety: outreach models have to account for violence risk alongside client demand.
Drug checking can reduce blind drug use only when people can reach the service, trust the result, and act on the information. The 2026 comparison suggests that in Latin America, the bottleneck is often whether the service has enough legal and institutional room to function.
Questions About Drug Checking Services
Does drug checking prevent overdose?
Evidence limit: drug checking can support overdose prevention by identifying unexpected substances and changing behavior before use, but the evidence is not a mortality trial.
Strongest claim: testing can reveal fentanyl, xylazine, tusi components, or other unexpected drugs, and some studies show people change use plans after receiving results.
Why compare Latin America with the United States?
The comparison shows that the same harm-reduction tool faces different implementation constraints. US services in this survey more often had government funding, stationary sites, naloxone distribution, and opioid-focused testing. Latin American services more often worked through mobile/community-based models and reported legal ambiguity, confiscation, and funding gaps.
Is this enough evidence to redesign policy?
It is enough to identify concrete policy targets, not enough to quantify mortality benefit. Legal protection for drug checking supplies, stable health-system funding, and service models matched to local drug markets are the actionable targets suggested by the evidence.
References
- Bird JA, Rosen JG, Arredondo Sanchez Lira J, Green TC, Park JN. Drug Checking Services in Latin America vs. the United States: Staff Perspectives, Program Characteristics, and Barriers to Implementation. medRxiv. 2026. https://doi.org/10.64898/2026.04.11.26350657
- Maghsoudi N, Tanguay J, Scarfone K, et al. Drug checking services for people who use drugs: A systematic review. Addiction. 2022;117(3):532-544. https://doi.org/10.1111/add.15734
- Laing MK, Tupper KW, Fairbairn N. Drug checking as a potential strategic overdose response in the fentanyl era. International Journal of Drug Policy. 2018;62:59-66. https://doi.org/10.1016/j.drugpo.2018.10.001
- Goodman-Meza D, Arredondo J, Slim S, et al. Behavior change after fentanyl testing at a safe consumption space for women in Northern Mexico: A pilot study. International Journal of Drug Policy. 2022;106:103745. https://doi.org/10.1016/j.drugpo.2022.103745
- Park JN, Tardif J, Thompson E, Rosen JG, Arredondo Sanchez Lira J, Green TC. A survey of North American drug checking services operating in 2022. International Journal of Drug Policy. 2023;121:104206. https://doi.org/10.1016/j.drugpo.2023.104206
- Bailey K, Abramovitz D, Artamonova I, et al. Drug checking in the fentanyl era: Utilization and interest among people who inject drugs in San Diego, California. International Journal of Drug Policy. 2023;118:104086. https://doi.org/10.1016/j.drugpo.2023.104086