
A 2026 targeted metabolomics study of knee osteoarthritis found 33 altered serum metabolites and 10 altered cerebrospinal-fluid metabolites, but the symptom signal split by compartment: serum amino acids, bile acids, and acylcarnitines tracked pain or fatigue, while CSF histamine and 3-hydroxyphenylacetic acid tracked central pain and sleep measures.1
Research Highlights
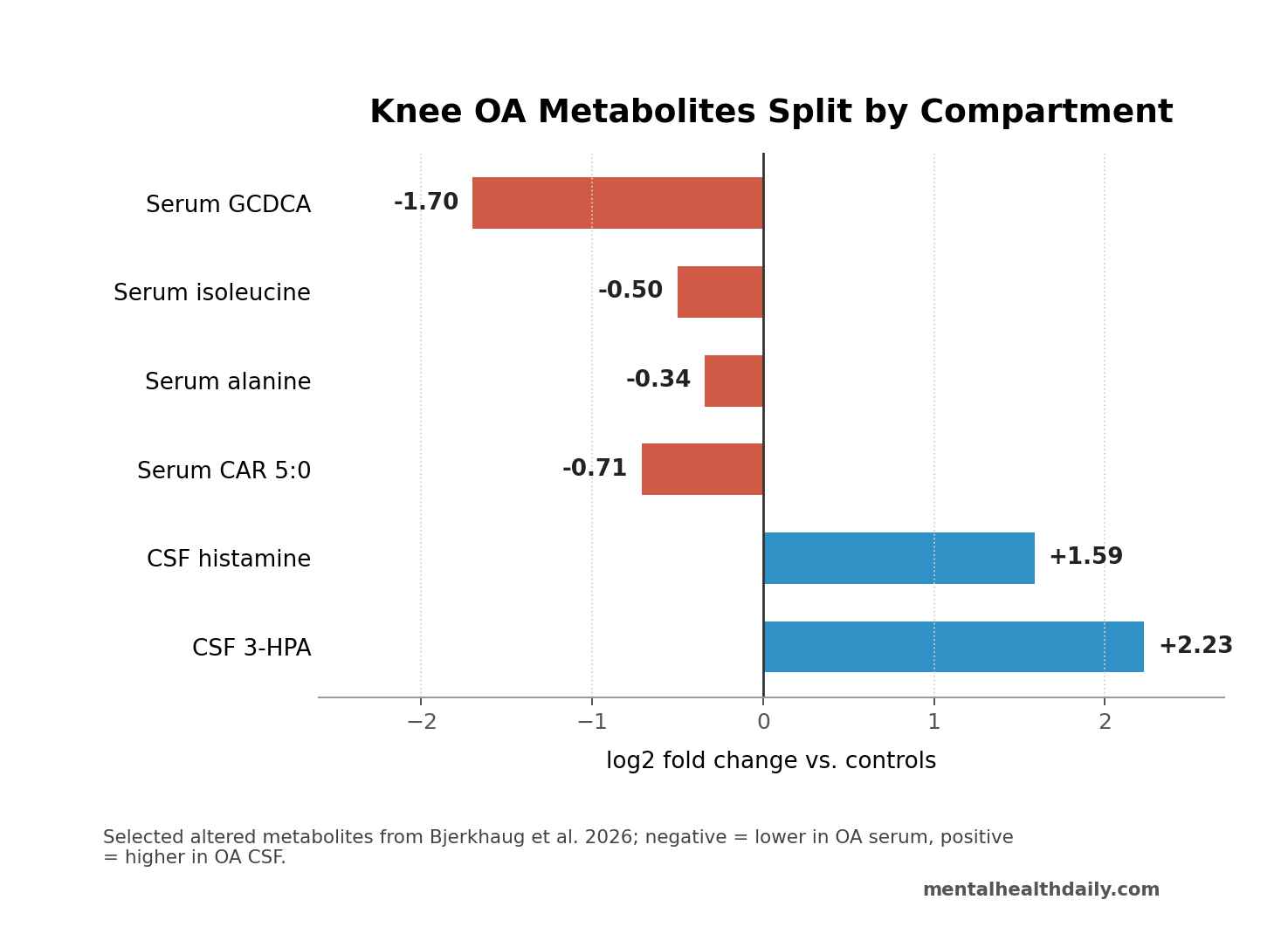
- 33 serum metabolites shifted: knee osteoarthritis patients had lower levels of 11 amino acids, 5 bile acids, and 4 lipids vs. healthy controls, while uracil was higher.1
- 10 CSF metabolites shifted: CSF 3-hydroxyphenylacetic acid rose by log2 FC 2.23 and histamine rose by log2 FC 1.59 vs. non-inflammatory neurological controls.1
- Fatigue tracked energy metabolism: lower alanine, isoleucine, creatine, and short-chain acylcarnitines were associated with higher fatigue ratings in the 36-person OA cohort.1
- Bile-acid findings were not simple: serum GCDCA was lower in OA patients by log2 FC −1.70, yet OA patients with relatively higher GCDCA reported higher average pain.1
- Evidence remains exploratory: the design was cross-sectional, serum analysis used 32 OA samples, and CSF controls were 39 non-inflammatory neurological-symptom patients rather than healthy volunteers.1
Metabolomics means measuring many small molecules at once — amino acids, bile acids, lipids, nucleotides, and related compounds — to see which biochemical pathways differ between groups or track symptoms. In chronic pain, that approach is useful because pain severity rarely maps cleanly onto joint damage alone.
Knee osteoarthritis is often described as a wear-and-tear disease, but painful OA behaves more like a peripheral-plus-central condition. Joint inflammation, nociceptor sensitization, spinal glial activation, brain pain modulation, sleep disruption, fatigue, anxiety, and depressed mood can all become part of the clinical pattern.2,3,4
36 Knee OA Patients Showed Pain, Fatigue, Sleep, and Mood Burden
Bjerkhaug et al. studied 36 people with radiologically confirmed knee osteoarthritis whose knee pain was severe enough to make them candidates for total knee replacement. Serum was available from 32 OA patients and 38 healthy controls; CSF was available from 36 OA patients and 39 controls with non-inflammatory neurological symptoms.1
The symptom separation was large. OA patients reported average pain of 48.8 on a 0–100 visual analog scale vs. 2.1 in healthy controls, current pain of 40.4 vs. 2.2, and worse sleep quality with Pittsburgh Sleep Quality Index scores of 8.4 vs. 3.7. Fatigue also separated the groups: Multidimensional Fatigue Inventory total scores averaged 50.1 in OA patients vs. 33.4 in controls.1
Pressure pain testing added a sensory readout. Pressure pain threshold at the affected knee was lower in OA patients, 344.5 kPa vs. 448.4 kPa, meaning less pressure was needed before the sensation became painful. Average pressure threshold across knee, trapezius, and gluteal sites did not differ significantly, which argues against treating this cohort as a simple whole-body hyperalgesia sample.
Serum Metabolism Pointed to Amino Acids, Bile Acids, and Fatigue
Serum results were mostly lower in OA patients than in healthy controls. The altered set included branched-chain amino acids — isoleucine, leucine, and valine — plus alanine, asparagine, histidine, ornithine, proline, threonine, tryptophan, and tyrosine. Several amino-acid derivatives were also lower, including creatine and methionine sulfoxide.1
Branched-chain amino acids are essential dietary amino acids involved in muscle protein turnover and energy metabolism. Their lower serum levels in this OA cohort are interesting but not a clean disease signature because fasting status differed: OA patients had fasted before surgery, while healthy controls were not handled identically. That design detail weakens any simple “low amino acids cause OA pain” interpretation.
Symptom correlations were more clinically useful than the group difference alone. Lower alanine and isoleucine were associated with higher total fatigue. Lower propionylcarnitine, isobutyrylcarnitine, and isovalerylcarnitine were also associated with higher fatigue, and isovalerylcarnitine was associated with worse sleep disturbance and anxiety.1
Acylcarnitines help move fatty-acid fragments into mitochondria for energy production. A fatigue link therefore has biological plausibility: the finding points toward energy handling and mitochondrial stress rather than only joint loading. It still does not prove causality. Fatigue can change activity, diet, sleep, medication use, and metabolic state, and each of those can feed back into serum chemistry.
GCDCA Was Lower Overall but Higher Within OA Pain Severity
The bile-acid signal was the most calibration-heavy part of the paper. Glycocholic acid, glycochenodeoxycholic acid, glycodeoxycholic acid, taurocholic acid, and taurodeoxycholic acid were lower in OA patients than healthy controls. Serum GCDCA, a conjugated primary bile acid, showed a log2 fold change of −1.70, with a 95% CI from −2.39 to −1.01 and q = 0.000085.1
Within the OA group, however, higher GCDCA was associated with higher average pain. GCA and GCDCA were also associated with lower Knee Injury and Osteoarthritis Outcome Score results, where lower KOOS means more severe knee-related symptoms and functional limitation.
That is not a contradiction to flatten away. It means 2 levels of analysis are being mixed:
- Between-group biology: OA patients had lower bile-acid levels than healthy controls.
- Within-OA symptom biology: among OA patients, relatively higher GCDCA tracked higher average pain.
Bile-acid pathway context: Yang et al. linked bile-acid profiles, gut microbiota, farnesoid-X-receptor signaling, and glucagon-like peptide-1 pathways to osteoarthritis biology in experimental and human analyses.5
Bjerkhaug et al. add human serum symptom data, but they do not show that changing bile acids would reduce pain.
CSF Findings Pointed to Central Pain Modulation
CSF results moved in the opposite broad direction from serum. OA patients had higher CSF levels of 3-hydroxyphenylacetic acid, histamine, indole, glutarylcarnitine, eicosapentaenoic acid, methylthioadenosine, phenylacetaldehyde, and N-acetylglucosamine than non-inflammatory neurological controls; adenine and vitamin B3 were higher in controls.1
Cerebrospinal fluid is the fluid around the brain and spinal cord. It is not the same as brain tissue, but it sits closer to central nervous system chemistry than blood does.
In this study, CSF histamine was higher in OA patients than controls, yet within OA patients it was negatively associated with knee pain intensity and sleep disturbance. The researchers interpreted that pattern as compatible with central histamine having pain-modulating or compensatory effects rather than acting like a straightforward peripheral inflammatory signal.1,6
3-hydroxyphenylacetic acid showed a different symptom link: higher CSF levels were associated with greater pressure pain sensitivity at the knee, meaning lower local pressure pain threshold. That finding ties a central metabolite to an evoked-pain measure rather than only to a questionnaire.
Serum-CSF correlations added a transport clue. Paraxanthine, trigonelline, and indole-3-acetic acid had high CSF-to-serum correlations at r ≥ 0.7, while glutamic acid and histamine showed negative correlations. Six metabolites — indole-3-propionic acid, GDCA, linoleic acid, biliverdin, deoxycarnitine, and trimethylamine N-oxide — correlated both between serum and CSF and with albumin quotient, a marker of blood-brain-barrier permeability.1
Prior Knee OA Work Already Pointed Beyond Cartilage
Painful knee OA already sits inside a decade of work showing joint damage, inflammatory signaling, and central pain processing acting together.
Serum and lipid context: Mehta et al. identified serum amino-acid metabolism associated with pain in symptomatic knee OA, which matches the amino-acid direction in Bjerkhaug et al.7 Khoury et al. linked lipid biomarkers to chronic joint pain across joint diseases, including lysophosphatidylcholine 16:0 pathways relevant to acid-sensing ion channel 3 activation.8
Neuroimmune studies from the same broader research program also matter. Kosek et al. reported that cytokine-symptom associations differed depending on whether inflammatory markers were measured in synovial fluid or CSF.3 Palada et al. later found elevated CSF inflammatory proteins in painful knee OA associated with reduced symptom severity, a direction that fits the idea that some central immune signals may be compensatory rather than purely pain-amplifying.4
Mechanism layer: peripheral brain-derived neurotrophic factor and TrkB signaling can increase OA joint pain in rodent models, while glial activation in dorsal root ganglia and spinal cord has been tied to chronic OA-like pain.9,10
Those models cannot be pasted directly onto a 36-person human metabolomics cohort, but they explain why serum-only biomarker hunting is too narrow.
Metabolite Biomarkers Are Not Ready for Individual Pain Triage
Several design limits keep this study in the discovery lane.
- Small sample: the core OA group had 36 patients, and serum analysis used 32 OA samples.
- Cross-sectional timing: metabolites and symptoms were measured at one point, so direction cannot be determined.
- Control mismatch: CSF controls were younger and had neurological symptoms; healthy people are not usually sampled for CSF for ethical reasons.
- Fasting mismatch: OA patients were sampled around surgery after fasting, while healthy serum controls were not matched on that detail.
- Multiple pathways: pain, fatigue, sleep, depression, anxiety, medication exposure, BMI, and activity can all influence metabolism.
Mechanistic conclusion: painful knee OA may involve different peripheral and central metabolic states, with fatigue leaning toward amino-acid and acylcarnitine energy pathways and pain/sleep measures showing bile-acid and CSF metabolite links.
The evidence does not justify ordering a metabolite panel to decide who should get surgery, opioids, injections, supplements, or bile-acid-targeting treatment.
Questions About Knee OA Pain and Metabolomics
Does this mean knee osteoarthritis is a brain disease?
No. Knee OA starts with joint pathology, mechanical loading, cartilage, bone, synovium, and local inflammation.
Persistent pain can also recruit central nervous system pathways, including spinal and brain-mediated pain modulation. CSF findings support a central component, not a brain-only explanation.1,3,4
Can serum metabolites diagnose painful knee OA?
Not yet. The study found group differences and symptom correlations, but it was not designed as a diagnostic test. A useful biomarker would need replication, standardized sampling, independent validation, and proof that it adds information beyond symptoms, imaging, and clinical examination.
Why did serum and CSF move in different directions?
Blood and CSF are different compartments. Serum reflects systemic metabolism, diet, muscle, liver, gut, adipose tissue, medications, and inflammation. CSF sits closer to central nervous system chemistry. The opposite direction — many serum metabolites lower, several CSF metabolites higher — is exactly why compartment-specific sampling matters.
Do bile acids explain knee pain?
They may be part of the biology, especially through gut-joint and metabolic signaling, but they do not explain knee pain by themselves. In Bjerkhaug et al., bile acids were lower in OA patients overall, while OA patients with relatively higher GCDCA reported higher average pain. That layered pattern needs replication before it becomes a treatment target.1,5
Does histamine help or worsen pain?
It depends on compartment and receptor context. Peripheral histamine can contribute to inflammation and nociception, but central histamine also participates in wakefulness and pain modulation. In this study, CSF histamine was higher in OA patients but lower CSF histamine within OA was associated with worse knee pain and sleep disturbance.1,6
What should patients take from the study?
Persistent knee OA pain is not always proportional to joint imaging. Fatigue, sleep disruption, mood symptoms, and pain sensitivity can reflect broader biology. That supports more complete clinical assessment, but it does not support self-treating based on metabolite theories or replacing established OA care with supplement protocols.
References
- Bjerkhaug AU, Jakobsson JE, Ahmed AS, et al. Distinct serum and cerebrospinal fluid metabolic signatures associate with pain and fatigue in knee osteoarthritis. Brain, Behavior, & Immunity – Health. 2026;53:101227. doi:10.1016/j.bbih.2026.101227
- Dainese P, Van Wyngaert K, De Mits S, Wittoek R, Van Ginckel A, Calders P. Association between knee inflammation and knee pain in patients with knee osteoarthritis: a systematic review. Osteoarthritis and Cartilage. 2022;30:516-534. PubMed
- Kosek E, Finn A, Ultenius C, Hugo A, Svensson C, Ahmed AS. Differences in neuroimmune signalling between male and female patients suffering from knee osteoarthritis. Journal of Neuroimmunology. 2018;321:49-60. PubMed
- Palada V, Ahmed AS, Freyhult E, Hugo A, Kultima K, Svensson CI, Kosek E. Elevated inflammatory proteins in cerebrospinal fluid from patients with painful knee osteoarthritis are associated with reduced symptom severity. Journal of Neuroimmunology. 2020;349:577391. doi:10.1016/j.jneuroim.2020.577391
- Yang W, et al. Bile acid receptor signaling and gut microbiota in osteoarthritis biology. Nature Communications. 2025. PubMed
- Panula P, Nuutinen S. The histaminergic network in the brain: basic organization and role in disease. Nature Reviews Neuroscience. 2013;14:472-487. PubMed
- Mehta O, Vijay A, Gohir SA, et al. Serum metabolome analysis identified amino-acid metabolism associated with pain in people with symptomatic knee osteoarthritis: a cross-sectional study. Journal of Pain. 2023;24:1251-1261. PubMed
- Khoury S, Colas J, Breuil V, et al. Identification of lipid biomarkers for chronic joint pain associated with different joint diseases. Biomolecules. 2023;13. PubMed
- Gowler PRW, Li L, Woodhams SG, et al. Peripheral brain-derived neurotrophic factor contributes to chronic osteoarthritis joint pain. Pain. 2020;161:61-73. PubMed
- Adaes S, Almeida L, Potes CS, et al. Glial activation in the collagenase model of nociception associated with osteoarthritis. Molecular Pain. 2017;13:1744806916688219. doi:10.1177/1744806916688219