
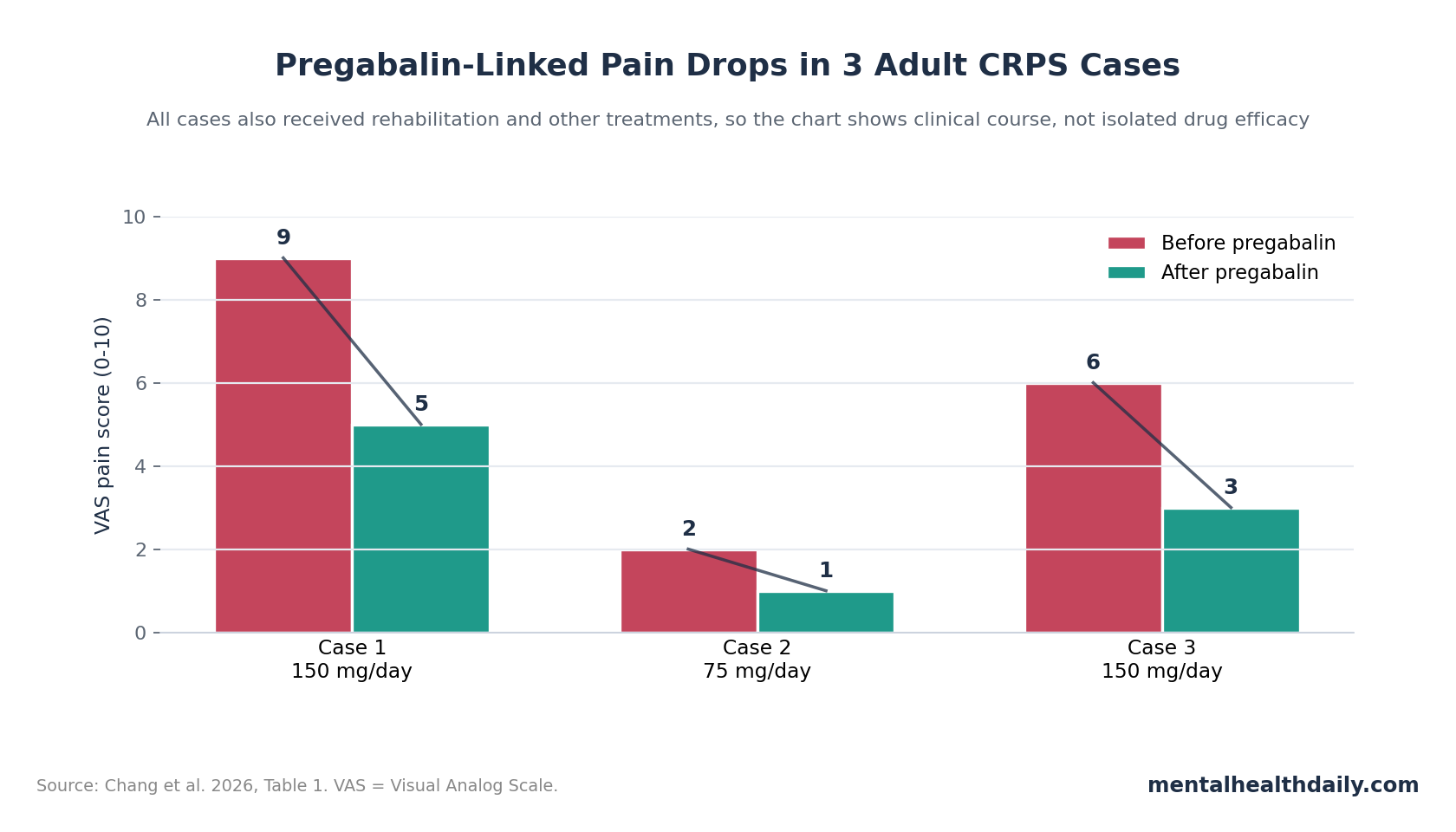
A 2026 Taiwanese case series reported VAS pain drops in all 3 adults treated with pregabalin for type I complex regional pain syndrome: 9 to 5, 2 to 1, and 6 to 3 after doses of 75-150 mg/day. The signal is clinically interesting because pain relief helped rehabilitation participation, but the evidence remains weak because every patient also received other treatments and this case series had no control group.1
Research Highlights
- 3 adult CRPS cases improved: Chang et al. reported VAS pain changes of 9 to 5, 2 to 1, and 6 to 3 after pregabalin was added to multimodal care.1
- Doses were modest: The 3 cases used 75 mg/day or 150 mg/day, below many neuropathic-pain trial doses, yet each patient resumed more physical or occupational therapy.1
- 1 scan improved: One patient had less prominent tracer uptake on a 6-month follow-up three-phase bone scan, giving a small objective signal beyond pain scoring.1
- CRPS evidence is still thin: A 2023 Cochrane overview found very low-certainty evidence across adult CRPS interventions, so this 3-person series should be read as hypothesis-generating.2
- Neuropathic-pain support does not settle CRPS: Pregabalin has broader neuropathic-pain evidence, including NNT 7.7 in a 2015 meta-analysis, but CRPS has vasomotor, inflammatory, and psychological features that make simple extrapolation risky.3
Complex regional pain syndrome (CRPS) is a pain condition in which severe limb pain is accompanied by sensory, temperature, sweating, color, swelling, motor, or tissue-change symptoms. Type I CRPS means the syndrome appears without a confirmed discrete nerve injury; type II means a nerve injury is identifiable.
Pregabalin is an alpha-2-delta calcium-channel ligand: it binds an auxiliary calcium-channel subunit and can reduce release of excitatory neurotransmitters involved in pain signaling. That mechanism makes pregabalin plausible for neuropathic pain, but plausibility is weaker than proof in CRPS because CRPS often combines peripheral inflammation, central sensitization, autonomic dysregulation, movement avoidance, and body-perception disturbance.
VAS Pain Scores Fell in All 3 Pregabalin-Treated CRPS Cases
Chang et al. retrospectively reviewed 3 adults treated at a rehabilitation department in Taiwan between January 2022 and March 2025. Diagnosis was based on the Budapest criteria, the standard symptom-and-sign framework for CRPS, and each case also had supportive three-phase bone scintigraphy, an imaging test that tracks blood-flow and bone-turnover patterns but is not the diagnostic gold standard.
The cases were neurologically complicated rather than clean post-fracture CRPS cases:
- Case 1: A 61-year-old man developed right shoulder and hand CRPS after left basal ganglia and centrum semiovale infarction with right hemiplegia and Broca’s aphasia. Pregabalin 150 mg/day was followed by a VAS pain drop from 9 to 5, rehabilitation participation, improved daily function, and less prominent tracer uptake at 6 months.1
- Case 2: A 49-year-old woman developed right-foot CRPS after left thalamic intracerebral hemorrhage with right hemiplegia. Pregabalin 75 mg/day was followed by VAS improvement from 2 to 1 and more intensive weight-bearing and gait rehabilitation.1
- Case 3: An 82-year-old man developed right wrist and hand CRPS after cervical myeloradiculopathy and surgery. Pregabalin 150 mg/day was followed by VAS improvement from 6 to 3, then pain control around 1-2 while continuing occupational therapy and sleeping with fewer breakthrough-pain interruptions.1
The central reader question is whether these numbers justify stronger pregabalin claims. They do not, but they make the treatment worth testing more carefully: all 3 patients moved in the desired direction, and the benefits were described in functional terms rather than pain-score language alone.
The Pain Signal Was Entangled With Rehabilitation and Procedures
A 3-patient case series can show a clinical course, not isolated drug efficacy. That distinction is especially important in CRPS because early functional restoration is itself part of treatment, and reduced fear, swelling, sleep disruption, and guarding can all reinforce one another.
Each case involved more than pregabalin:
- Case 1: non-steroidal anti-inflammatory drugs (NSAIDs), steroid injections, suprascapular nerve block, physical therapy, and occupational therapy.
- Case 2: baclofen, botulinum toxin injections for spasticity, physical therapy, and occupational therapy.
- Case 3: tramadol, celecoxib, steroid injection, nerve hydrodissection, tender-point injections, and occupational therapy.
Evidence-strength note: This design can support a useful clinical observation: pregabalin was tolerated and improvement followed its use in 3 adult type I CRPS cases. It cannot show that pregabalin caused the improvement, identify the best dose, separate pregabalin from injections and rehabilitation, or prove superiority over gabapentin, duloxetine, bisphosphonates, sympathetic blocks, ketamine, or structured rehabilitation.
CRPS Is More Than Standard Neuropathic Pain
CRPS overlaps with neuropathic pain while adding limb-level autonomic, inflammatory, motor, and body-perception features. The syndrome can include allodynia (pain from normally harmless touch), hyperalgesia (exaggerated pain from painful input), edema, sweating changes, skin-temperature changes, color changes, weakness, tremor, dystonia, stiffness, nail or skin changes, and reduced limb ownership.
Mechanistically, several systems can be active at the same time:
- Neurogenic inflammation: C-fibers can release substance P and calcitonin gene-related peptide (CGRP), which may amplify local swelling, vasomotor change, and pain sensitivity.4
- Central sensitization: Spinal and brain pain circuits can become over-responsive, so pain spreads beyond the initial injury area or persists after tissue healing.5
- Autonomic dysregulation: sympathetic and vascular control can become unstable, producing temperature, sweating, and color asymmetry.
- Psychological load: anxiety, depression, catastrophizing, body-perception disturbance, and avoidance can worsen disability while also arising from persistent severe pain.
Pregabalin’s calcium-channel mechanism could plausibly reduce excitatory neurotransmitter release and dampen neuropathic pain signaling. The case-series authors also discussed possible effects on substance P and CGRP-linked pathways, but the study did not measure inflammatory markers, CGRP, substance P, serum pregabalin levels, or central sensitization.
Broader Pregabalin Evidence Supports Neuropathic Pain, Not CRPS Proof
The strongest reason to take pregabalin seriously in CRPS is not this 3-person series by itself. It is the broader neuropathic-pain literature, where pregabalin has randomized-trial evidence across conditions such as postherpetic neuralgia, diabetic painful neuropathy, and other neuropathic-pain states.
Finnerup et al.’s 2015 systematic review and meta-analysis reported moderate-certainty support for pregabalin in neuropathic pain, with an NNT of 7.7 (95% CI 6.5-9.4). NNT means number needed to treat: roughly how many patients must receive a treatment for 1 additional patient to achieve a defined benefit compared with control.3
Mayoral et al.’s 2024 systematic review comparing pregabalin with gabapentin also favored pregabalin across multiple neuropathic-pain outcomes, including pain scores, quality-of-life measures, and opioid requirements. Pharmacokinetic differences give a plausible explanation: pregabalin has more predictable absorption and dose-response behavior than gabapentin.6
Those findings still require a CRPS-specific discount. A drug can work for diabetic neuropathy or postherpetic neuralgia and still have uncertain value in CRPS, where inflammation, autonomic instability, movement avoidance, altered body perception, and rehabilitation timing can dominate the clinical course.
CRPS Reviews Keep the Treatment Bar High
Ferraro et al.’s 2023 Cochrane overview is the calibration point: adult CRPS trials remain too sparse, heterogeneous, and low-certainty to justify confident drug rankings. The review did not create a clean medication hierarchy where pregabalin clearly belongs at the top.2
A 2024 Lancet Neurology review reached the same practical destination from a broader clinical angle: CRPS needs careful diagnosis, early functional restoration, pain control, psychological support when needed, and staged escalation rather than a single medication algorithm.7
For pregabalin, the most reasonable current interpretation is narrow:
- Reasonable role: a neuropathic-pain medication to consider when allodynia, burning pain, sleep disruption, or rehabilitation-blocking pain are prominent.
- Weak claim: pregabalin as a proven first-line CRPS therapy based on 3 uncontrolled adult cases.
- Best research test: a randomized trial comparing pregabalin with gabapentin, placebo, or standardized multimodal care, with pain, function, sleep, mood, edema, limb use, and adverse events measured prospectively.
What Patients and Clinicians Should Take From the 2026 Series
The case series is most useful as a rehabilitation signal. In all 3 cases, pain reduction was linked to better participation in physical or occupational therapy, improved activities of daily living, ambulation, or sleep. In CRPS, that functional bridge may matter more than a pain score in isolation, because disuse and guarded movement can help maintain disability.
Practical implication: pregabalin should be judged by whether it helps the patient move, sleep, tolerate desensitization, and participate in graded limb use without unacceptable dizziness, sedation, edema, cognitive slowing, or misuse risk.
Research implication: future CRPS studies should measure functional endpoints alongside VAS pain. A treatment that reduces pain by 2-4 points but fails to improve hand use, gait, sleep, or therapy participation would be less compelling than one that changes the whole rehabilitation trajectory.
Questions About Pregabalin for CRPS
Does this case series prove pregabalin works for CRPS?
No. A 3-person uncontrolled case series cannot prove efficacy. It shows that all 3 adults improved after pregabalin was added, but the cases also included rehabilitation, injections, NSAIDs, opioids, baclofen, botulinum toxin, or procedures depending on the patient.
Why is pregabalin biologically plausible for CRPS?
Pregabalin reduces calcium-channel-linked neurotransmitter release in pain pathways. That could matter in CRPS when allodynia, burning pain, central sensitization, sleep disruption, and rehabilitation-blocking pain are prominent.
Why not treat CRPS like any other neuropathic pain condition?
CRPS includes neuropathic pain features, but it can also include swelling, sweating changes, temperature asymmetry, movement problems, tissue changes, altered limb ownership, anxiety, and depression. Those features make multimodal care more important than a drug-only plan.
What would make the pregabalin claim stronger?
A randomized trial with standardized CRPS diagnosis, clear pregabalin dosing, a control group, blinded outcome assessment, functional endpoints, adverse-event tracking, and follow-up long enough to see whether pain relief changes rehabilitation and relapse risk.
References
- Chang W-Y, Chang C-C, Wu Y-T, Li T-Y. Clinical outcomes of pregabalin therapy in adults with type I complex regional pain syndrome: a case series. Journal of Pain Research. 2026;19:591680. doi:10.2147/JPR.S591680
- Ferraro MC, Cashin AG, Wand BM, et al. Interventions for treating pain and disability in adults with complex regional pain syndrome: an overview of systematic reviews. Cochrane Database of Systematic Reviews. 2023;6:CD009416. doi:10.1002/14651858.CD009416.pub3
- Finnerup NB, Attal N, Haroutounian S, et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Lancet Neurology. 2015;14(2):162-173. doi:10.1016/S1474-4422(14)70251-0
- Littlejohn G. Neurogenic neuroinflammation in fibromyalgia and complex regional pain syndrome. Nature Reviews Rheumatology. 2015;11(11):639-648. doi:10.1038/nrrheum.2015.100
- Nijs J, George SZ, Clauw DJ, et al. Central sensitisation in chronic pain conditions: latest discoveries and their potential for precision medicine. Lancet Rheumatology. 2021;3(5):e383-e392. doi:10.1016/S2665-9913(21)00032-1
- Mayoral V, Galvez R, Ferrandiz M, et al. Pregabalin vs. gabapentin in the treatment of neuropathic pain: a comprehensive systematic review and meta-analysis of effectiveness and safety. Frontiers in Pain Research. 2024;5:1513597. doi:10.3389/fpain.2024.1513597
- Ferraro MC, O’Connell NE, Sommer C, et al. Complex regional pain syndrome: advances in epidemiology, pathophysiology, diagnosis, and treatment. Lancet Neurology. 2024;23(5):522-533. doi:10.1016/S1474-4422(24)00076-0