A 16-patient pilot study after facial reanimation surgery found that online emotional training and in-person emotional training both reduced anxiety and improved facial movement; FDI physical function changed by 21.25 points in the in-person group vs. 7.5 points in the online group.1
Research Highlights
- Small pilot, real recovery signal: Guidetti et al. followed 16 adults after triple innervation surgery, with 8 receiving in-person emotional training and 8 receiving the same protocol online for 10 sessions over 20 weeks.1
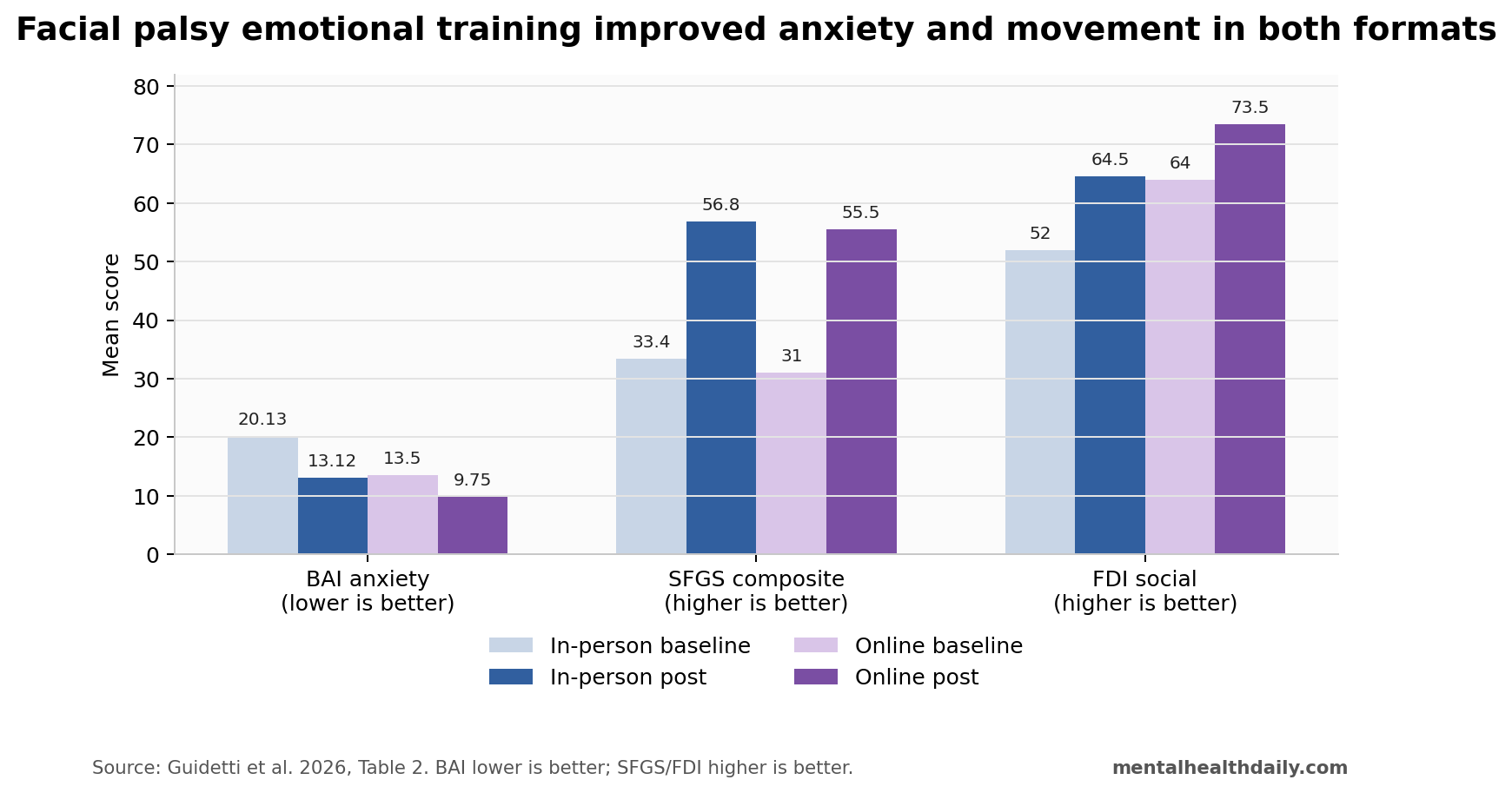
- Anxiety decreased in both formats: Beck Anxiety Inventory scores fell from 20.13 to 13.12 in the in-person group and from 13.5 to 9.75 in the online group, with a time effect of p = 0.002.1
- Facial movement improved strongly: Sunnybrook Facial Grading System composite scores rose from 33.4 to 56.8 in-person and from 31.0 to 55.5 online, with a time effect of p < .001 and no format split.1
- Physical function favored hands-on care: the only significant time x treatment interaction was FDI physical function (F1=14.356; p = 0.002), where in-person care improved more than online care.1
- Evidence remains preliminary: there were 0 dropouts, but the study was nonrandomized, assessor-blinded only by treatment group, and limited to post-surgical facial palsy after triple innervation.1
Facial nerve palsy means weakness or paralysis of the muscles on 1 side of the face. The disability reaches eye closure, speech, eating, smiling, social signaling, and self-confidence.
Emotional training is a rehabilitation approach that links facial movement practice to sensory attention, emotional expression, and daily functions such as smiling, blinking, speaking, and drinking. In this study, the online version was not a home exercise handout; a physiotherapist supervised each video session live.
Online Emotional Training Matched In-Person Care on Most Outcomes
Guidetti et al. enrolled 16 adults with unilateral peripheral facial nerve palsy after triple innervation surgery, a facial reanimation operation that uses masseteric, hypoglossal, and contralateral facial-nerve inputs to support voluntary movement, muscle tone, and spontaneous expression.1
The 2 rehabilitation formats had the same schedule: 1 session every 2 weeks, 10 sessions total, across 20 weeks. Each session lasted about 50 minutes and used the same progression from sensory awareness to emotional expression to functional facial tasks.
Participants were not randomized. People entered online or in-person care based on whether they could attend the hospital. That design fits real-world access, but it also means the groups may differ in ways that a 16-person table cannot fully detect.
The main readout is still clear enough to be useful: anxiety, facial symmetry, voluntary movement, and facial social well-being improved over time in both formats, while the treatment-format interaction was mostly nonsignificant.
Beck Anxiety Scores Fell Despite No Talk-Therapy Component
Beck Anxiety Inventory (BAI) is a 21-item symptom scale scored from 0 to 63, where higher scores mean more anxiety symptoms. The in-person group moved from a mean BAI score of 20.13 to 13.12. The online group moved from 13.5 to 9.75. The overall time effect was significant (p = 0.002), while the time x treatment interaction was not (p = 0.27).1
That matters because facial palsy often produces social anxiety through a direct route: the face no longer communicates reliably. Hotton et al. reviewed the psychosocial impact of facial palsy and found consistent effects on social interaction, emotional distress, appearance-related concern, and quality of life.3
Emotional training plausibly acts on anxiety through several paths at once:
- Motor control: better facial movement can reduce fear that expressions will look distorted.
- Expression practice: repeatedly practicing smiles, eye closure, and emotion-linked movements may lower avoidance.
- Therapist feedback: live correction can make the patient less dependent on self-monitoring.
- Social function: exercises target communication along with isolated muscle contraction.
None of those mechanisms proves the anxiety change was caused by the emotional content of the protocol. Anxiety might also improve because patients are recovering over time after surgery. But the finding is clinically coherent: facial rehabilitation that restores social signaling can plausibly reduce anxiety even when the program is not conventional psychotherapy.
Sunnybrook Composite Scores Improved by About 24 Points
Sunnybrook Facial Grading System (SFGS) scores facial resting symmetry, voluntary movement, and synkinesis, then combines them into a 0-100 composite score. Higher composite scores mean better facial function.
In the Guidetti pilot, SFGS composite scores rose from 33.4 to 56.8 in the in-person group and from 31.0 to 55.5 in the online group. The time effect was strong (F1=111.430; p < .001), and the format interaction was not significant (p = 0.81).1
The modified SFGS with bilateral masseter contraction also improved: composite scores increased from 48.5 to 65.9 in-person and from 46.1 to 67.9 online. That measure is specific to the surgery logic because patients initially activate facial movement through masseter engagement.
Clinical implication: the online format seemed adequate for supervised movement practice, emotional-expression retraining, and feedback-driven progression. It did not obviously collapse into unsupported self-exercise.
FDI Physical Function Was the One Clear In-Person Advantage
Facial Disability Index (FDI) is a self-report measure with physical and social/well-being components. The social and well-being subscale improved in both groups, from 52.0 to 64.5 in-person and 64.0 to 73.5 online, with a significant time effect (p < .001) and no treatment interaction (p = 0.45).1
Physical function separated more. Scores improved from 45.0 to 66.25 in the in-person group and from 62.5 to 70.0 in the online group. The time x treatment interaction was significant (F1=14.356; p = 0.002), and post hoc testing identified a larger in-person change.1
That finding should not be flattened into “online and in-person are identical.” The better interpretation is narrower: online emotional training looked feasible and broadly comparable for most outcomes, but hands-on care may still add something for physical facial function, especially where tissue flexibility, massage, stretching, and tactile correction are important.
Digital Facial Palsy Care Already Had Feasibility Signals
The 2026 pilot fits a broader shift toward remote neurological rehabilitation. Federico et al. reviewed telerehabilitation for neurological motor impairment and found support for quality of life, satisfaction, and acceptance across stroke, multiple sclerosis, and Parkinson’s disease populations.2
Facial palsy has a separate digital-care literature. Szczepura et al. surveyed patients and clinicians about changing UK facial palsy treatment pathways and reported interest in digital technology, but also a need for careful pathway design rather than a simple replacement of specialist care.4
Tan et al. compared face-to-face and video assessment of facial paralysis and framed the measurement issue directly: remote care only works if clinicians can judge facial movement accurately enough through video.5 That is why the Guidetti protocol’s live supervised sessions matter. The treatment was remote, but it still preserved observation, feedback, correction, and adherence monitoring.
Facial Exercise Evidence Supports Rehab, Not One Best Protocol
Khan et al. updated the evidence for physical therapy and facial exercise therapy in facial nerve paralysis and found support for facial exercise approaches, while the literature still varied by cause, timing, severity, outcome measure, and intervention type.6
Shi et al. reviewed pharmacological and physical therapies for Bell’s palsy using a Bayesian network meta-analysis, underscoring the same practical issue: physical therapy can be useful, but the field does not have a single universally superior protocol that fits every facial palsy phenotype.7
The Guidetti study is even narrower than Bell’s palsy. These participants had post-surgical facial palsy after triple innervation, so the motor learning problem included masseter-assisted movement and gradual dissociation from jaw clenching. That makes the intervention highly relevant to surgical facial reanimation, but less directly portable to idiopathic Bell’s palsy or acute viral facial palsy.
Evidence Strength: Feasible, Promising, Not Equivalent Yet
This was an assessor-blinded pilot cohort study, not an equivalence trial. A real equivalence claim would need random assignment, prespecified noninferiority margins, larger sample size, and enough power to rule out clinically meaningful differences between formats.
The best current read has 3 parts:
- Online delivery is feasible: the study reported 0 dropouts and completed live supervised telerehabilitation in a rare post-surgical population.
- Most outcomes moved similarly: facial movement, anxiety, and social/well-being function improved over time without a clear online-vs-in-person split.
- Hands-on care may still matter: physical FDI improvement favored in-person treatment, which fits the tactile and manual components of facial rehabilitation.
For patients who cannot easily attend specialty facial palsy rehabilitation, online emotional training may be a serious access tool. For patients with substantial physical dysfunction, tissue tightness, or need for manual therapy, in-person care still has a plausible advantage.
Questions About Facial Palsy Telerehabilitation
Did online facial palsy rehabilitation work as well as in-person treatment?
Mostly, but the word “work” needs endpoint-specific wording. Anxiety, facial movement, and social/well-being scores improved over time in both groups, with no significant format interaction. Physical facial-disability scores improved more in the in-person group.
Was this a randomized trial?
No. The study was prospective and assessor-blinded, but treatment format was assigned according to whether participants could attend in-person sessions. That makes the results useful for feasibility and signal detection, not proof of equivalence.
Who do these findings apply to?
The clearest fit is adults with unilateral facial palsy after triple innervation surgery. The results should not be generalized automatically to all Bell’s palsy, acute facial palsy, or non-surgical facial nerve injuries.
Why would facial movement training reduce anxiety?
Facial palsy changes social communication. Better movement control, less fear of distorted expression, therapist feedback, and repeated practice of emotional expressions can all plausibly lower anxiety around speaking, smiling, and being seen.
Should remote care replace in-person facial palsy therapy?
No. Remote emotional training looks like a credible access option when specialist attendance is difficult. In-person care may still be preferable when manual therapy, direct tactile feedback, or more severe physical impairment is central.
References
- Guidetti M, Cupello S, Reali J, et al. Emotional Training via Telerehabilitation After Surgical Treatment for Facial Palsy: Prospective, Assessor-Blinded, 2-Arm Pilot Cohort Study. JMIR Rehabil Assist Technol. 2026;13:e79520. doi:10.2196/79520
- Federico S, Cacciante L, Cieslik B, et al. Telerehabilitation for neurological motor impairment: a systematic review and meta-analysis on quality of life, satisfaction, and acceptance in stroke, multiple sclerosis, and Parkinson’s disease. J Clin Med. 2024;13(1):299. doi:10.3390/jcm13010299
- Hotton M, Huggons E, Hamlet C, et al. The psychosocial impact of facial palsy: a systematic review. Br J Health Psychol. 2020;25(3):695-727. doi:10.1111/bjhp.12440
- Szczepura A, Holliday N, Neville C, et al. Raising the digital profile of facial palsy: national surveys of patients’ and clinicians’ experiences of changing UK treatment pathways and views on the future role of digital technology. J Med Internet Res. 2020;22(10):e20406. doi:10.2196/20406
- Tan JR, Coulson S, Keep M. Face-to-face versus video assessment of facial paralysis: implications for telemedicine. J Med Internet Res. 2019;21(4):e11109. doi:10.2196/11109
- Khan AJ, Szczepura A, Palmer S, et al. Physical therapy for facial nerve paralysis (Bell’s palsy): an updated and extended systematic review of the evidence for facial exercise therapy. Clin Rehabil. 2022;36(11):1424-1449. doi:10.1177/02692155221110727
- Shi J, Lu D, Chen H, et al. Efficacy and safety of pharmacological and physical therapies for Bell’s palsy: a Bayesian network meta-analysis. Front Neurol. 2022;13:868121. doi:10.3389/fneur.2022.868121