A 2026 single-arm Survivors RESET study enrolled 20 Black female breast cancer survivors with obesity and elevated stress, then met its enrollment, retention, and adherence feasibility benchmarks while missing its stricter satisfaction benchmark by 5 percentage points.1 Weight fell by 2.4 kg and perceived stress fell by 6.9 PSS-10 points over 4 months, but without a control group those changes are best read as a signal for a full randomized trial.
Research Highlights
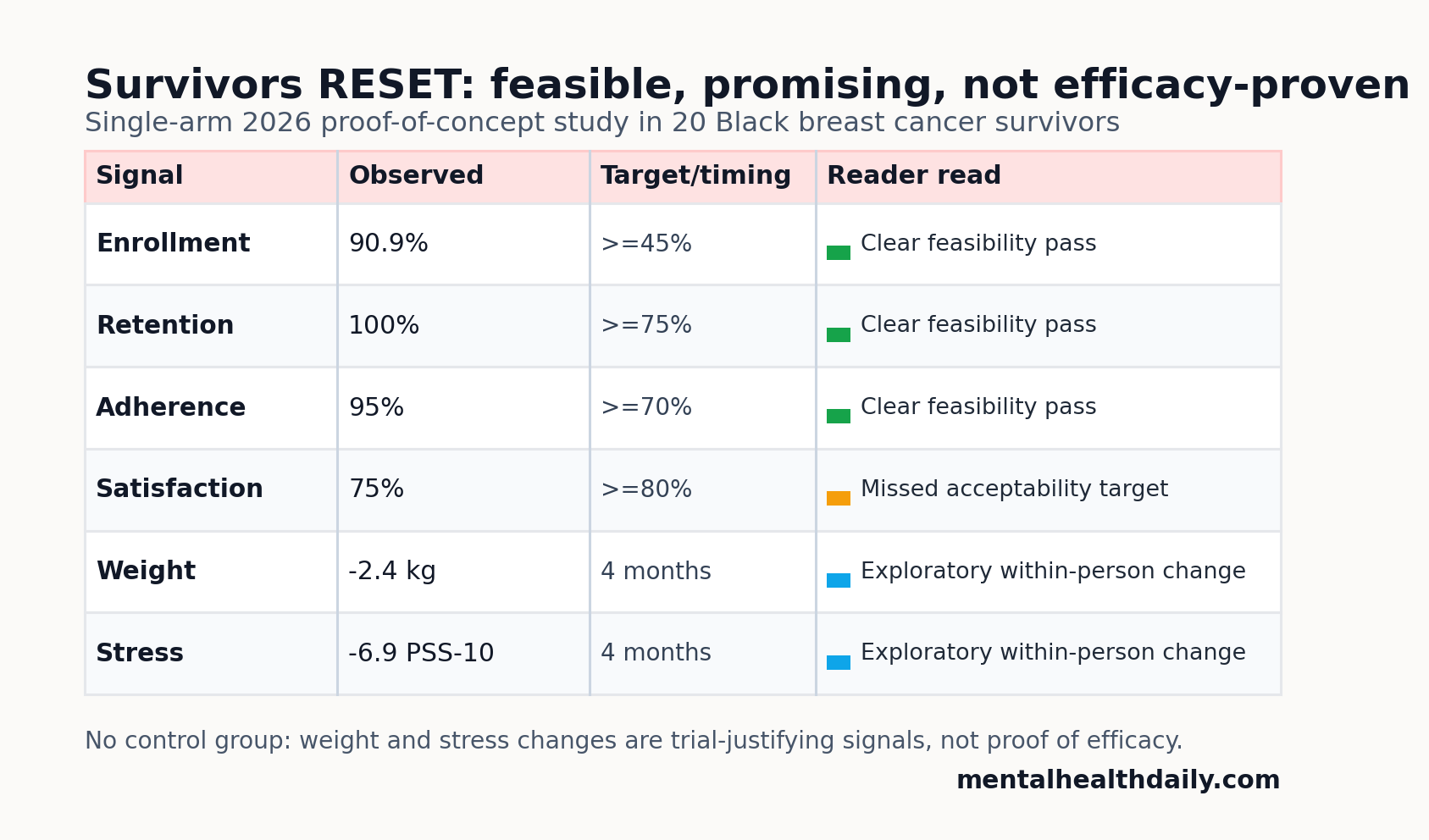
- Enrollment was strong: 20 of 22 eligible women enrolled, or 90.9%, exceeding the pre-set 45% feasibility benchmark.1
- Retention and adherence cleared the bar: 100% completed baseline and 4-month assessments, and 95% attended at least 70% of the 16 weekly sessions.1
- Satisfaction was the weak feasibility signal: 75% were somewhat or very satisfied, below the 80% acceptability benchmark, although 95% said they would recommend the program.1
- Exploratory outcomes moved in the intended direction: mean weight decreased by 2.4 kg, BMI decreased by 0.9 kg/m2, and PSS-10 perceived stress decreased by 6.9 points over 4 months.1
- Stress relief did not explain weight change: change in PSS-10 and change in weight were not significantly correlated, r = 0.25, p = 0.279, so the stress-management mechanism remains unproven.1
Survivors RESET is a culturally tailored behavioral weight-loss program adapted from the Diabetes Prevention Program and enhanced with stress-management and breast-cancer survivorship content. The tested version delivered 16 weekly online group sessions led by a trained Black female interventionist, with diet, activity, self-monitoring, relaxation, action planning, time management, cognitive stress skills, and cancer-relevant activity barriers all built into the curriculum.1
Perceived stress means the person’s own rating of how unpredictable, overloaded, or uncontrollable life has felt recently. Rodrigues et al. used the 10-item Perceived Stress Scale (PSS-10), where scores range from 0 to 40 and higher scores mean more perceived stress.
Enrollment, Retention, and Attendance Beat Feasibility Benchmarks
Rodrigues et al. recruited Black female breast cancer survivors from Moffitt Cancer Center survivorship care and Tampa Bay community channels.1 Eligibility required prior stage 0-3 breast cancer treated with curative intent, body mass index at or above 30 kg/m2, and moderate-to-high PSS-10 stress.
The feasibility results were unusually clean for a small behavioral intervention:
- Enrollment: 20 of 22 eligible survivors enrolled, or 90.9%, against a 45% benchmark.
- Retention: 20 of 20 completed both baseline and 4-month assessments, against a 75% benchmark.
- Adherence: 19 of 20 attended at least 70% of the 16 sessions, with mean attendance of 13.55 sessions.
Those numbers do not prove clinical effectiveness. They do answer a necessary earlier question: this population could be recruited, retained, and kept engaged through the intensive weekly phase of an online lifestyle-and-stress program.
Satisfaction Fell Just Short of the 80% Acceptability Target
Acceptability was more mixed than the enrollment and attendance data. Fifteen of 20 participants, or 75%, were somewhat or very satisfied with the overall weight-management program. The study’s benchmark was 80%, so satisfaction fell slightly short.
Recommendation looked better: 19 of 20 participants, or 95%, said they probably or definitely would recommend the program. That split is important. Participants may have valued the program enough to recommend it while still seeing burdens, fit problems, or parts of the experience that need refinement.
Treatment burden means the work a person must do to follow the intervention. The adapted burden questionnaire was generally low, with a mean score of 29.1 on a 0-70 scale among 18 participants with complete data. Low-burden ratings were most common for session frequency, session time, dietary changes, physical-activity recommendations, and relationship effects. Food and activity self-monitoring plus financial burden produced more mixed responses.
Weight and Stress Improved, But the Design Cannot Prove Efficacy
Over 4 months, mean weight decreased from 97.8 kg to 95.5 kg, a mean change of −2.4 kg, p = 0.006. Mean BMI decreased from 37.1 to 36.2 kg/m2, with a mean change of −0.9 kg/m2. Mean PSS-10 decreased from 21.4 to 14.6, a mean change of −6.9 points, p = 0.003.1
75% of participants lost weight. Among those who lost weight, mean loss was 3.7 kg. 40% lost at least 3% of baseline weight, and 10% lost at least 5%.
Evidence-strength note: these were within-person changes in a single-arm proof-of-concept study. The design cannot separate the intervention from expectancy effects, regression to the mean, measurement timing, outside behavior change, or survivorship-clinic selection. It also cannot tell whether the stress-management content added benefit beyond standard behavioral weight-loss counseling.
Mechanism remained unresolved: baseline PSS-10 and baseline weight were unrelated, r = 0.00, p = 0.996. Change in stress and change in weight were also not significantly correlated, r = 0.25, p = 0.279.
Stress may still affect adherence, sleep, eating patterns, or energy regulation, but this study did not show that stress reduction mediated weight loss.
Stress-Management Augmentation Has Prior Support, Not Proof
The rationale for adding stress skills is biologically and behaviorally plausible. Chronic stress can push eating toward high-reward foods, worsen sleep, reduce activity, raise emotional exhaustion, and make self-monitoring harder. Black women also report high chronic stress exposure in many US health datasets, and breast cancer survivorship can add fatigue, neuropathy, body-image concerns, fear of recurrence, and care-burden pressure.
Cox et al. previously tested a stress-management-augmented behavioral weight-loss intervention in African American women with overweight or obesity.2 That pilot found perceived-stress reductions of −6.5 points in the lifestyle-only group and −5.3 points in the lifestyle plus stress-management group, without a significant between-group advantage for the stress-management addition.
Rodrigues et al. therefore extend the feasibility question into breast cancer survivorship, but they do not settle the additive-treatment question. A future trial needs a comparator that can separate:
- Standard behavioral weight loss: calorie reduction, activity targets, self-monitoring, and group support.
- Cultural and survivorship tailoring: racial concordance, relevant imagery, spirituality/community/pride framing, fatigue and neuropathy adaptations, and cancer-risk messaging.
- Stress-management content: relaxation practice, cognitive stress skills, time management, and action planning.
Without those comparisons, the strongest conclusion is narrower: Survivors RESET looks deliverable and worth testing, not already proven superior to DPP-style weight management.
Behavioral Weight-Loss Comparators Keep the Result in Scale
Rodrigues et al. compared their 4-month weight reduction with prior adaptations of the Diabetes Prevention Program and community weight-loss trials.
Closest weight-loss scale: Kitzman et al. reported an average 2.3 kg reduction over 4 months in a faith-based diabetes-prevention program for African American women, close to the 2.4 kg reduction in Survivors RESET.4 Katula et al. tested a digital Diabetes Prevention Program in adults with prediabetes and provides a delivery-mode comparator outside cancer survivorship.5
Ard et al. studied a community-based randomized trial in rural African American women and reported weight loss plus metabolic improvements over 6 months.3 Rodrigues et al. note that 75% of their participants lost weight after 4 months, higher than the 57.1% reported after 6 months in that rural trial and broadly comparable to the church-based intervention.
The comparison supports feasibility, not triumphalism. A 2.4 kg mean reduction can be meaningful in survivorship care, especially if paired with lower stress and better function, but it is still an early-phase signal. Breast cancer recurrence, metabolic risk, quality of life, fatigue, depression, and long-term maintenance require longer randomized follow-up.
What a Full Survivors RESET Trial Needs to Show
A serious next trial should retain the strengths of this pilot: targeted recruitment, culturally relevant delivery, strong attendance tracking, and survivorship-specific content. It should also pressure-test the pieces that a single-arm pilot cannot answer.
- Comparator: standard DPP-style behavioral weight loss, attention control, or another credible active intervention.
- Duration: the full 26-session curriculum, including the maintenance phase that follows the 16-session intensive phase.
- Outcomes: weight, waist circumference, metabolic markers, PSS-10, fatigue, quality of life, depression/anxiety symptoms, and physical function.
- Mechanism: whether stress reduction predicts adherence, self-monitoring, sleep, eating behavior, activity, or later weight maintenance.
- Reach: lower-income survivors, rural survivors, patients with more treatment toxicity, and people with less flexible schedules.
That design would let the intervention succeed or fail on the right terms. The current paper says the program can be run and that early signals point in the intended direction. It does not yet say the stress-management layer is the active ingredient.
Questions About Survivors RESET and Stress-Managed Weight Loss
Does this prove stress management caused weight loss?
No. The study had no control group, and stress reduction was not significantly correlated with weight change. Stress management may still help adherence or quality of life, but this pilot did not prove mediation.
Was the intervention acceptable?
Partly. Retention, attendance, and recommendation were strong, but satisfaction reached 75% and missed the pre-set 80% acceptability benchmark.
Why focus specifically on Black breast cancer survivors?
Black women experience persistent breast-cancer survivorship disparities and are underrepresented in many behavioral intervention trials. A tailored feasibility study tests whether recruitment, delivery, and engagement work before a larger efficacy trial.
What would make this clinically persuasive?
A randomized trial showing better weight, stress, function, or survivorship outcomes than a credible comparator, with benefits maintained after the intensive weekly phase, would move Survivors RESET from promising pilot to clinically stronger evidence.
References
- Rodrigues APS, Cooper AJ, Llanos AAM, Fleming K, Pittman S, Pena A, Henderson J, Mallory M, Sutton SK, Jim HSL, Stern M, Carson TL. Feasibility and acceptability of a stress-management behavioral weight loss intervention for Black breast cancer survivors. Scientific Reports. 2026. doi:10.1038/s41598-026-49330-4
- Cox TL, Krukowski R, Love SRJ, Eddings K, DiCarlo M, Chang JY, Prewitt TE, West DS. Stress management-augmented behavioral weight loss intervention for African American women: a pilot, randomized controlled trial. Health Education and Behavior. 2013;40:78-87. doi:10.1177/1090198112439411
- Ard JD, Carson TL, Shikany JM, Li Y, Hardy CM, Robinson JC, Williams AG, Baskin ML. Weight loss and improved metabolic outcomes amongst rural African American women in the Deep South: six-month outcomes from a community-based randomized trial. Journal of Internal Medicine. 2017;282:102-113. doi:10.1111/joim.12622
- Kitzman H, Mamun A, Dodgen L, Slater D, King G, King A, Slater JL, DeHaven M. Better Me Within randomized trial: faith-based diabetes prevention program for weight loss in African American women. American Journal of Health Promotion. 2021;35:202-213. doi:10.1177/0890117120958545
- Katula JA, Dressler EV, Kittel CA, Harvin LN, Almeida FA, Wilson KE, Michaud TL, Porter GC, Brito FA, Goessl CL, Jasik CB, Sweet CMC, Schwab R, Estabrooks PA. Effects of a digital Diabetes Prevention Program: an RCT. American Journal of Preventive Medicine. 2022;62:567-577. doi:10.1016/j.amepre.2021.10.023
- Carson TL, Llanos AAM, Fleming K, Pittman S, Pena A, Henderson J, Doerr V, Cooper AJ, Mallory M, Sutton S, Jim HSL. Rationale and study protocol for a pilot study to determine the feasibility and acceptability of a tailored stress management enhanced behavioral weight loss intervention for Black breast cancer survivors with obesity. Contemporary Clinical Trials. 2025;159:108113. doi:10.1016/j.cct.2025.108113
- Jiralerspong S, Goodwin PJ. Obesity and breast cancer prognosis: evidence, challenges, and opportunities. Journal of Clinical Oncology. 2016;34:4203-4216. doi:10.1200/JCO.2016.68.4480