
A 430-caregiver study in Kathmandu found caregiving burden in 65.3% of family caregivers of older adults with disability, with adjusted predictors clustering around low economic status, 8 or more daily care hours, and severe impairment in activities of daily living.1
Research Highlights
- Burden was the majority experience: 65.3% of 430 family caregivers reported caregiving burden while caring for older adults with disability in Kathmandu.1
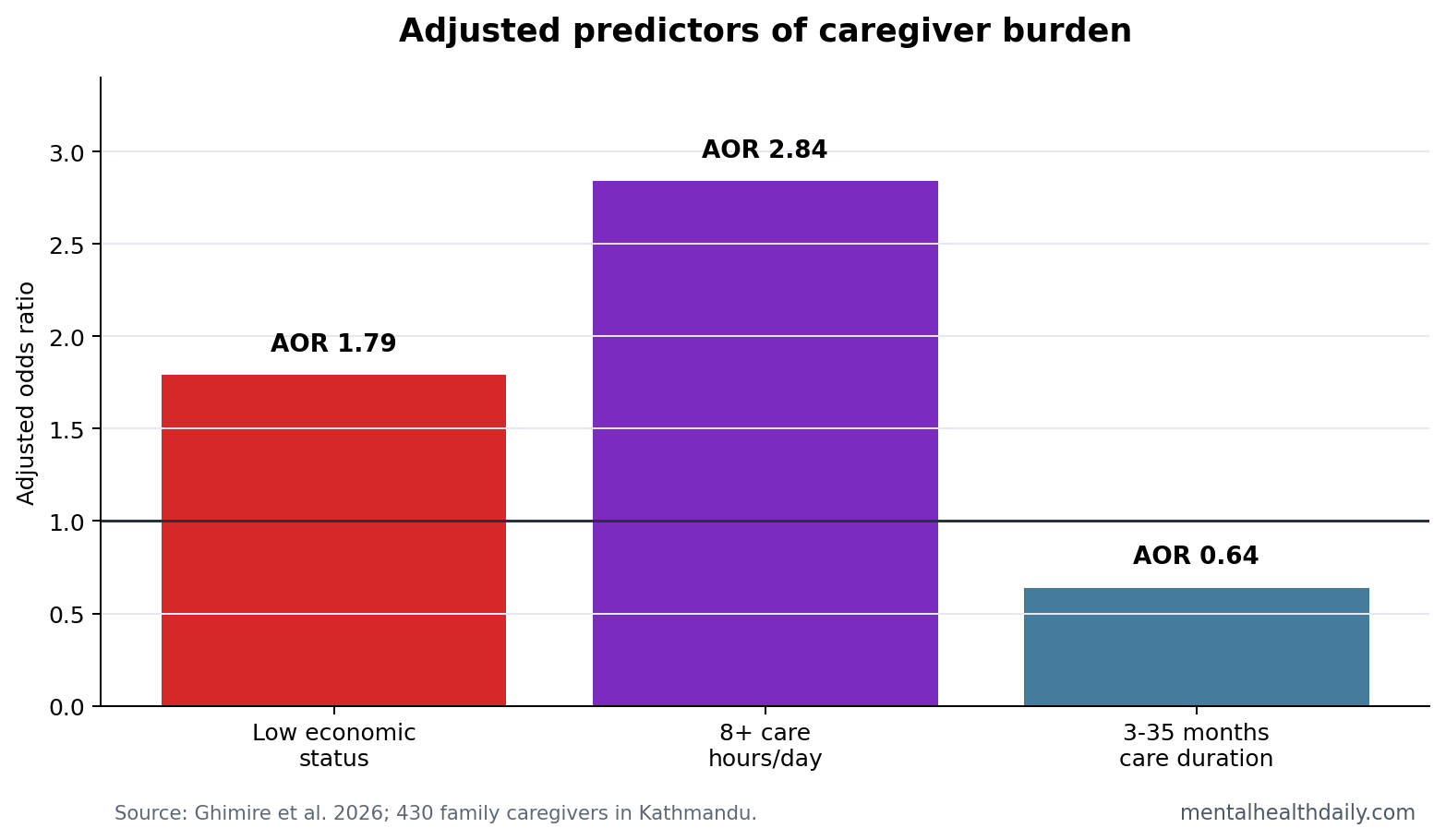
- Time demand was the strongest adjusted signal: providing care for 8 or more hours daily was associated with higher burden odds (AOR 2.84; 95% CI 1.14 to 7.06; p = .025).1
- Money pressure remained visible: low economic status predicted burden after adjustment (AOR 1.79; 95% CI 1.05 to 3.05; p = .031).1
- Disability severity mattered: 12.3% of older adults had complete ADL impairment, and ADL status stayed in the adjusted predictor set.1
- Stress and sleep were part of the burden picture: 58.6% of caregivers reported extra stress and 37.7% reported disturbed nighttime sleep.1
Caregiver burden means the emotional, physical, financial, and time-load strain that comes from caring for another person. It is not the same as love, duty, or family involvement. A caregiver can be committed and still be overloaded.
Activities of daily living (ADLs) are basic self-care tasks such as bathing, dressing, toileting, transferring, continence, and feeding. When an older adult loses ADL independence, family members often become the replacement care system.
Ghimire et al. studied that replacement system in Kathmandu, where formal long-term care support is limited for many families.1 The mental-health relevance is direct: high care hours, low money, sleep disruption, and perceived stress create the conditions under which depression, anxiety, irritability, and somatic strain accumulate.
65.3% of Family Caregivers Reported Burden
The study used structured interviews with 430 family caregivers from January to March 2022. Just over half of caregivers were aged 40 to 59 years, 83.5% were female, 43.0% had paid work, and 50.4% had income sufficient for 1 year or more.
The care context was intensive. Most caregivers had been caring for 3 years or more, and 19.5% provided 8 or more hours of care each day. Among older adults receiving care, 44.9% had impairment in 1 to 2 ADLs, 42.8% had impairment in 3 to 5 ADLs, and 12.3% had complete ADL impairment.
Reader-level translation: this was a high-load caregiving sample. Many caregivers were providing chronic hands-on support for older adults whose disability affected basic self-care. A 65.3% burden rate in that setting is a capacity signal and a psychological risk signal.
8 or More Daily Care Hours Carried the Clearest Adjusted Signal
The adjusted model found that caregivers providing 8 or more hours of care per day had 2.84 times the odds of burden compared with those providing 1 to 7 hours daily. That result is easy to understand clinically because time is the resource that disappears first.
High daily care hours compress sleep, paid work, errands, exercise, social contact, and private recovery time. They also make stress less episodic. The day itself becomes organized around another person’s disability.
Care duration had a more complicated pattern in the reported model: caring for 3 to 35 months had lower adjusted odds than caring for 36 months or more. The direction suggests chronicity may matter, but the more actionable result is the daily-hour load. A caregiver providing 8 or more hours today needs relief even if the caregiving role is relatively new.
Economic Status Turned Family Care Into a Mental-Health Risk
Low economic status predicted caregiver burden after adjustment. The model estimated an AOR of 1.79 for caregivers whose income was sufficient for less than 1 year compared with those with income sufficient for 1 year or more.
That money signal changes the interpretation of family care. In a high-support system, caregiving strain might be buffered by paid respite, transportation, assistive devices, home nursing, or paid leave. In a low-formal-support setting, the family absorbs more of the care labor and the financial uncertainty at the same time.
Clinical implication: stress-reduction training may help, but it cannot substitute for time and material support. Teaching relaxation to a caregiver who has no respite, poor sleep, and 8 daily care hours may reduce distress at the margin while leaving the central burden intact.
ADL Impairment Made the Care Work More Concrete
The study’s disability measure keeps the result grounded. ADL impairment is not an abstract severity score. It means the older adult needs help with basic tasks that have to happen repeatedly, privately, and often under time pressure.
Complete ADL impairment stayed in the adjusted predictor set. The reported direction in the article-in-press table requires cautious reading because the coding reference appears compressed in the extracted table text, but the study’s conclusion framed complete ADL impairment as part of the predictor profile for caregiver burden.1
That caveat matters because local policy should not treat any single odds ratio as the whole answer. Burden emerges from a bundle:
- Care intensity: 8 or more daily care hours leave little recovery time.
- Financial vulnerability: low economic status narrows options for paid help.
- Functional impairment: ADL limitations turn supervision into hands-on care.
- Sleep disruption: 37.7% reported disturbed nighttime sleep.
Cross-Sectional Data Support Triage, Not Causal Certainty
Evidence-strength note: this was a cross-sectional study using convenience sampling. It can identify caregivers who are more likely to report burden, but it cannot prove that low income, care hours, or ADL impairment caused burden in a strict causal sequence.
The direction is still useful. Caregiver-burden screening does not need to wait for perfect causal proof before asking about daily hours, sleep, economic stress, and ADL dependence. Those are concrete triage variables that can identify families who may need respite, cash support, skills training, or mental-health referral.
Caregiver-burden research going back to Zarit et al. treated burden as a measurable subjective strain rather than a vague family complaint.2 Later reviews and clinical overviews linked burden to care-recipient impairment, depression, stress, and caregiver health risk.3,4 The Nepal study adds setting-specific numbers for a low-formal-support care environment.
What the design can support: a risk screen. The study cannot prove that changing income, hours, or ADL support would reduce burden by a specific amount, but it can identify which families are already in the danger zone. In practice, that is enough to justify asking about caregiver sleep, mood, physical symptoms, paid-work disruption, and whether the caregiver has anyone who can take over for even a few hours.
What a Useful Caregiver Screen Should Ask First
The study points toward a short practical screen rather than a long psychological interview. A clinician, community worker, or social-service program can start with the variables that expose overload fastest: daily care hours, sleep disruption, income strain, ADL dependence, and whether the caregiver feels extra stress.
High-risk profile: a female middle-aged family caregiver providing 8 or more daily care hours, sleeping poorly, and caring for an older adult with multiple ADL impairments should be treated as a support-priority case even before a formal psychiatric diagnosis appears.
Intervention implication: monthly allowances, weekly respite, volunteer support, and stress-management education target different parts of the burden chain. Allowances reduce economic pressure. Respite returns time. Skills training may reduce helplessness. Mental-health referral becomes more useful when those practical supports are not ignored.
For MHD readers, the central mental-health point is that caregiver distress should be screened before collapse. Waiting until depression, family conflict, or medical neglect appears means the care system has already let the burden load become clinically visible.
A short burden screen also gives clinicians permission to ask about the caregiver as a patient-adjacent person with health risks and as the older adult’s helper. The shift is small but practical.
The screen should not stop at asking whether the caregiver feels stressed. It should ask what the day requires.
A caregiver who reports 8 or more hours of help, disturbed sleep, low economic reserve, and an older adult with several ADL impairments is describing a workload problem before describing a psychiatric label.1 That distinction keeps the response grounded: respite, money, transport, assistive devices, and skills support are mental-health interventions when the stressor is continuous care labor.
Caregiver-burden tools are most useful when they turn private strain into service eligibility. Without that step, screening can become another way to document distress while leaving the same family to absorb the next week of care alone.
Questions About Caregiver Burden in Older-Adult Disability Care
Does a high burden score mean the caregiver is unwilling?
No. Burden measures strain. A caregiver can be devoted, skilled, and morally committed while still being overloaded by time, money, sleep, and disability demands.
What is the most actionable screening question from this study?
Daily care hours are hard to ignore. A caregiver providing 8 or more hours of care each day should trigger a closer look at sleep, finances, respite access, and mental-health symptoms.
Can this study prove respite care would reduce burden?
No. It supports the logic for respite and support programs, but intervention trials are needed to estimate how much burden changes when support is added.
References
- Ghimire RDA, Tang S, Shrestha A. Factors associated with caregiving burden of family caregivers of older adults with disability, Kathmandu, Nepal. BMC Geriatrics. 2026. https://doi.org/10.1186/s12877-026-07506-7
- Zarit SH, Reever KE, Bach-Peterson J. Relatives of the impaired elderly: correlates of feelings of burden. The Gerontologist. 1980. https://doi.org/10.1093/geront/20.6.649
- Pinquart M, Sorensen S. Differences between caregivers and noncaregivers in psychological health and physical health: a meta-analysis. Psychology and Aging. 2003. https://doi.org/10.1037/0882-7974.18.2.250
- Adelman RD, Tmanova LL, Delgado D, Dion S, Lachs MS. Caregiver burden: a clinical review. JAMA. 2014. https://doi.org/10.1001/jama.2014.304