A 2026 study of Hodgkin lymphoma survivors treated with mantle radiation found obstructive sleep apnea (OSA) in 36 of 42 people who eventually underwent sleep testing. The practical screening target is a younger, non-obese, positional, hypopnea-heavy post-radiation OSA phenotype that standard risk heuristics can miss.1
Research Highlights
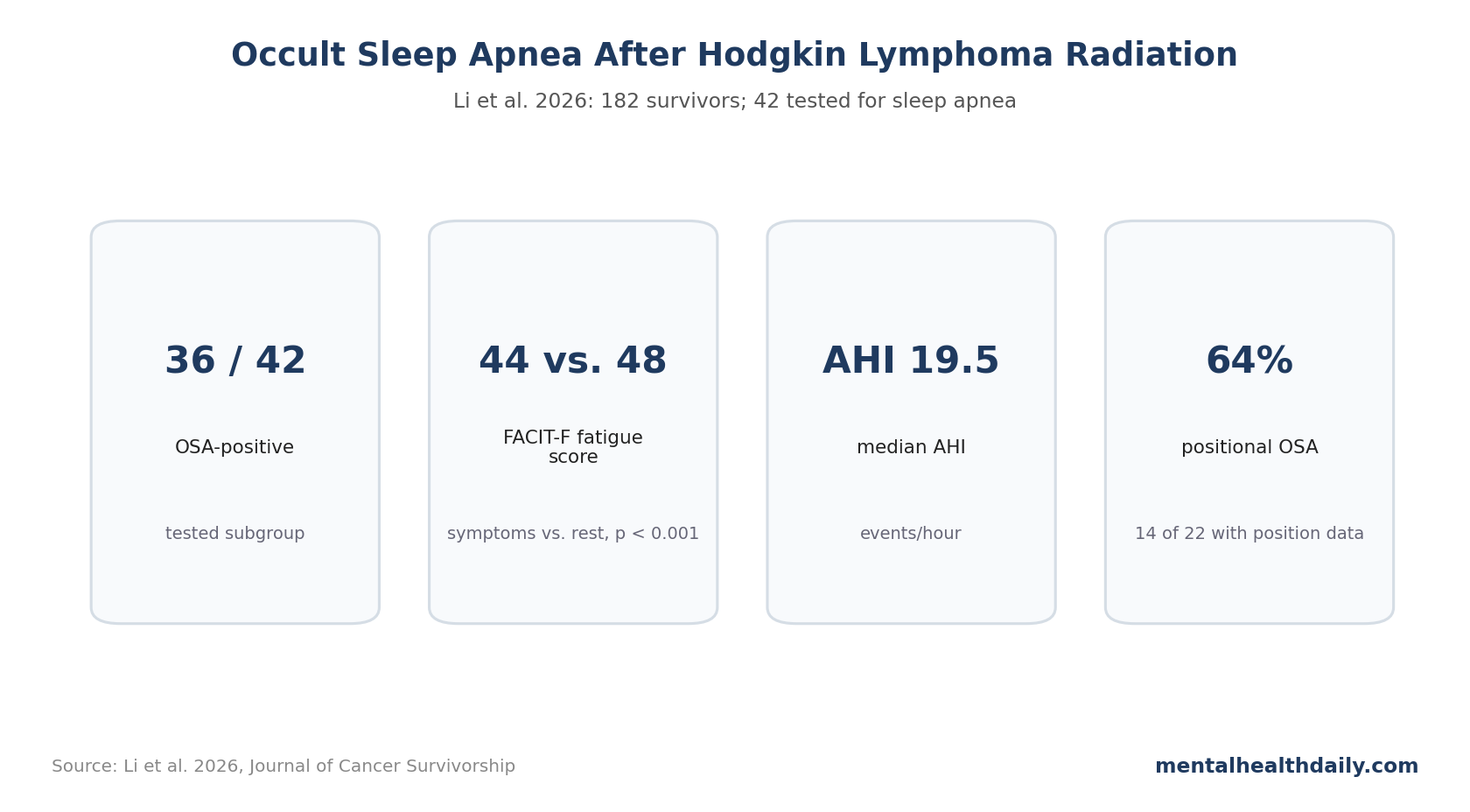
- Sleep symptoms identified a fatigued subgroup: 45 of 182 survivors had at least 2 sleep symptoms and lower FACIT-F fatigue scores than the rest of the cohort (44 vs. 48, p < 0.001).1
- OSA positivity was common among those tested: 21 of 25 prospectively tested survivors and 15 of 17 later chart-review cases were OSA-positive, totaling 36 of 42 tested people.1
- The phenotype was not classic obesity-driven OSA: median body mass index at sleep study was 27.5 kg/m2, and neck circumferences were smaller than usual high-risk thresholds.1
- Positional OSA was frequent: 14 of 22 patients with recorded supine/non-supine apnea-hypopnea index had positional OSA, defined as supine/non-supine AHI ratio >2.1
- Cardiac follow-up raised concern: OSA-positive survivors had higher adjusted heart-failure event rate than those without documented OSA (rate ratio 1.94, p = 0.007).1
Fatigue is common after Hodgkin lymphoma treatment, and it is easy to file it under cancer history, chemotherapy, radiation, endocrine disruption, mood, deconditioning, or aging. This paper adds a more specific possibility: sleep-disordered breathing after neck and chest radiation may be under-recognized.
182 Survivors Were Followed After Mantle Radiation
Li et al. studied 182 Hodgkin lymphoma survivors previously treated with mantle radiation therapy, meaning radiation that included the neck and chest region. The cohort came from 3 teaching hospitals and combined a prospective sleep-symptom protocol with later chart review.1
In the prospective phase, participants were interviewed about fatigue and sleep-related symptoms. They completed the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F), where lower score means greater fatigue.
The key screening path was simple:
- 182 survivors: all had prior mantle radiation.
- 45 with at least 2 sleep symptoms: this subgroup had lower median FACIT-F scores, 44 vs. 48.
- 25 attended in-lab polysomnography: 21 were OSA-positive.
- 17 more tested later in chart review: 15 were OSA-positive.
Polysomnography is the in-lab sleep test that records breathing, oxygenation, sleep stage, limb movement, and other physiology. OSA was diagnosed by sleep physicians using apnea-hypopnea index (AHI) >5 events per hour.
36 of 42 Tested Survivors Were OSA-Positive
Among the 42 survivors who underwent sleep testing, 36 were diagnosed with OSA. That is not the same as saying 36 of all 182 survivors definitely had OSA, because not everyone was tested. The denominator matters.
The more accurate statement is:
- Prospective testing: 21 of 25 tested people were OSA-positive.
- Later chart review: 15 of 17 tested people were OSA-positive.
- Total tested: 36 of 42 were OSA-positive.
- Untested symptomatic group: 15 of the original 45 symptom-positive survivors declined testing.
That last line cuts both ways. Some OSA cases may have been missed among people who declined testing, but the tested subgroup was not a random sample of all survivors. It was enriched for symptoms or clinical suspicion.
The study supports targeted suspicion, not a population-wide prevalence estimate. That distinction keeps the conclusion useful without inflating it.
Fatigue Plus Sleep Symptoms Was the Practical Entry Point
The symptom-positive group had median FACIT-F 44 compared with 48 in the rest of the cohort, p < 0.001. The difference is not enormous, but it tells clinicians where to look: survivors reporting multiple sleep symptoms were also more fatigued.1
FACIT-F is a patient-reported fatigue scale used frequently in chronic illness and cancer survivorship. It cannot diagnose OSA, but it can capture the fatigue burden that makes sleep testing clinically relevant.
OSA is especially plausible when fatigue travels with symptoms such as snoring, witnessed apneas, non-restorative sleep, morning headaches, nocturnal choking, fragmented sleep, or daytime sleepiness. But this cohort also warns against relying only on classic sleepiness: the Epworth Sleepiness Scale median among OSA-positive patients was 6 out of 24, which is not strikingly high.
That is common in sleep medicine. Some people with clinically important OSA are not dramatically sleepy. They may present with fatigue, insomnia, blood pressure problems, atrial fibrillation, mood symptoms, nocturia, or nonspecific “I never feel restored” complaints.
Non-Obese, Positional, Hypopnea-Heavy OSA Is Easy to Miss
The OSA-positive Hodgkin survivors did not look like the highest-risk OSA stereotype. Median body mass index at sleep study was 27.5 kg/m2, which is overweight but not severe obesity. Median neck circumference was 30 cm in women and 38 cm in men, smaller than usual high-risk thresholds cited by the authors.1
The sleep-study data also leaned toward hypopneas rather than classic obstructive apneas:
- Median total AHI: 19.5 events/hour, range 5.8-49.4.
- Total hypopneas: median 67, range 6-432.
- Obstructive apneas: median 1, range 0-48.
- Positional OSA: 14 of 22 with usable position data.
- Severe supine OSA: 8 of 14 with available data had supine AHI >30 events/hour.
Hypopneas are partial breathing reductions that fragment sleep and can lower oxygenation. They may be clinically important even when the person is not having many complete airway collapses.
The radiation history supplies a plausible mechanism. Neck and chest radiation can affect soft tissue, airway anatomy, neuromuscular control, thyroid function, vascular health, and cardiopulmonary reserve. The study does not prove a single pathway, but the phenotype is plausible enough to change screening behavior.
STOP-BANG May Underperform in This Survivor Subgroup
STOP-BANG is a common OSA screening tool built around snoring, tiredness, observed apnea, blood pressure, body mass index, age, neck circumference, and male sex.4 It works well for many perioperative and general-risk settings, but it can miss atypical phenotypes.
This cohort illustrates the problem. If the OSA-positive survivor is not severely obese, does not have a large neck, is relatively young at cancer treatment, and reports fatigue more than classic sleepiness, a purely anatomy-heavy screen may under-prioritize testing.
That does not make STOP-BANG useless. It means Hodgkin lymphoma survivorship history should change pretest probability. For this group, the better screen may combine:
- Treatment history: prior mantle or neck/chest radiation.
- Fatigue burden: persistent fatigue not explained by active cancer or another obvious cause.
- Sleep symptoms: snoring, witnessed apneas, non-restorative sleep, insomnia, or morning symptoms.
- Cardiovascular clues: hypertension, arrhythmia, heart failure, or unexplained cardiometabolic deterioration.
Heart Failure Signal Needs Cautious Follow-Up
Retrospective chart review over median 17.5 years found higher heart-failure event rates among OSA-positive survivors vs. those without documented OSA. The adjusted rate ratio was 1.94, p = 0.007, after adjustment for sex and body mass index.1
That result is clinically important but not causal proof. OSA may contribute to cardiac strain, but people who get diagnosed with OSA may also differ in surveillance intensity, symptom burden, radiation exposure, cardiotoxic treatment history, or baseline cardiovascular risk.
Still, Hodgkin lymphoma survivors already have elevated late cardiovascular risk after radiation and some chemotherapy exposures.5 Adding untreated sleep-disordered breathing on top of that risk is not a small concern.
OSA treatment is not guaranteed to erase heart-failure risk, and continuous positive airway pressure adherence can be difficult. But diagnosing a treatable sleep disorder is a reasonable survivorship target when fatigue, cardiovascular risk, and nighttime breathing all point in the same direction.
Limitations of This Hodgkin Survivor Study
Evidence-strength note: this was not a randomized screening trial, and it did not test whether routine sleep testing improves fatigue, cardiovascular outcomes, or survival.
The stronger claim is narrower: among Hodgkin lymphoma survivors with prior mantle radiation, fatigue plus sleep symptoms identified a group with a high diagnostic yield once testing occurred. That supports a lower threshold for asking about sleep-disordered breathing, but it does not estimate the true population prevalence of OSA after Hodgkin lymphoma treatment.
- Testing was selective. Only 42 of 182 survivors had sleep testing, so the paper cannot estimate true OSA prevalence in all Hodgkin lymphoma survivors.
- Some symptomatic people declined testing. Fifteen of the 45 initially referred symptom-positive survivors did not attend testing, which could undercount OSA.
- Chart-review diagnoses varied. Later cases included home sleep testing for some patients, which can underestimate AHI compared with in-lab polysomnography.
- Small event numbers: cardiac analyses are hypothesis-generating, especially for outcomes other than heart failure.
- Radiation-era specificity: mantle radiation exposures in historical Hodgkin treatment may differ from modern involved-site radiation approaches.
Questions About Sleep Apnea After Hodgkin Lymphoma
Should every Hodgkin lymphoma survivor get a sleep study?
No. The study supports a lower threshold for testing when fatigue and sleep symptoms are present, especially after neck/chest radiation history.
Can someone have OSA without severe obesity?
Yes. This cohort is a good example: many OSA-positive survivors were not obese and did not have large neck circumferences.
Does treating OSA reduce late heart failure after Hodgkin lymphoma?
This study does not prove that. It shows an association between OSA diagnosis and higher heart-failure event rate, which should be tested in larger survivorship cohorts.
When should Hodgkin lymphoma survivors ask about sleep testing?
Persistent fatigue after Hodgkin lymphoma treatment should not be assumed to be untreatable survivorship residue. If sleep symptoms are present, OSA testing can be clinically reasonable even when the patient does not fit the classic OSA stereotype.
References
- Occult obstructive sleep apnea in survivors of Hodgkin lymphoma. Li A, et al. Journal of Cancer Survivorship. 2026. doi:10.1007/s44470-026-00075-x
- Persisting fatigue in Hodgkin lymphoma survivors: a systematic review. Daniels LA, et al. Annals of Hematology. 2013;92:1023-1032. doi:10.1007/s00277-013-1793-2
- Obstructive sleep apnea and fatigue in head and neck cancer patients. Zhou J, Jolly S. American Journal of Clinical Oncology. 2015;38:411-414. doi:10.1097/01.coc.0000436086.61460.cb
- STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Chung F, et al. Anesthesiology. 2008;108:812-821. doi:10.1097/ALN.0b013e31816d83e4
- Long-term cause-specific mortality in Hodgkin lymphoma patients. de Vries S, et al. Journal of the National Cancer Institute. 2021;113:760-769. doi:10.1093/jnci/djaa194