
A 2026 pilot randomized trial in 16 frail adults with multiple sclerosis found that 6 weeks of supervised multimodal exercise was feasible: retention was 87.5%, adherence was 97.2%, no adverse events were recorded, and fatigue and quality-of-life scores moved more than they did with waitlist control.1
Research Highlights
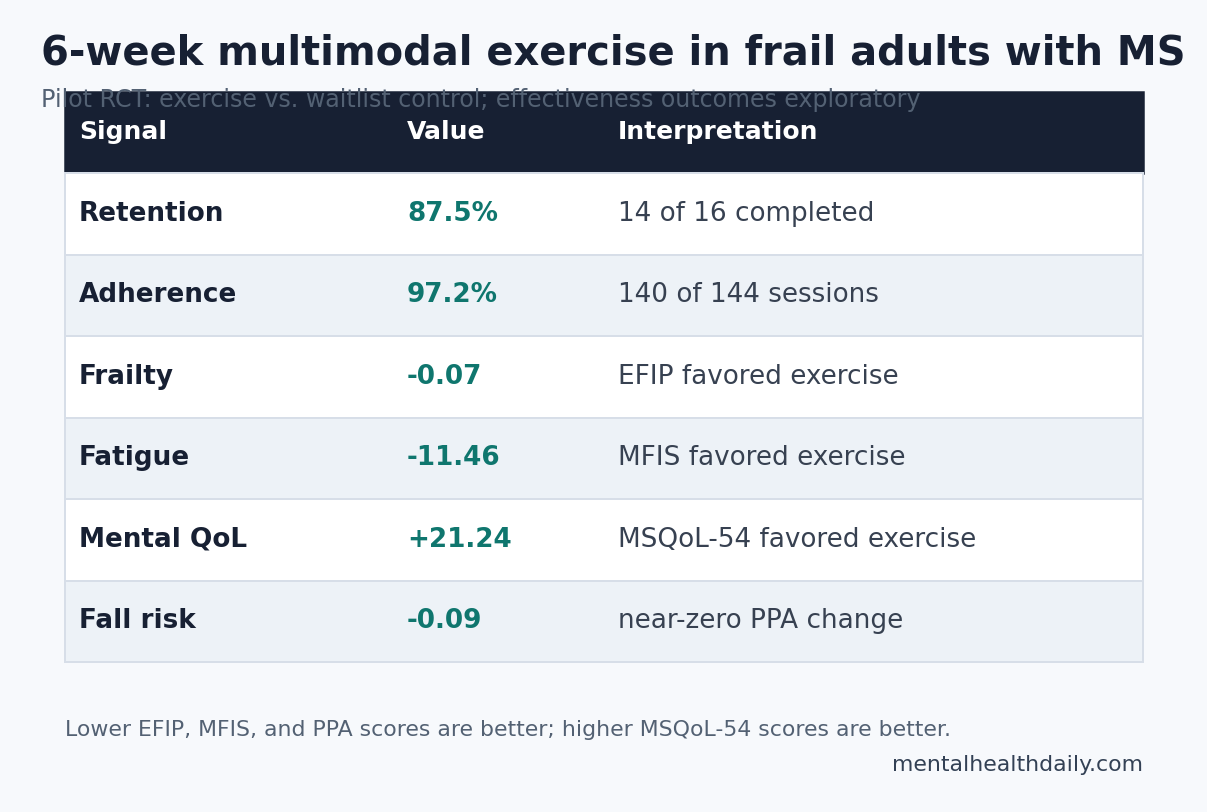
- Feasibility cleared the prespecified bar: 14 of 16 participants completed the trial, and the exercise group completed 140 of 144 planned training sessions.1
- Frailty moved in the expected direction: the Evaluative Frailty Index for Physical Activity changed by −0.08 in the exercise group vs. −0.01 in waitlist control, a between-group difference of −0.07.1
- Fatigue improved more clearly than fall risk: Modified Fatigue Impact Scale change favored exercise by −11.46 points, while Physiological Profile Assessment fall-risk change was near zero at −0.09.1
- Quality of life rose: MSQoL-54 mental health improved by +21.24 points and physical health by +19.26 points more than waitlist control.1
- Recruitment was the weak link: only 8.9% of approached patients consented, and enrollment reached 67% of the planned sample.1
Frailty means reduced physiologic reserve: the body has less margin when illness, fatigue, falls, medication effects, heat, sleep loss, or ordinary exertion add stress. In multiple sclerosis (MS), frailty can overlap with mobility impairment, fatigue, weakness, mood symptoms, cognition, and fall risk, which makes it a neurologic rehabilitation problem as much as an aging construct.
Multimodal exercise training in this trial combined 2 active ingredients: virtual-reality treadmill walking to train gait plus attention-demanding navigation, and progressive resistance training to build strength. The narrow result is still meaningful: frail adults with MS could tolerate the program, and the exploratory symptom signals were large enough to justify a larger efficacy trial.
16 Frail Adults With MS Entered a 6-Week Exercise Trial
Zanotto et al. ran a 2-arm assessor-blinded pilot randomized trial at the University of Kansas Medical Center. Participants were 40–65 years old, had neurologist-confirmed MS, could walk without bilateral support, and met at least 3 Fried frailty phenotype criteria.1
Fried frailty phenotype is a clinical frailty model built around observable features such as weakness, slowness, exhaustion, low activity, and weight loss. Requiring frailty at baseline matters because many MS exercise studies include mixed disability levels and then infer frailty relevance afterward.
Eight participants were randomized to exercise and 8 to waitlist control. The sample was mostly female (81.3%), mean age was 55.0 years, and disease course was mixed: 62.5% relapsing-remitting MS, 18.8% primary progressive MS, and 18.8% secondary progressive MS.1
Evidence-strength note: this was a feasibility trial, not a definitive treatment trial. The sample was small, the control condition was passive, and the investigators treated effectiveness outcomes as exploratory because recruitment fell below the original plan.
The Program Mixed Virtual-Reality Treadmill Work With Strength Training
The exercise prescription was intensive for a frail MS sample: 3 visits per week for 6 weeks, with up to 18 sessions. Each session used 15 minutes of treadmill training with virtual-reality navigation, 30 minutes of resistance training, and another 15 minutes of treadmill training.1
Virtual-reality treadmill training means walking while responding to a projected environment that asks the person to avoid obstacles and navigate a path. In MS, that design is relevant because walking is rarely just leg strength; attention, visual processing, balance, and motor planning all affect real-world mobility.
Progressive resistance training means loading muscles with planned progression over time. Participants performed leg press, knee extension, chest press, and lat-pulldown exercises, beginning at 30% of 1-repetition maximum and progressing toward 80% as tolerated.1
Adjacent MS rehabilitation evidence supports both halves of that logic. A prior 6-week treadmill trial with and without virtual reality reported a frailty-index reduction of 0.024 in 83 people with MS, with the virtual-reality treadmill arm showing a stronger cognitive-frailty signal than treadmill training alone.2
Galperin et al. also tested treadmill training with virtual reality for gait and cognition in MS, providing the motor-cognitive precedent for the walking component.3
Resistance training has its own MS evidence base. A systematic review by Kjolhede et al. found progressive resistance training to be a plausible MS rehabilitation tool, especially for strength and function, and later resistance-training studies reported muscle and MRI-related effects in relapsing-remitting MS.4
Retention and Adherence Were Strong, but Recruitment Was Slow
Feasibility was the primary question, and the trial mostly passed that test. In total, 14 participants completed the study, giving an 87.5% retention rate. In the exercise group, participants completed 140 of 144 planned sessions, or 97.2%. The lowest individual dose was still 16 of 18 sessions.1
- Safety: no adverse events were recorded, median training-related pain was 0.0, and no sessions stopped because of pain or discomfort.
- Data collection: exploratory outcomes had no missing data at assessment visits.
- Engagement: participants agreed or strongly agreed with 95.7% of applicable Study Participant Feedback Questionnaire items.
- Burden: 7 completers said the overall commitment was somewhat more or much more than expected.
Recruitment was the clear constraint. The 16 randomized participants represented 67% of the planned sample, and only 8.9% of approached individuals consented. A 3-times-weekly supervised facility program may be ideal for safety and dose control, but it creates transportation, fatigue, schedule, and effort barriers for the exact population most likely to need it.
Fatigue and Quality of Life Improved More Than Fall-Risk Scores
Evaluative Frailty Index for Physical Activity (EFIP) is a frailty score designed to detect change after physical-activity interventions; lower scores indicate less frailty. EFIP fell from 0.27 to 0.19 in the exercise group and from 0.35 to 0.34 in the waitlist group, producing a between-group change difference of −0.07 (95% CI: −0.14 to −0.00).1
Modified Fatigue Impact Scale (MFIS) measures how fatigue affects physical, cognitive, and psychosocial function; lower scores are better. MFIS improved by −10.13 points in the exercise group and worsened by +1.33 points in controls, a between-group difference of −11.46 points (95% CI: −18.34 to −5.13).1
Quality-of-life signals were also favorable. MSQoL-54 mental health improved by +16.48 points in the exercise group and worsened by −4.76 in controls, while physical health improved by +14.64 with exercise and worsened by −4.63 with control. Between-group differences were +21.24 for mental health and +19.26 for physical health.1
Fall-risk physiology did not show the same pattern. Physiological Profile Assessment (PPA) combines vision, proprioception, reaction time, balance, and strength into a fall-risk z-score. PPA changed by +0.02 in the exercise group and +0.11 in controls, leaving a between-group difference of only −0.09 (95% CI: −1.19 to 1.01).1
That split is clinically coherent. Six weeks may be long enough to improve perceived fatigue, strength confidence, and quality of life, but too short to change a composite fall-risk profile. It also suggests that future MS frailty trials should separate symptom benefit from fall-prevention benefit instead of assuming they move together.
Frailty in MS Includes More Than Walking Disability
Frailty in MS is increasingly treated as a multidomain risk state. A 2024 scoping review reported that frailty is common in MS and linked to poorer outcomes, while a cross-sectional MS study connected multidimensional frailty with lower quality of life and disability.56
That matters for intervention design. A treadmill-only program may improve gait, and a strength-only program may improve muscle function, but frailty bundles motor reserve, fatigue, cognition, mood, and social functioning. A multimodal program is more biologically plausible because it targets several weak links at once.
General frailty evidence points in the same direction. A network meta-analysis of nonpharmacological frailty interventions found that exercise-centered strategies are among the more credible approaches, especially when programs combine strength, balance, and functional training rather than relying on a single narrow modality.7
The Next Trial Needs an Active Control and a Scalable Dose
The trial raises 3 design questions that have to be answered before multimodal exercise becomes a practical MS frailty intervention.
- Comparator: a waitlist control cannot separate exercise-specific effects from attention, travel, expectancy, and supervised contact. A credible next trial needs an active control.
- Access: a facility-based program 3 times per week may exclude people with severe fatigue, transportation problems, work constraints, heat sensitivity, or greater disability.
- Target population: the current sample was ambulatory and age-limited. Older adults with MS and non-ambulatory patients may need adapted cycling, seated resistance training, home-based support, or telerehabilitation.
Practical read: multimodal exercise is a strong candidate for MS frailty, especially when fatigue and quality of life are the outcomes. The evidence does not yet prove durable frailty reversal, fall-risk reduction, or a scalable care model.
Questions About Exercise for Frailty in Multiple Sclerosis
Did the 2026 trial prove that exercise treats MS frailty?
No. It showed feasibility and favorable exploratory changes in a small pilot randomized trial. The findings support a larger efficacy trial, but they do not settle clinical effectiveness.
Was virtual reality necessary?
Unknown. The intervention combined virtual-reality treadmill training with resistance exercise, so the trial cannot isolate which component carried the benefit. Prior MS work supports motor-cognitive treadmill training, but this pilot tested the package.
Why did fatigue improve while fall risk did not?
Fatigue and quality of life can improve through conditioning, confidence, routine, mood, and perceived function. Fall-risk physiology may require longer training, higher dose, different balance work, or a larger sample to detect change.
Who should not generalize from this trial?
People with non-ambulatory MS, severe cognitive impairment, unstable cardiovascular disease, active psychiatric problems, or major orthopedic barriers were not represented. The results also do not show whether unsupervised home exercise would work.
References
- Zanotto T, Tabatabaei A, Lynch SG, He J, Lysaught M, Ahmadnezhad P, et al. Reducing frailty in frail people with multiple sclerosis: Feasibility of a 6-week multimodal exercise training program. PLOS One. 2026;21(4):e0347063. doi:10.1371/journal.pone.0347063
- Zanotto T, Galperin I, Pradeep Kumar D, Mirelman A, Yehezkyahu S, Regev K, et al. Effects of a 6-Week Treadmill Training With and Without Virtual Reality on Frailty in People With Multiple Sclerosis. Archives of Physical Medicine and Rehabilitation. 2025;106(2):187–194. doi:10.1016/j.apmr.2024.09.010
- Galperin I, Mirelman A, Schmitz-Hubsch T, Hsieh KL, Regev K, Karni A, et al. Treadmill training with virtual reality to enhance gait and cognitive function among people with multiple sclerosis: a randomized controlled trial. Journal of Neurology. 2023;270(3):1388–1401. doi:10.1007/s00415-022-11469-1
- Kjolhede T, Vissing K, Dalgas U. Multiple sclerosis and progressive resistance training: a systematic review. Multiple Sclerosis. 2012;18(9):1215–1228. doi:10.1177/1352458512437418
- Al Worikat N, Molaei F, Zanotto A, Tabatabaei A, Lynch SG, Troen BR, et al. Frailty in multiple sclerosis: A scoping review. Multiple Sclerosis and Related Disorders. 2024;92:106157. doi:10.1016/j.msard.2024.106157
- Frau J, Mulasso A, Coghe G, Melis M, Beratto L, Cuomo S, et al. Multidimensional frailty and its association with quality of life and disability: A cross-sectional study in people with multiple sclerosis. Multiple Sclerosis and Related Disorders. 2023;79:105036. doi:10.1016/j.msard.2023.105036
- Sun X, Liu W, Gao Y, Qin L, Feng H, Tan H, et al. Comparative effectiveness of non-pharmacological interventions for frailty: a systematic review and network meta-analysis. Age and Ageing. 2023;52(2):afad004. doi:10.1093/ageing/afad004
- Amatya B, Khan F, Galea M. Rehabilitation for people with multiple sclerosis: an overview of Cochrane Reviews. Cochrane Database of Systematic Reviews. 2019;1(1):CD012732. doi:10.1002/14651858.CD012732.pub2