A 2026 meta-analysis of 54 human studies found that 8-hydroxy-2′-deoxyguanosine rose in Parkinson’s disease, while F2-isoprostanes did not show a statistically confirmed Parkinson’s signal; type 2 diabetes showed much larger peripheral oxidative-stress elevations than Parkinson’s disease for both biomarkers.
Research Highlights
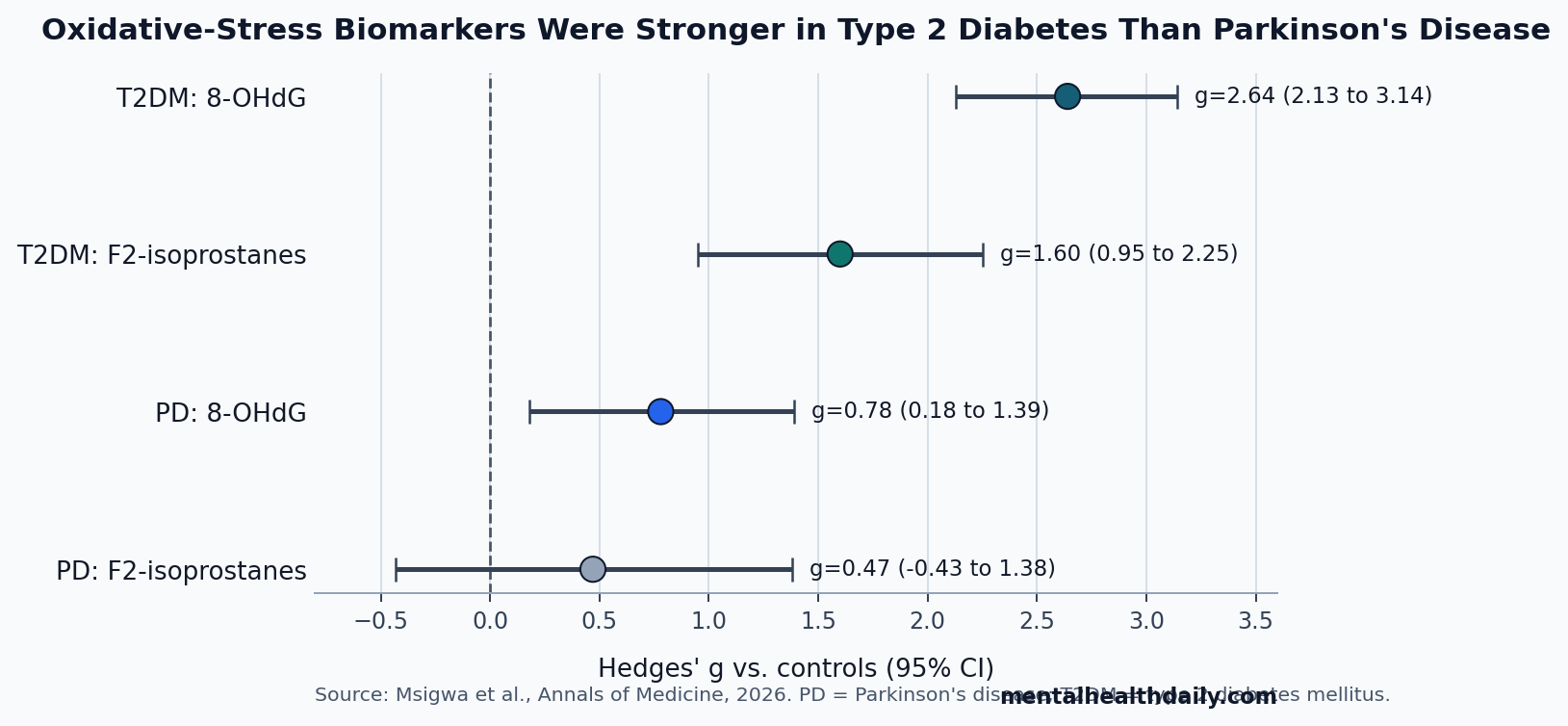
- Parkinson’s DNA-oxidation signal was moderate: Msigwa et al. pooled 5 Parkinson’s disease studies with usable 8-OHdG data and found a moderate elevation vs. controls (Hedges’ g = 0.78, 95% CI 0.18 to 1.39; p = 0.011).1
- Lipid peroxidation did not clear the Parkinson’s bar: F2-isoprostanes were directionally higher in Parkinson’s disease, but the pooled estimate was not statistically confirmed (g = 0.47, 95% CI −0.43 to 1.38; p = 0.303).1
- Diabetes produced a broad systemic signal: type 2 diabetes showed large elevations for both F2-isoprostanes (g = 1.60) and 8-OHdG (g = 2.64), making the diabetes profile much stronger than the Parkinson’s profile.1
- Comorbidity remains untested directly: the meta-analysis compared Parkinson’s disease groups and type 2 diabetes groups with their own controls; it did not pool patients who had both conditions.1
- Assay noise was a major caveat: heterogeneity approached I2 ≈ 97%, and diabetes analyses showed small-study effects, so the biomarker pattern is stronger than the clinical-readiness case.1
Oxidative stress means reactive oxygen species are being generated faster than antioxidant systems can neutralize them. In Parkinson’s disease, that idea is biologically plausible because dopamine metabolism, mitochondrial dysfunction, iron handling, and neuroinflammation can all push vulnerable neurons toward oxidative injury.4
The new meta-analysis is useful because it separates 2 often-blurred peripheral signals. 8-OHdG is a marker of oxidative damage to DNA. F2-isoprostanes are lipid-peroxidation products, usually treated as markers of oxidative injury to cell membranes. If both markers rose similarly in Parkinson’s disease and diabetes, the story would be a broad systemic redox signature. Instead, the pattern was asymmetric.
8-OHdG Rose in Parkinson’s Disease, But F2-Isoprostanes Did Not
Msigwa et al. reviewed 54 unique human studies involving 7,521 people: 3,522 with type 2 diabetes, 722 with Parkinson’s disease, and 3,277 controls. The analysis included adults aged ≥50 years and measured biomarkers in serum, plasma, or leukocytes.1
Hedges’ g is a standardized effect size: around 0.2 is often described as small, around 0.5 as moderate, and around 0.8 as large, although biomarker studies should not be read as symptom-effect studies. The Parkinson’s disease result was a moderate 8-OHdG elevation and a non-confirmed F2-isoprostane elevation.
- 8-OHdG in Parkinson’s disease: g = 0.78, 95% CI 0.18 to 1.39; p = 0.011 across 5 studies.
- F2-isoprostanes in Parkinson’s disease: g = 0.47, 95% CI −0.43 to 1.38; p = 0.303 across 4 studies.
- Study-count caution: the Parkinson’s evidence was much thinner than the diabetes evidence, especially for F2-isoprostanes.
The directional F2-isoprostane point estimate should not be overcorrected into “no signal at all.” It leaned positive. The confidence interval was simply too wide and crossed zero, meaning the pooled Parkinson’s data could not distinguish a real elevation from noise.
Practical read: 8-OHdG is the cleaner Parkinson’s candidate in this evidence base because the point estimate cleared zero and matched the DNA-oxidation hypothesis.
F2-isoprostanes remain biologically plausible, but 4 Parkinson’s studies were not enough to separate a true lipid-peroxidation signal from assay scatter and small-sample instability. The next step is larger, assay-harmonized Parkinson’s sampling rather than treating the lipid marker as settled. Medication state and disease stage also need clearer reporting.
Diabetes Showed a Much Larger Peripheral Oxidative-Stress Profile
Type 2 diabetes gave the analysis its strongest and most consistent peripheral signal. F2-isoprostanes were elevated in diabetes vs. controls (g = 1.60, 95% CI 0.95 to 2.25; p < 0.001; 11 studies), and 8-OHdG was even more elevated (g = 2.64, 95% CI 2.13 to 3.14; p < 0.001; 27 studies).1
Why diabetes dominates the peripheral profile: chronic hyperglycemia, insulin resistance, vascular inflammation, and mitochondrial stress create systemic oxidative pressure. Reviews of type 2 diabetes describe this as a whole-body metabolic problem that blood and serum markers can capture more readily than brain-local oxidative injury.5
The diabetes subgroup results were large enough to be clinically tempting but still not plug-and-play. 8-OHdG effects were especially high in diabetic nephropathy (g = 5.24, 95% CI 2.51 to 7.98) and diabetic retinopathy (g = 3.50, 95% CI 3.13 to 3.87). Those numbers say oxidative DNA damage tracked diabetic complication states in the reviewed literature. They do not establish a standardized clinical threshold for individual risk classification.
Why complication status matters: diabetic nephropathy and retinopathy are vascular and metabolic end-organ damage states. Large biomarker effects in those subgroups may reflect advanced systemic disease, not a simple early-warning signal that can be transferred to Parkinson’s disease risk prediction.
The Parkinson’s-Diabetes Link Is Plausible, But Not Proven by These Markers
Epidemiologic link: diabetes has repeatedly been linked to later Parkinson’s disease risk. Aune et al. pooled 15 cohort studies with 29.9 million participants and 86,345 Parkinson’s disease cases when evaluating diabetes, prediabetes, and Parkinson’s risk.2
Mechanistic overlap: reviews connect the 2 conditions through insulin signaling, mitochondrial dysfunction, neuroinflammation, and cellular stress pathways.3
Peripheral oxidative-stress markers fit that framework, but they sit several steps away from proof. The 2026 meta-analysis did not compare people with Parkinson’s disease plus type 2 diabetes against people with Parkinson’s disease alone. It compared separate Parkinson’s and diabetes study groups against their respective controls.
That design supports a narrower conclusion: 8-OHdG is the more promising peripheral oxidative marker for Parkinson’s disease, while F2-isoprostanes look more robust in type 2 diabetes than in Parkinson’s disease. It does not prove that diabetes raises Parkinson’s risk through oxidative DNA damage.
The missing direct comparison is important. A clinically useful comorbidity study would separate Parkinson’s disease without diabetes, type 2 diabetes without Parkinson’s disease, both conditions together, and neither condition. Without that 4-group structure, the meta-analysis cannot show whether diabetes amplifies oxidative-stress markers inside Parkinson’s disease specifically.
Peripheral Blood May Miss Brain-Specific Oxidative Damage
Parkinson’s disease creates a compartment problem for peripheral biomarkers. Dopamine neurons in the substantia nigra are vulnerable because dopamine can oxidize, mitochondria can fail under high energetic demand, and inflammatory glial signaling can add local stress.4 A peripheral serum or plasma measure may see part of that biology, but it may also miss compartment-specific injury inside the central nervous system.
Assay type also mattered: the included studies used enzyme-linked immunosorbent assays, gas chromatography-mass spectrometry, high-performance liquid chromatography, and other methods. These platforms do not always measure the same biological quantity with the same precision. In the 2026 analysis, heterogeneity was extreme, with I2 values around 97% for the main pooled biomarker analyses.1
High heterogeneity means the studies disagreed substantially about effect size. Some disagreement may come from disease stage, medication exposure, specimen type, age, assay platform, and control selection. That is why the effect direction can be informative while the pooled number remains too unstable for clinical use.
What These Biomarkers Can and Cannot Support
Evidence-strength note: this was a systematic review and meta-analysis dominated by observational and cross-sectional biomarker studies. It can support a research claim about peripheral oxidative-stress patterns. It cannot support causal claims, screening recommendations, treatment selection, or individual prognosis.
For a clinically useful Parkinson’s-diabetes biomarker, the next evidence layer would need to be prospective and comorbidity-specific:
- Comorbid cohorts: enroll people with Parkinson’s disease with and without type 2 diabetes, rather than comparing separate disease literatures.
- Standardized assays: use the same specimen handling and assay platform across sites.
- Brain-relevant sampling: combine blood markers with cerebrospinal fluid, imaging, or other measures closer to central nervous system biology.
- Clinical endpoints: test whether baseline or changing 8-OHdG predicts motor progression, cognition, autonomic symptoms, or treatment response.
Until then, 8-OHdG is best read as a candidate marker of oxidative DNA damage in Parkinson’s disease, not a diagnostic test. F2-isoprostanes remain more convincing as a diabetes-linked oxidative marker than as a Parkinson’s marker.
Questions About Parkinson’s, Diabetes, and Oxidative-Stress Biomarkers
Does this mean oxidative stress causes Parkinson’s disease?
No. The evidence supports association, not causation. Oxidative stress may participate in Parkinson’s biology, but the 2026 meta-analysis did not prove that peripheral oxidative markers cause neurodegeneration.
Is 8-OHdG ready for Parkinson’s screening?
No. The Parkinson’s 8-OHdG signal was moderate and statistically confirmed in pooled data, but the evidence base was small, heterogeneous, and not standardized enough for routine screening.
Why did diabetes show larger biomarker effects?
Type 2 diabetes is a systemic metabolic disease, so blood and serum oxidative-stress markers are more likely to capture its biology. Parkinson’s disease may involve more localized brain oxidative injury that peripheral markers detect only partly.
Which marker looks more relevant to Parkinson’s disease?
8-OHdG looks more relevant than F2-isoprostanes in the current pooled human evidence. The result still needs longitudinal confirmation in Parkinson’s cohorts, especially cohorts with diabetes status measured carefully.
References
- Msigwa SS, Mkwambe MC, Yu QY, et al. Comparative evaluation of oxidative stress biomarkers F2-isoprostanes and 8-OHdG in Parkinson’s disease and Type 2 Diabetes Mellitus: a systematic review and meta-analysis of human studies. Annals of Medicine. 2026;58(1):2654251. https://doi.org/10.1080/07853890.2026.2654251
- Aune D, Schlesinger S, Mahamat-Saleh Y, et al. Diabetes mellitus, prediabetes and the risk of Parkinson’s disease: a systematic review and meta-analysis of 15 cohort studies with 29.9 million participants and 86,345 cases. European Journal of Epidemiology. 2023;38(6):591-604. https://doi.org/10.1007/s10654-023-00970-0
- Konig A, Outeiro TF. Diabetes and Parkinson’s disease: understanding shared molecular mechanisms. Journal of Parkinson’s Disease. 2024;14(5):917-924. https://doi.org/10.3233/jpd-230104
- Dias V, Junn E, Mouradian MM. The role of oxidative stress in Parkinson’s disease. Journal of Parkinson’s Disease. 2013;3(4):461-491. https://doi.org/10.3233/jpd-130230
- Caturano A, D’Angelo M, Mormone A, et al. Oxidative stress in type 2 diabetes: impacts from pathogenesis to lifestyle modifications. Current Issues in Molecular Biology. 2023;45(8):6651-6666. https://doi.org/10.3390/cimb45080420