
A 2026 cross-sectional study involving 428 employed adults found that poor sleepers reported a median 292.8 mg/day of caffeine, compared with 176.1 mg/day among good sleepers, and total caffeine intake still predicted higher Pittsburgh Sleep Quality Index scores after adjustment (β = 0.147, p = 0.003). The source breakdown is the useful part: black coffee, black tea, Turkish coffee, caffe latte, and espresso accounted for most daily caffeine load, so “how much caffeine?” is often a coffee-and-tea pattern rather than an energy-drink question.
Research Highlights
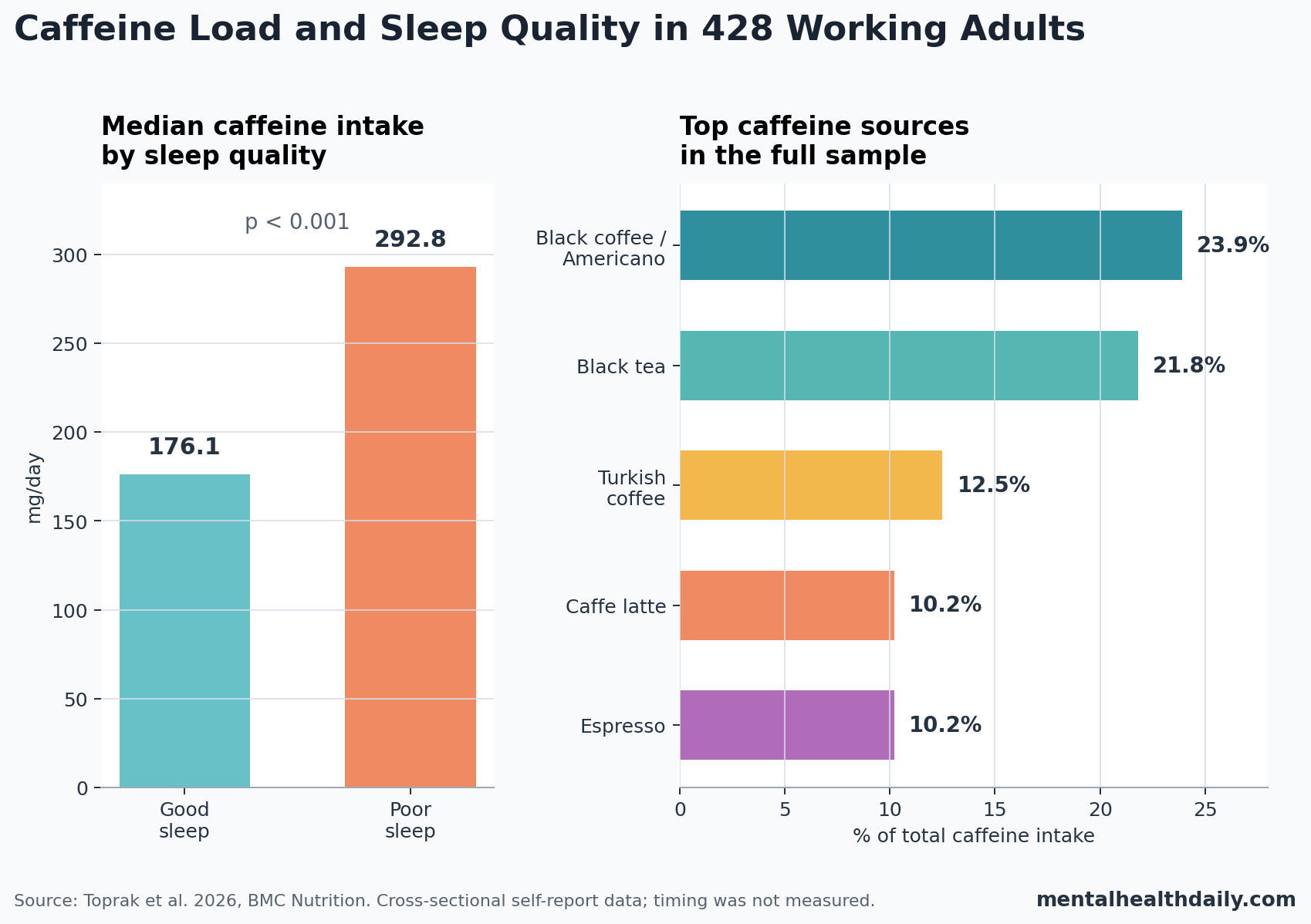
- Poor sleepers consumed more caffeine: median intake was 292.8 mg/day in the poor-sleep group vs. 176.1 mg/day in the good-sleep group (p < 0.001).
- Poor sleep was common: 71.7% of the employed adults scored ≥5 on the Pittsburgh Sleep Quality Index, the usual threshold for poor sleep quality.
- The adjusted signal was modest: total caffeine intake predicted higher total PSQI score after adjustment for age, gender, education, exercise, and chronic disease (β = 0.147, p = 0.003).
- Duration and disturbances carried the association: adjusted links remained for sleep duration (β = 0.107, p = 0.029) and sleep disturbances (β = 0.148, p = 0.002), not every PSQI component.
- Coffee and tea dominated the dose: black coffee/filter-Americano contributed 23.9% of total caffeine intake, black tea 21.8%, Turkish coffee 12.5%, caffe latte 10.2%, and espresso 10.2%.
Caffeine is a psychoactive stimulant that promotes wakefulness mainly by blocking adenosine receptors. Adenosine is a sleep-pressure signal that tends to build during wakefulness; caffeine does not erase the pressure, but it can make the brain less responsive to it while the drug is active.
Causal caveat: the adenosine mechanism makes the Toprak et al. finding biologically plausible, but the paper should not be read as proof that caffeine caused the sleep problems.
Poor sleepers may drink more caffeine because they are tired, higher caffeine intake may worsen sleep, and both pathways can operate inside the same workweek.
Poor Sleepers Reported About 117 mg/day More Caffeine
Toprak et al. recruited adults aged 19–50 years who were actively employed in public institutions in Ankara, Turkey. Researchers estimated caffeine intake with a 30-item quantitative consumption-frequency form covering coffee, tea, soft drinks, energy drinks, chocolate, and caffeinated desserts; sleep quality was measured with the Pittsburgh Sleep Quality Index (PSQI), a self-report scale in which higher scores mean worse sleep and scores ≥5 usually indicate poor sleep quality.
The median participant was 27 years old, 76.4% of the sample was female, and the median body mass index was 23.4 kg/m2. Median total caffeine intake was 262.5 mg/day, with a wide interquartile range from 144.0 to 411.0 mg/day.
The sleep split was sharp. Among 428 participants, 307 were classified as poor sleepers and 121 as good sleepers. The poor-sleep group reported a median caffeine intake of 292.8 mg/day, while the good-sleep group reported 176.1 mg/day. That is a between-group gap of 116.7 mg/day, roughly the caffeine in a strong cup of coffee or several cups of tea depending on preparation.
Evidence-strength note: this was a cross-sectional self-report study. It can show that higher caffeine intake and worse PSQI sleep quality traveled together in this employed sample, but it cannot determine the direction of causality or estimate what would happen if a specific person cut caffeine by 100 mg/day.
The Adjusted Signal Was Real but Not Large
Regression modeling kept the caffeine-sleep association after adjustment for age, gender, education, exercise status, and chronic disease. For total PSQI score, daily caffeine intake had an adjusted unstandardized coefficient of B = 0.0020 and standardized coefficient of β = 0.147 (p = 0.003).
The unstandardized coefficient makes the effect easier to scale. An extra 100 mg/day of caffeine corresponded to about 0.2 additional PSQI points in the adjusted model. That is not a dramatic individual-level shift on a 0–21 scale, but it is directionally consistent with a sleep-cost signal when intake differences accumulate across several drinks per day.
Component-level modeling narrowed the signal:
- Sleep duration: adjusted β = 0.107, p = 0.029.
- Sleep disturbances: adjusted β = 0.148, p = 0.002.
- Subjective sleep quality, sleep latency, habitual sleep efficiency, and daytime dysfunction: caffeine was not a significant adjusted predictor.
- Sleeping medication: regression could not be computed because participants reported no sleep-medication use, leaving no variance to model.
That pattern argues against a cartoon version of the result. The study did not show that caffeine explained every part of poor sleep. It linked caffeine most clearly with shorter sleep and more disturbances, which matches the pharmacology more closely than a broad claim that every sleep-quality domain worsened equally.
Coffee and Tea Accounted for Most of the Caffeine Load
The study’s strongest practical contribution is its source breakdown. In many caffeine discussions, energy drinks get most of the cultural attention. In this employed Turkish sample, ordinary coffee and tea did the heavy lifting.
- Black coffee/filter-Americano: 58.6% consumed it, and it contributed 23.9% of total caffeine intake.
- Black tea: 90.4% consumed it, and it contributed 21.8% of total caffeine intake.
- Turkish coffee: 78.3% consumed it, and it contributed 12.5% of total caffeine intake.
- Caffe latte: 45.1% consumed it, and it contributed 10.2% of total caffeine intake.
- Espresso: only 17.1% consumed it, but intake among consumers was high enough for espresso to contribute 10.2% of total caffeine intake.
Chocolate, cola drinks, green tea, iced tea, and energy drinks were not irrelevant, but they were smaller contributors in the total sample. Energy drinks contributed 1.7% of total caffeine intake, while cola drinks contributed 2.0%.
Timing Is the Missing Variable
Controlled experiments make timing hard to ignore. A 2024 randomized crossover trial by Gardiner et al. tested 100 mg and 400 mg caffeine doses taken 12, 8, or 4 hours before bedtime.
The 400 mg dose reduced objective total sleep time by an estimated 50.6 minutes when taken 4 hours before bedtime and reduced sleep efficiency by 9.5%; the 100 mg dose did not significantly affect objective or subjective sleep outcomes.
That trial helps interpret the Toprak et al. findings. The median daily dose in the employed-adult study was 262.5 mg/day, and the upper half of the distribution included many people above 400 mg/day. If that dose was packed into morning hours, the sleep effect could be smaller. If some of it landed in the afternoon or evening, the same total daily intake could be much more disruptive.
A 2023 systematic review and meta-analysis by Gardiner et al. reached the same general calibration: caffeine can worsen subsequent sleep, but dose, timing, and individual sensitivity change the size of the effect. The practical unit is milligrams, clock time, usual sensitivity, and whether the caffeine is compensating for existing sleep debt.
Why Caffeine Can Fragment Sleep Even When It Feels Helpful
Reichert et al. summarized the adenosine pathway behind the clinical pattern. Adenosine generally promotes sleep pressure through receptor signaling across sleep-wake circuits, while caffeine acts as an adenosine-receptor antagonist. In plain terms: caffeine can make wakefulness feel easier by blocking part of the brain’s sleep-pressure message.
That is why caffeine can be both useful and costly. Morning caffeine may improve alertness and work performance without obviously damaging sleep for many people. Higher total intake, later intake, or slower metabolism can keep the adenosine-blocking effect active when the person is trying to sleep.
Self-perception is also unreliable. In the 2024 Gardiner trial, 400 mg caffeine produced objective sleep changes even when subjective awareness did not fully track the disruption at longer pre-bed intervals. Someone can feel that caffeine “doesn’t affect sleep” while still losing sleep efficiency, slow-wave sleep, or continuity.
Worker Studies Add Context but Not Causality
Toprak et al. is not the only workforce-shaped caffeine/sleep paper. Raju et al. studied young information-technology professionals, and Saglam et al. examined physicians’ caffeine-use problems in relation to sleep quality and professional burnout. Those samples matter because work stress, long hours, and fatigue can turn caffeine into both a symptom-management tool and a possible sleep disruptor.
The direction can run in 2 loops:
- Caffeine-to-sleep loop: heavier or later caffeine intake blocks adenosine signaling, delays sleep, shortens sleep, or fragments sleep.
- Sleep-to-caffeine loop: poor sleep increases fatigue, which drives higher caffeine intake the next day.
Cross-sectional worker studies are vulnerable to both loops at once. Their value is not that they prove causality; their value is that they identify real-world caffeine patterns that controlled lab studies often simplify.
Practical Read: Track Sources Before Moralizing Caffeine
The Toprak et al. data support a source-aware sleep audit. A person trying to improve sleep should count black tea, espresso, Turkish coffee, lattes, filter coffee, cola, chocolate, and energy drinks in the same caffeine ledger rather than treating only coffee as “real” caffeine.
Start with the high-yield questions:
- Total dose: is daily intake closer to 100 mg, 250 mg, or 400+ mg?
- Clock time: does meaningful intake continue after lunch or near the end of the workday?
- Reason for use: is caffeine being used for enjoyment, focus, headache prevention, or rescue from chronic sleep debt?
- Sleep pattern: is the problem short sleep, frequent awakenings, long sleep latency, early waking, or daytime dysfunction?
For someone with poor sleep and a high caffeine load, the data favor a measured experiment: reduce late-day caffeine first, then reduce total dose if sleep duration or disturbances remain poor. For someone using 1 morning coffee and sleeping well, the Toprak et al. study does not justify needless caffeine anxiety.
Questions About Caffeine Intake and Sleep Quality
Does this study prove caffeine caused poor sleep?
No. The study was cross-sectional, so it cannot separate caffeine causing worse sleep from tired people consuming more caffeine. The adjusted association remained statistically significant, but causal direction requires longitudinal or randomized evidence.
Was the median caffeine intake above common safety limits?
The median was 262.5 mg/day, below the 400 mg/day adult limit often cited for healthy adults. The upper part of the distribution reached and exceeded that level, and timing was not measured, so safety-limit language does not settle the sleep question.
Which caffeine source mattered most?
Black coffee/filter-Americano was the largest contributor at 23.9% of total intake, closely followed by black tea at 21.8%. Turkish coffee, caffe latte, and espresso were also major contributors.
What should poor sleepers change first?
Late-day caffeine is the most direct first target because controlled trials show stronger sleep disruption when high doses are taken closer to bedtime. If timing is already early, the next step is lowering total daily load and tracking sleep duration and awakenings for 1–2 weeks.
References
- Toprak K, Yildirim Z, Ayyildiz F. Caffeine intake from different dietary sources and its association with sleep quality in employed adults. BMC Nutrition. 2026. https://doi.org/10.1186/s40795-026-01312-5
- Gardiner C, Weakley J, Burke LM, et al. The effect of caffeine on subsequent sleep: A systematic review and meta-analysis. Sleep Medicine Reviews. 2023;69:101764. https://doi.org/10.1016/j.smrv.2023.101764
- Gardiner C, Weakley J, Burke LM, et al. Dose and timing effects of caffeine on subsequent sleep: a randomized clinical crossover trial. Sleep. 2024. https://doi.org/10.1093/sleep/zsae230
- Reichert CF, Deboer T, Landolt HP. Adenosine, caffeine, and sleep-wake regulation: state of the science and perspectives. Journal of Sleep Research. 2022;31:e13597. https://doi.org/10.1111/jsr.13597
- Raju A, Chandran M, Fredrick J. Excessive day time sleepiness, poor sleep quality, and their association to caffeine consumption among young informational technology professionals. Industrial Psychiatry Journal. 2025;34:191–195. https://doi.org/10.4103/ipj.ipj_247_24
- Saglam B, Tural E, Dayan A. Exploring the link between physicians’ caffeine use disorders with sleep quality and professional burnout: a cross-sectional study. BMC Health Services Research. 2024;24. https://doi.org/10.1186/s12913-024-11360-x