
A 2025 longitudinal analysis of 1,528 older Chinese Americans by Chen et al. in the Journal of Prevention of Alzheimer’s Disease says something more specific than “stress causes Alzheimer’s”: it isn’t the count of stressors that tracks memory decline — it’s a latent trait the authors call stress internalization, a bundle of high perceived stress, hopelessness, and low conscientiousness.1
Research Highlights
- Stress internalization over stressor count: 1,528 Chinese Americans aged 60+ were followed across 3 waves over roughly 4 years.1
- Three-factor stress style: perceived stress, hopelessness, and low conscientiousness loaded together.1
- Memory-decline slope: each 1 SD higher score predicted 0.024 SD more annual memory decline than lower scores (p = 0.015).1
- Baseline vs. decline: acculturation, activity, and education predicted baseline scores, not 4-year decline rate.1
- Cross-cohort convergence: 2 non-Asian cohorts also linked conscientiousness or hopelessness to cognitive decline.2,3
The bundle predicted memory loss across 3 waves. Demographics, neighborhood cohesion, and even acculturation predicted baseline scores but not the rate of decline.1
The paper points the same direction as Wilson’s long-running Rush work in primarily White and Black Americans, where conscientiousness and hopelessness independently predict cognitive decline.2,3 The honest read isn’t that stress causes dementia — it’s that how a person processes stress carries a memory-decline signal that survives adjustment for the usual demographic and clinical predictors.
Stress Internalization Outranked Stressor Frequency in PINE
The PINE cohort is community-based and skews lower-SES than most US Asian-American aging samples. The study context matters because social stress, immigration history, income, and neighborhood exposure are tightly entangled in this population.
- Age: mean age was 71 at wave 1.
- Immigration: mean age at immigration was 52, with an average of about 19 years in the US.
- Socioeconomic context: average education was 9 years, 84% reported annual income under $10,000, and 60% lived in or near Chicago’s Chinatown.1
Exploratory factor analysis on the psychosocial battery collapsed into 3 factors:
- Stress internalization: perceived stress, hopelessness, and low conscientiousness.
- Neighborhood/community cohesion: neighborhood cohesion plus sense of community.
- External stress alleviation: perceived social support plus low perceived stress.1
Linear mixed-effects models entered all demographic, immigration, health, and psychosocial predictors as fixed effects, with time-since-baseline as both fixed and random and a first-order autoregressive covariance structure for within-person clustering. Predictors were stepwise removed at p > 0.15 with an Akaike information criterion (a tool that compares model fit while penalizing extra variables) gate of ΔAIC > 2.
Only stress internalization survived as a sociobehavioral predictor of memory decline. Activity engagement, neighborhood cohesion, and acculturation did not.1
Effect Size: Comparable to a Stroke History, but per Standard Deviation
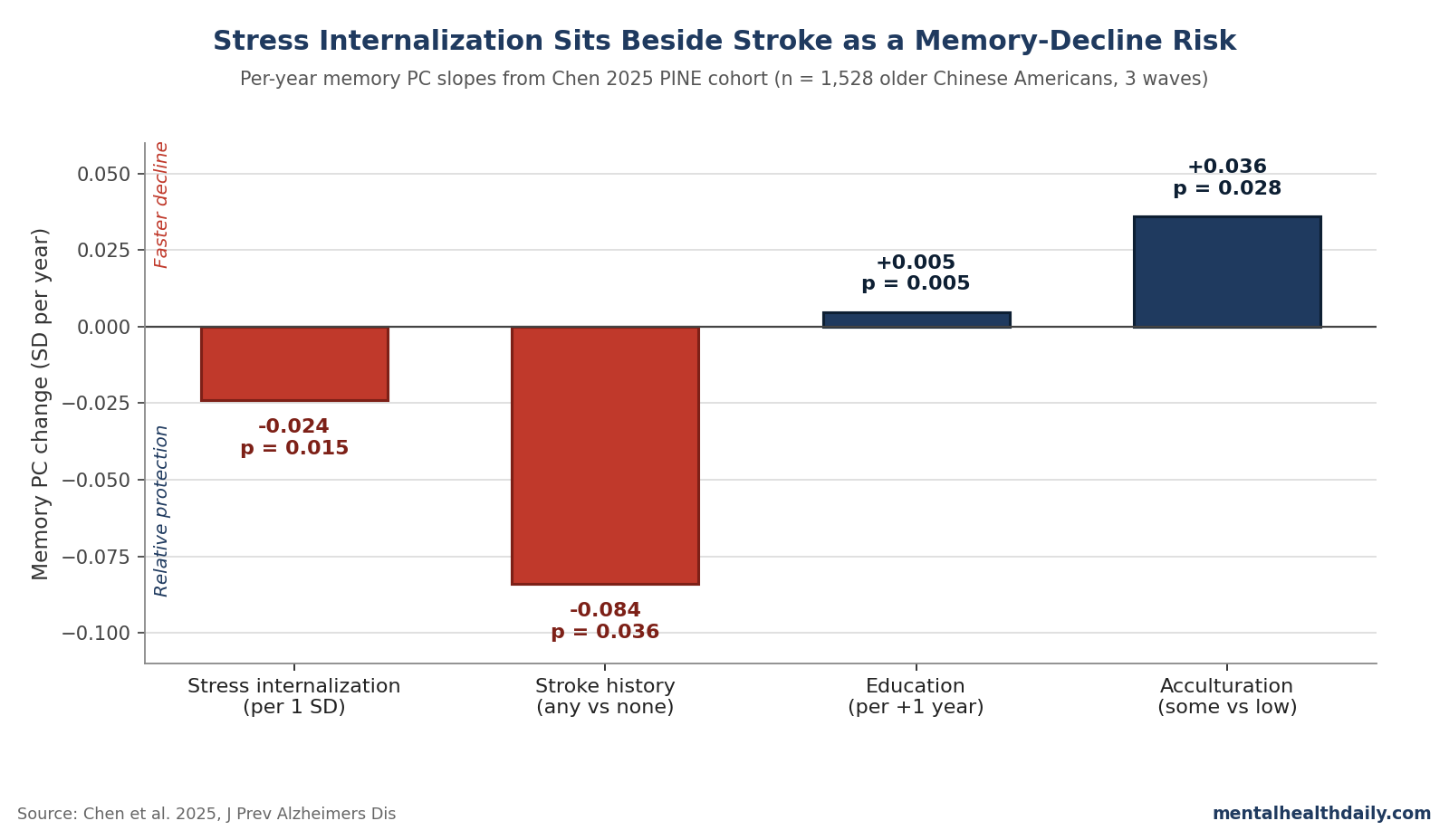
The headline coefficient is a 0.024 SD faster annualized memory decline for each 1 SD increase in the stress-internalization factor. That sounds small — and per-year, it is small — but the comparison numbers in the same model frame it.
For context, having a stroke history (n = 50, p = 0.036) was associated with a 0.084 SD/year greater memory decline in the same cohort. The stress-internalization effect is roughly 29% the size of the stroke effect, per standard deviation of exposure.1
Across the 4-year span of PINE’s 3 waves, a person 2 SD above the cohort mean on stress internalization would lose roughly 0.19 SD more memory function than a person 2 SD below. That gradient is not catastrophic, but it can compound over a decade.
Two qualifiers belong with the number:
- This is a per-SD slope, not a per-stressor effect; the metric is on the latent factor, not on a clinical scale.
- The stroke comparator was based on only 50 stroke cases, so its own confidence interval is wide.
The right read isn’t “stress internalization equals a stroke’s worth of decline.” It’s “stress internalization sits in the same order of magnitude as classical vascular risk factors for memory decline in this cohort.”
Why Older Chinese Americans Are an Underrepresented Cohort
A 2024 systematic review found Asian Americans are systematically underrepresented in Alzheimer’s and related dementia research, with prevalence estimates for Chinese Americans ranging from under 1% to 33% across studies and incidence data essentially unavailable.4
The two large historical cohorts that included Asian Americans — the Honolulu-Asia Aging Study (Japanese American men in Hawaii) and the Multi-Ethnic Study of Atherosclerosis — aren’t generalizable to the mainland Chinese-American population PINE recruits.5,6 MESA Chinese Americans were comparatively high-SES (64% had at least some college, vs. 23% in PINE).1
Mayeda et al. at UCSF have separately documented that dementia incidence among Asian Americans is heterogeneous and that aggregating across Asian subgroups masks within-group differences.7 PINE lands in that gap. The signal it returns — that a stress-internalization phenotype tracks memory decline in a low-SES, largely immigrant, mostly enclave-dwelling sample — isn’t the kind of result that reproduces automatically from White-cohort templates.
HPA Axis and Inflammatory Pathways: Plausible but Not Proven Here
The standard mechanism for why chronic stress would harm memory runs through the hypothalamic-pituitary-adrenal axis (the body’s main stress-response system) and downstream inflammation. Sapolsky’s decades of glucocorticoid-and-hippocampus work established that prolonged cortisol elevation can impair hippocampal neurogenesis and synaptic plasticity in animal models.8 McEwen’s allostatic-load framework extended that to humans: the wear-and-tear of cumulative stress responses, not stress exposure per se, predicts downstream disease.9
The inflammatory leg has independent support. Chronic perceived stress correlates with higher IL-6 (a pro-inflammatory signaling molecule), CRP, and TNF-alpha, and several of those markers prospectively predict cognitive decline.10 A meta-analysis of the Copenhagen City Heart Study found higher PSS scores associated with elevated dementia incidence over follow-up.11
None of that is measured directly in PINE. The Chen analysis is a phenotype-to-cognition study, not a biomarker study.
The HPA-and-inflammation route is the most defensible mechanistic candidate, but the design doesn’t pin it — the relationship could equally run through subclinical depression, sleep disruption, vascular reactivity, or pre-symptomatic neurodegeneration that selectively expresses as a higher-distress phenotype. Wilson’s Rush work on distress proneness in midlife predicting later decline argues against pure reverse causation,3 but in any single 4-year window in older adults the chicken-and-egg problem remains live.
Convergence with the Rush MAP and Religious Orders Cohorts
The strongest argument for taking the PINE finding seriously isn’t the p-value — it’s the convergence with prior longitudinal work in culturally distinct populations. Wilson et al., in a 2007 analysis of the Religious Orders Study, found participants in the highest decile of NEO-FFI conscientiousness had an 89% lower risk of incident Alzheimer’s compared to the lowest decile, controlling for age, sex, and education.2
The finding has held up in subsequent MAP analyses. A 2022 analysis using National Alzheimer’s Coordinating Center data extended that to specific depression dimensions, with the “dysphoric” cluster (which includes hopelessness items) showing the strongest link to longitudinal cognitive decline.12
What Chen 2025 adds: the same three traits cluster into a single latent factor in a low-SES Chinese-American immigrant cohort, and that factor predicts memory decline. The convergence across White, Black, and now Chinese-American samples broadens the generalizability claim well beyond what any single cohort could carry.
Limitations of the Chen Analysis
Three caveats deserve weight before any practical inference:
- Selection bias from attrition is substantial. Roughly 1,000 of the original PINE participants were lost to follow-up or excluded for incomplete waves. Dropouts had higher stress internalization, lower neighborhood/community cohesion, older age, and lower cognitive scores at baseline. The analytic sample is a healthier subgroup — which likely understates the stress-internalization effect, but limits transfer to the broader population.1
- Cultural appropriateness of the scales is a live question. The PSS-10, Beck Hopelessness Scale, NEO-FFI conscientiousness, and NSHAP social-support items were developed in mid-20th-century American samples. Forward and back translation with a bilingual community advisory board is the right methodological move, but linguistic accuracy doesn’t automatically produce cultural construct validity. A Chinese-American respondent endorsing hopelessness items may be reporting something clinically different from what those items capture in a White American or Finnish respondent.1
- Mechanism remains underdetermined by the design. The 4 cognitive measures (C-MMSE, EBMT, Digit Span Backward, oral SDMT) are a thin battery for distinguishing hippocampal-memory-specific decline from executive-network-mediated or vascular decline. No imaging, no fluid biomarkers. The selectivity of the effect for memory is suggestive of a hippocampal-stress route, consistent with the Sapolsky/McEwen framework, but suggestion isn’t evidence.8,9
Stress-Response Style Is More Actionable Than Stressor Counts
Popular framing of stress and dementia usually leans on a simple causal claim: chronic stress harms the brain, so reducing stress prevents dementia. The PINE result reframes the variable. The dementia-relevant signal in this sample isn’t the count of stressors a person reports — it’s the response style that turns stressors into a sustained perception of being overwhelmed, hopeless, and low-control.
Reducing stress exposure (job change, relocation, caregiving burden) is often impossible. The response-style construct is closer to what cognitive-behavioral therapy, mindfulness-based stress reduction, and acceptance and commitment therapy directly target — modalities with clearer evidence bases than generic “reduce your stress” advice.13
The PINE-specific layer adds a second implication. The authors flag the “model minority” stereotype as a cultural pattern that may amplify stress internalization in older Chinese Americans — the expectation of silent endurance interacts with low English proficiency, low SES, and reduced healthcare access to produce a high-effort coping pattern that has been described as John Henryism in other low-resourced minority populations.14
Clinical implication: in older adults, stress-management interventions that target rumination, hopelessness, and conscientiousness-adjacent self-regulation are more defensible from this evidence base than interventions that try to reduce stressor counts. That is a calibration of where the prospective signal is strongest, not a treatment claim.
What Older Chinese-American Patients and Families Ask About Stress and Memory
Does this study show that stress causes Alzheimer’s?
No. A latent factor combining high perceived stress, hopelessness, and low conscientiousness was associated with faster memory decline over about 4 years in 1,528 older Chinese Americans. The design is observational and cannot establish causation. Pre-symptomatic neurodegeneration shifting personality before it’s detectable as cognitive decline remains a live alternative.1
Why does stressor frequency not predict decline if stress internalization does?
2 people exposed to the same stressors can differ widely in how much sustained arousal those stressors produce. The PINE factor structure pulled apart the “perceived stress + hopelessness + low conscientiousness” bundle from simpler stress-exposure measures, and only the bundle predicted decline.1
How big is the effect?
A 1 SD higher score on the stress-internalization factor was associated with 0.024 SD faster annualized memory decline than a 1 SD lower score. For comparison, stroke history was 0.084 SD/year in the same model — the stress-internalization effect is roughly 29% of the stroke effect per SD. Modest per year, the gradient can still compound over a decade.1
Does it apply to executive function or just memory?
Just memory. None of the sociobehavioral factors in PINE predicted longitudinal decline in executive functioning. The selectivity is consistent with a hippocampal-stress mechanism but doesn’t prove one.1
Does the result generalize beyond Chinese Americans?
The same 3 traits have been linked to cognitive decline in primarily White cohorts (Rush MAP, Religious Orders Study) and in NACC depression-dimension analyses. The Chen result is the first robust signal in a low-SES, largely immigrant Chinese-American sample. Convergence across culturally distinct populations broadens generalizability, but the effect size may differ.2,3,12
What kind of intervention does this evidence support?
The evidence is observational, so “support” is too strong. What it makes more defensible: stress-management approaches that target the response style — rumination, hopelessness, perceived control — rather than approaches that try to reduce stressor counts. Whether CBT, MBSR, or ACT actually slow cognitive decline is a question for trials, not for PINE.13
References
- Stress internalization is a top risk for age-associated cognitive decline among older Chinese in the U.S. Chen MH, Ma Y, Verma C, Bergren S, Hu WT. The Journal of Prevention of Alzheimer’s Disease. 2025;12(8):100270. doi:10.1016/j.tjpad.2025.100270
- Conscientiousness and the incidence of Alzheimer disease and mild cognitive impairment. Wilson RS, Schneider JA, Arnold SE, Bienias JL, Bennett DA. Archives of General Psychiatry. 2007;64(10):1204–1212. doi:10.1001/archpsyc.64.10.1204
- Distress proneness and cognitive decline in a population of older persons. Wilson RS, Bennett DA, Mendes de Leon CF, et al. Psychoneuroendocrinology. 2005;30(1):11–17. doi:10.1016/j.psyneuen.2004.04.005
- A systematic review/meta-analysis of prevalence and incidence rates illustrates systemic underrepresentation of individuals racialized as Asian and/or Asian-American in ADRD research. Zhu Y, Park S, Kolady R, et al. Alzheimer’s & Dementia. 2024;20(6):4315–4330. doi:10.1002/alz.13818
- Prevalence of dementia in older Japanese-American men in Hawaii: the Honolulu-Asia Aging Study. White L, Petrovitch H, Ross GW, et al. JAMA. 1996;276(12):955–960. doi:10.1001/jama.1996.03540120033030
- Sociodemographic correlates of cognition in the Multi-Ethnic Study of Atherosclerosis (MESA). Fitzpatrick AL, Rapp SR, Luchsinger J, et al. The American Journal of Geriatric Psychiatry. 2015;23(7):684–697. doi:10.1016/j.jagp.2015.01.003
- Inequalities in dementia incidence between six racial and ethnic groups over 14 years. Mayeda ER, Glymour MM, Quesenberry CP, Whitmer RA. Alzheimer’s & Dementia. 2016;12(3):216–224. doi:10.1016/j.jalz.2015.12.007
- Glucocorticoids and hippocampal atrophy in neuropsychiatric disorders. Sapolsky RM. Archives of General Psychiatry. 2000;57(10):925–935. doi:10.1001/archpsyc.57.10.925
- Stress, adaptation, and disease: allostasis and allostatic load. McEwen BS. Annals of the New York Academy of Sciences. 1998;840:33–44. doi:10.1111/j.1749-6632.1998.tb09546.x
- Inflammation and cognitive function in older adults: a meta-analysis. Lai KSP, Liu CS, Rau A, et al. Journal of Neurology, Neurosurgery & Psychiatry. 2017;88(10):876–882. doi:10.1136/jnnp-2017-316201
- Perceived stress and dementia: results from the Copenhagen City Heart Study. Nabe-Nielsen K, Rod NH, Hansen ÅM, et al. Aging & Mental Health. 2020;24(11):1828–1836. doi:10.1080/13607863.2019.1625304
- Specific depression dimensions are associated with a faster rate of cognitive decline in older adults. Soleimani L, Schnaider Beeri M, Grossman H, Sano M, Zhu CW. Alzheimer’s & Dementia: Diagnosis, Assessment & Disease Monitoring. 2022;14(1):e12268. doi:10.1002/dad2.12268
- Mindfulness-based stress reduction for healthy individuals: a meta-analysis. Khoury B, Sharma M, Rush SE, Fournier C. Journal of Psychosomatic Research. 2015;78(6):519–528. doi:10.1016/j.jpsychores.2015.03.009
- Stress, coping, and health outcomes among African-Americans: a review of the John Henryism hypothesis. Bennett GG, Merritt MM, Sollers JJ, et al. Psychology & Health. 2004;19(3):369–383. doi:10.1080/0887044042000193505