A 2026 medRxiv preprint did not find one simple autism excitation-inhibition signature. Bertelsen et al. found 2 EEG-derived E:I neurosubtypes in 286 autistic males: a 47% inhibition-dominant subtype with higher Hurst exponent and lower gamma, and a 53% excitation-dominant subtype with the opposite pattern.1
Research Highlights
- Two subtypes, opposite directions: in 286 autistic males ages 5–21, the optimal EEG clustering solution was 2 subtypes, not a single high-E:I or low-E:I autism pattern.1
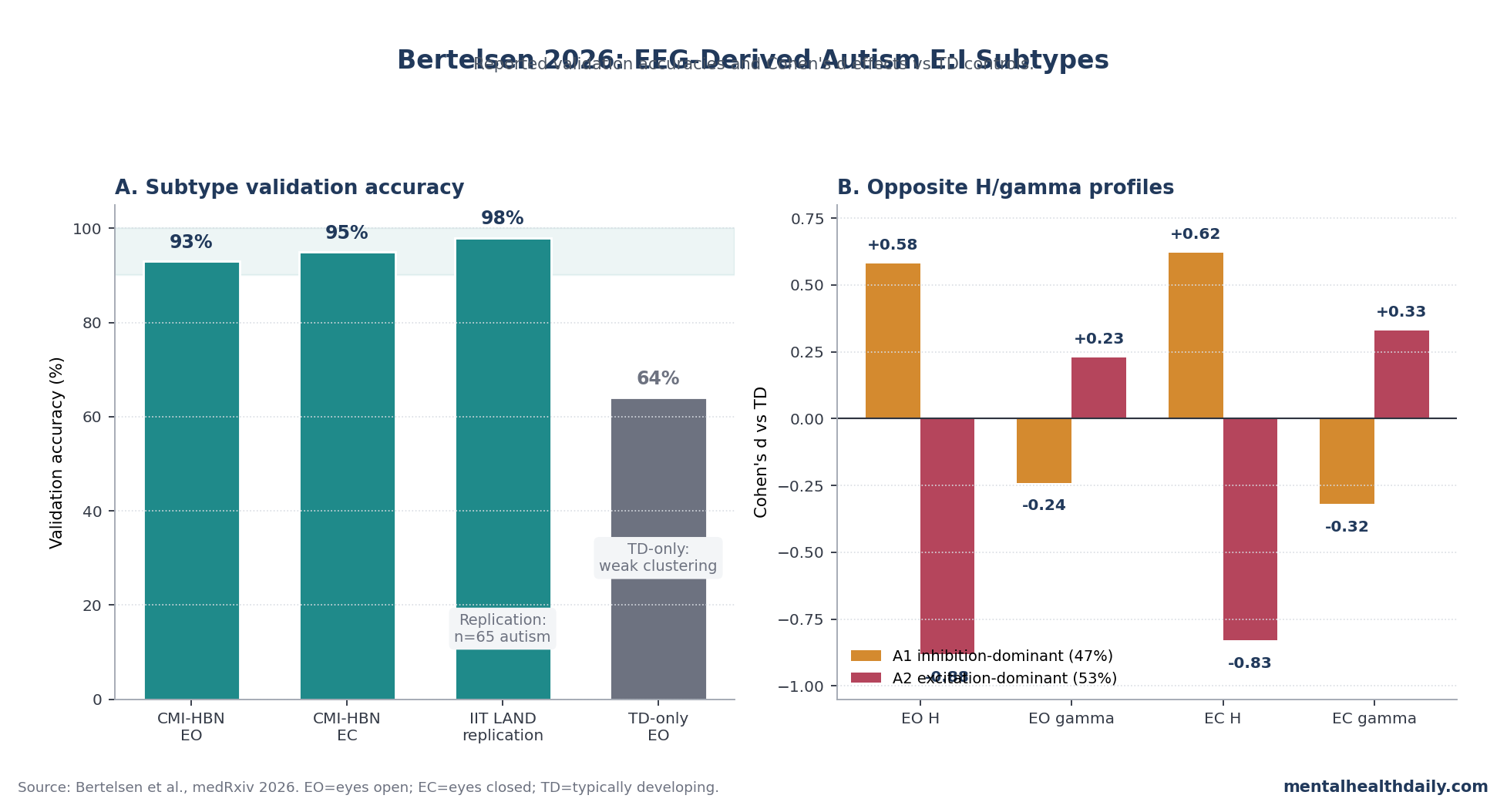
- The validation signal was strong: held-out CMI-HBN accuracy reached 93% with eyes-open EEG and 95% with eyes-closed EEG; an independent IIT LAND sample replicated the 2-subtype classifier at 98% accuracy.1
- The control check mattered: typically developing children did not show comparably robust clustering, with only 64% mean eyes-open accuracy and 59.6% of runs failing the SigClust test.1
- The physiology was not interchangeable: A1 showed higher H and lower gamma vs. typically developing controls (eyes-open H d=0.58; gamma d=-0.24), while A2 showed lower H and higher gamma (H d=-0.88; gamma d=0.23).1
- Treatment matching is not proven: the brain-behavior analysis used 176 autistic participants with consistent subtype labels, but no prospective medication or neuromodulation trial tested whether subtype assignment predicts response.1
Excitation-inhibition balance means the relationship between excitatory signaling, largely glutamate-driven, and inhibitory signaling, largely GABA-driven, inside neural circuits. Autism neuroscience has leaned on this idea since Rubenstein and Merzenich proposed that an increased excitation-to-inhibition ratio could help explain autistic sensory, cognitive, and social features.2
Bertelsen et al. made the older theory more measurable and less simplistic. Their abstract says autism contained “two autism neurosubtypes characterized by opposing profiles of H and gamma,” so the right reading is calibrated confirmation: E:I biology looks relevant, but the direction is not the same across all autistic people.1
Hurst Exponent and Gamma Were Mapped Before the Human Autism Split
The paper used a 3-step translational chain before asking whether human autism clustered into E:I subtypes.1
- Computational model: a recurrent network with 4,000 excitatory and 1,000 inhibitory neurons varied single-neuron excitability and synaptic E:I conductance ratios. Hurst exponent (H; a measure of long-range temporal persistence in the EEG signal) tracked single-neuron excitability, while gamma oscillations (30–50 Hz rhythmic activity) tracked the excitatory-vs.-inhibitory synaptic conductance ratio.
- Mouse validation: 3 chemogenetic experiments altered excitatory neurons, inhibitory neurons, or both. H and gamma moved in the predicted directions often enough that the researchers treated them as complementary readouts, not generic EEG texture.
- Human EEG clustering: H and gamma were estimated across 93 scalp electrodes and 5 repeat blocks in eyes-open and eyes-closed resting conditions, then entered into a stability-based clustering pipeline.
The distinction between H and gamma is the paper’s load-bearing measurement claim. H was not being used as a vague “complexity” marker, and gamma was not being used as a generic arousal marker.
The paper argued that each feature carries different E:I information, and that combining them predicts overall network excitability better than using either feature alone.1
Male Autistic Participants Split Into 47% A1 and 53% A2
The human EEG analysis used Child Mind Institute Healthy Brain Network data from 286 male autistic participants ages 5–21. Female autistic participants were not included in the main subtype analysis because the available sample was too small for the same modeling strategy, which is a major boundary on the result.1
The optimal autism-only solution was 2 clusters in both eyes-open and eyes-closed EEG. Held-out validation accuracy was 93% for eyes-open and 95% for eyes-closed EEG, with SigClust p<0.05 and permutation p<0.05.
Around 80% of participants received the same subtype label across the 2 viewing conditions.1
A classifier trained on the CMI-HBN eyes-open data then identified the same 2 autism subtypes in the independent Italian IIT LAND dataset at 98% accuracy. That replication matters because the dataset used a different country, a different sample, and an “Inscapes” movie-viewing condition rather than a perfectly matched resting-state protocol.1
The typically developing comparison was a useful guardrail. In 123 typically developing participants, 2-cluster solutions did not generalize cleanly: eyes-open mean accuracy was 64%, and 59.6% of runs failed to reject a single-Gaussian null distribution.
That makes the autism split less likely to be a generic artifact of forcing any EEG dataset into 2 groups.1
A1 Looked Inhibition-Dominant; A2 Looked Excitation-Dominant
A1 included about 47% of the autism sample. Compared with typically developing controls, A1 had higher H and lower gamma: eyes-open H d=0.58, eyes-open gamma d=-0.24, eyes-closed H d=0.62, and eyes-closed gamma d=-0.32.
Bertelsen et al. described this as an inhibition-dominant profile.1
A2 included about 53% of the autism sample and moved in the opposite direction: eyes-open H d=-0.88, eyes-open gamma d=0.23, eyes-closed H d=-0.83, and eyes-closed gamma d=0.33. The paper described A2 as excitation-dominant.1
Those labels can sound backwards if H is read casually. The paper’s own computational and animal work is what makes the interpretation coherent: H and gamma were treated as different windows onto circuit physiology, not as 2 interchangeable “more activity” numbers.
“E:I imbalance” is not specific enough. Direction matters.
Brain-Behavior Links Differed More Than Mean Symptoms
The subtype story was not mainly that A1 and A2 had obviously different average symptom profiles. Across 138 phenotypic variables, many autism-vs.-control differences appeared, but mean A1-vs.-A2 separation was less dramatic than a simple clinical-subtype headline would imply.1
Partial least squares analysis, a multivariate method that links patterns across many brain and behavior variables at once, gave the stronger subtype signal. The analysis used 94 typically developing participants and 176 autistic participants with consistent subtype labels across eyes-open and eyes-closed conditions, split into A1 n=87 and A2 n=89.
Across 139 variables in 13 domains, H and gamma each produced 1 FDR-significant latent-variable pair.1
The broad pattern was that A1 related more to autism features, mood, anxiety, ADHD, comorbidity, and sleep, while A2 related more to language and cognition. That is a brain-behavior relationship, not a bedside subtype rule.
It says the EEG physiology tracked different clinical dimensions in the dataset; it does not say a clinician can run a routine EEG and choose a medication tomorrow.
Bumetanide and Other E:I Treatments Need Stratified Trials
Bumetanide is a diuretic studied in autism because it can shift chloride handling and make GABA signaling more inhibitory in some developmental contexts. A 2021 systematic review and meta-analysis described a mixed and still unsettled treatment literature.3
The Bertelsen framework offers a plausible reason why pooled autism trials can look inconsistent: if 2 E:I subtypes need opposite circuit pushes, a mixed sample can average away a real subtype-specific effect.
That is a trial-design hypothesis, not proof that bumetanide, baclofen, glutamate-modulating drugs, repetitive transcranial magnetic stimulation, or transcranial direct-current stimulation should be prescribed by EEG subtype. The needed test is straightforward but has not been done: subtype participants first, randomize within subtype, then test whether the predicted subtype-by-treatment interaction appears.
That calibration also applies to sensory features. Large autism cohorts show sensory symptoms are common but heterogeneous, and sensory hypersensitivity vs. hyporesponsivity has often been treated as a clinical clue that autism is biologically plural.4
Bertelsen et al. add a candidate circuit-level measurement layer, but the paper does not collapse sensory heterogeneity into a single EEG rule.
The Main Boundary Is Clinical Translation
The paper is strong as a translational research argument because it does not jump directly from human EEG to mechanism. It first asks whether H and gamma track controlled E:I manipulations in simulations and mice, then applies those measures to human datasets.
Several limits still matter:
- Preprint status: the paper was posted on medRxiv and had not completed peer review at the time of posting.
- Sex/gender boundary: the main human subtype result was in males; the authors explicitly noted that autistic females require future testing.
- Age and functioning boundary: generalization to younger children, older adults, and autistic people with lower language or cognitive function remains unsettled.
- Clinical-use boundary: no prospective study has shown that subtype assignment predicts treatment response, adverse effects, or long-term outcome.
The good version of this finding is not “there are 2 autisms.” It is narrower and more useful: in the studied male autism datasets, H/gamma EEG features separated 2 reproducible E:I profiles, and those profiles give future trials a better way to stop mixing mechanistically opposite participants.
Questions About Autism E:I Subtypes
Did Bertelsen et al. find a single autism E:I imbalance?
No. The paper supports E:I biology as relevant to autism, but it found 2 opposite profiles rather than 1 direction.
A1 was higher-H/lower-gamma vs. controls; A2 was lower-H/higher-gamma vs. controls.1
Are these EEG subtypes ready for clinical diagnosis?
No. The 93–98% accuracy numbers came from research classification and replication analyses, not from a validated clinical diagnostic workflow.
Autism diagnosis still rests on developmental history, behavior, and standardized clinical assessment.
Why does the male-only sample matter?
E:I biology may differ by sex or gender, and autistic females were not represented enough for the same subtype inference. The article’s strongest claims should therefore be read as claims about the studied male samples, not all autistic people.
Does this mean bumetanide failed because trials mixed subtypes?
It is plausible, not proven. The subtype framework gives a biologically specific explanation for mixed E:I-targeted trial results, but only a prospective stratified trial can show whether one subtype benefits and another does not.
What should readers take from H and gamma?
H and gamma are research EEG features that Bertelsen et al. linked to different E:I mechanisms. They should be read as candidate biomarkers for stratifying studies, not as simple “high brain activity” or “low brain activity” scores.
References
- Electrophysiologically-defined excitation-inhibition autism neurosubtypes. Bertelsen N, Mancini G et al. medRxiv. 2026 (preprint). doi:10.1101/2023.11.22.23298729
- Model of autism: increased ratio of excitation/inhibition in key neural systems. Rubenstein JL, Merzenich MM. Genes, Brain and Behavior. 2003;2(5):255-267. doi:10.1034/j.1601-183X.2003.00037.x
- Bumetanide for the treatment of autism spectrum disorder: a systematic review and meta-analysis. Sprengers JJ et al. European Child & Adolescent Psychiatry. 2021;30(9):1311-1322. doi:10.1007/s00787-020-01538-z
- Sensory features in autism: findings from a large family-based study. Tavassoli T et al. Molecular Autism. 2019;10:22. doi:10.1186/s13229-019-0274-4
- Cortical interneuron development in autism. Cellot G, Cherubini E. Frontiers in Neural Circuits. 2014;8:70. doi:10.3389/fncir.2014.00070
- Inhibitory interneuron deficit links altered network activity and cognitive dysfunction in Alzheimer model. Verret L et al. Cell. 2012;149(3):708-721. doi:10.1016/j.cell.2012.02.046