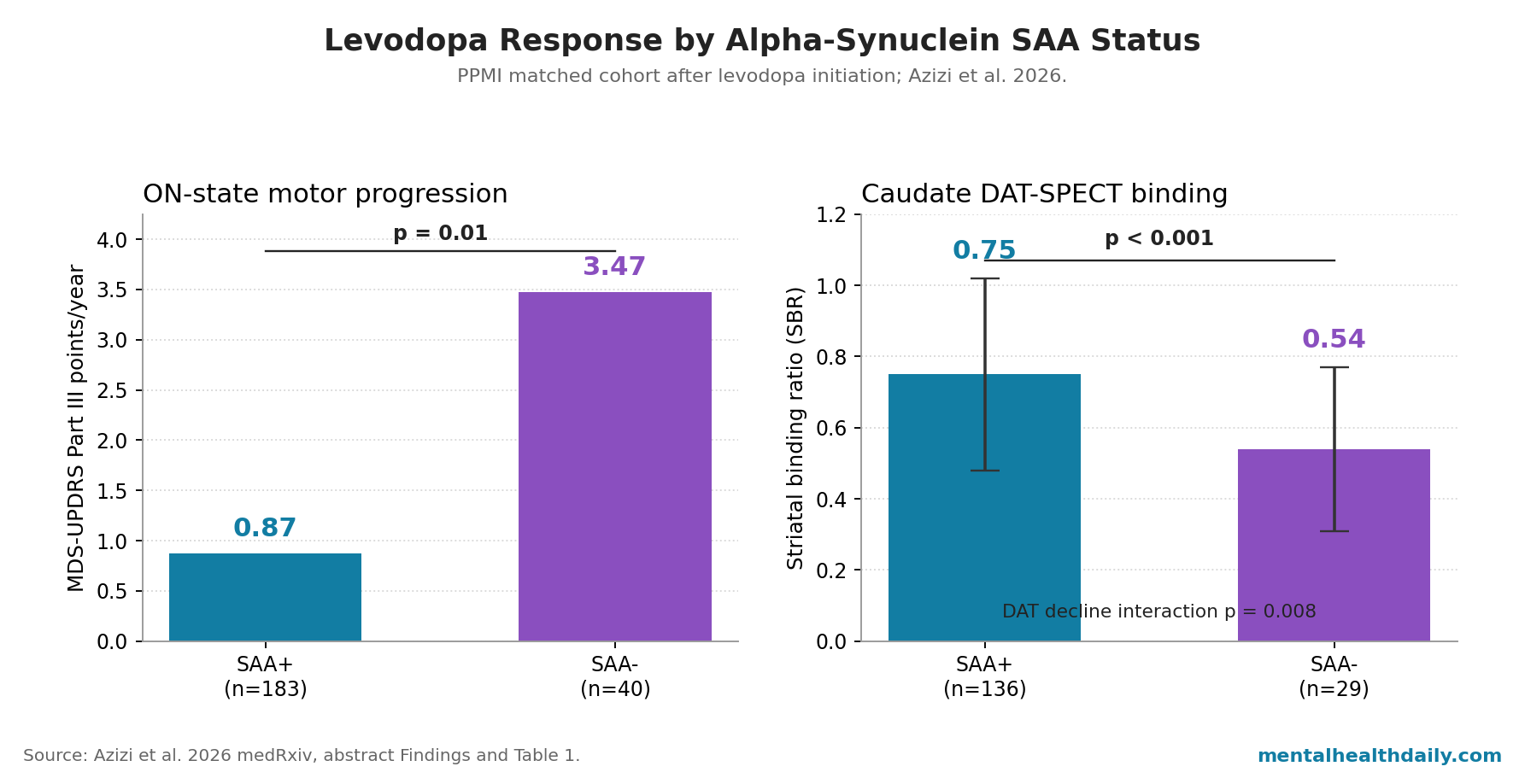
A 2026 PPMI analysis found that Parkinson’s patients with positive CSF α-synuclein seed amplification assay results kept gaining levodopa benefit over follow-up, while SAA-negative patients showed faster ON-medication motor progression than SAA-positive patients: 0.87 vs. 3.47 MDS-UPDRS Part III points/year in 183 matched SAA-positive and 40 SAA-negative patients.1
Research Highlights
- ON-state progression split sharply: SAA-positive patients progressed at 0.87 MDS-UPDRS Part III points/year while SAA-negative patients progressed at 3.47 points/year, with the abstract reporting p = 0.01.1
- Levodopa response diverged over time: proportional responsiveness started similarly at 28.0% vs. 29.9%, then rose by 1.2% per year in SAA-positive patients while falling by 1.7% per year in SAA-negative patients (interaction p = 0.036).1
- DAT-SPECT supplied the mechanism: caudate dopamine-transporter binding was 0.75 vs. 0.54 SBR near treatment initiation, and SAA-negative patients had faster longitudinal DAT decline than SAA-positive patients (interaction p = 0.008).1
- This was not simple non-response: baseline absolute levodopa improvement was 6.6 vs. 7.8 MDS-UPDRS Part III points (p = 0.16), so the key finding is response durability rather than an absent initial medication effect.1
- Clinical translation remains early: the SAA-negative group had 40 patients, the DAT-SPECT subgroup had 29 SAA-negative patients, and the paper is a 2026 preprint rather than a practice guideline.1
CSF α-synuclein seed amplification assay (SAA) is a cerebrospinal-fluid test that amplifies tiny amounts of misfolded α-synuclein until the signal is detectable. In Parkinson’s disease, misfolded α-synuclein is the protein aggregate associated with Lewy-body pathology, while levodopa works downstream by supplying dopamine precursor to surviving nigrostriatal neurons.
Azizi et al. did not show that SAA-negative Parkinson’s patients cannot benefit from levodopa. The sharper read is that SAA status predicted trajectory: similar early levodopa response, then a widening gap as SAA-negative patients lost dopaminergic reserve faster.
40 SAA-Negative Patients Had Faster ON-Medication Motor Progression
Azizi et al. used the Parkinson’s Progression Markers Initiative (PPMI), a multicenter longitudinal cohort of people with recently diagnosed Parkinson’s disease and repeated clinical, imaging, and biomarker assessments.1 The researchers restricted the analysis to sporadic Parkinson’s disease, excluded LRRK2 and SNCA genetic Parkinson’s cases, required baseline CSF SAA testing, and included patients who started levodopa during follow-up.
The matched analysis compared 40 SAA-negative patients with 183 SAA-positive patients. Matching used sex, age, and time since diagnosis at the first post-medication visit, which kept the main comparison from collapsing into a simple older-vs.-younger or longer-disease-duration contrast.
At treatment initiation, the groups were close on age (67.8 vs. 66.6 years), sex (40.0% vs. 37.2% female), disease duration (1.43 vs. 1.37 years), and levodopa equivalent daily dose (295 vs. 288 mg/day).1
The core model separated MDS-UPDRS Part III motor scores in the ON and OFF medication states. MDS-UPDRS Part III is the motor-examination section of the Movement Disorder Society Unified Parkinson’s Disease Rating Scale; higher scores mean worse motor impairment.
In the ON state, SAA-positive patients progressed more slowly than SAA-negative patients: 0.87 vs. 3.47 points/year in the abstract, with the Results section reporting a significant ON-state SAA comparison (β = −2.61, p < 0.001).1
The OFF-medication comparison was weaker. SAA-negative patients trended toward faster OFF-state deterioration, but the interaction did not meet the usual statistical cutoff (β = −1.29, p = 0.066).
That pattern is important: the clearest group separation emerged when patients were assessed on medication, which points toward treatment-response durability rather than just baseline disease severity.
Initial Levodopa Response Was Similar, Then the Trajectories Split
Proportional levodopa responsiveness means the fraction of OFF-state motor impairment that improves in the ON state: (OFF score − ON score) divided by OFF score. At treatment initiation, the 2 groups were essentially similar on that measure: 28.0% in SAA-positive patients vs. 29.9% in SAA-negative patients (β = −0.024, p = 0.47).1
Over time, the pattern changed. Proportional responsiveness increased by 1.2% per year in SAA-positive patients and decreased by 1.7% per year in SAA-negative patients, with a significant time-by-SAA interaction (β = 0.028, p = 0.036).
In plain English: SAA-negative patients did not start out as levodopa nonresponders, but their relative medication benefit eroded while SAA-positive patients maintained or increased the OFF-to-ON gap.
Absolute responsiveness showed the same pattern more softly. Baseline absolute improvement was 6.6 MDS-UPDRS Part III points in SAA-positive patients vs. 7.8 points in SAA-negative patients (p = 0.16).
During follow-up, absolute responsiveness increased by 1.05 points/year in SAA-positive patients and 0.17 points/year in SAA-negative patients, but that between-group slope difference did not reach statistical significance (interaction p = 0.098).1
The calibrated conclusion is not “SAA-positive good, SAA-negative no response.” It is narrower and more useful: SAA-negative Parkinson’s patients in this PPMI analysis showed a shorter durable-response window, especially when response was measured proportionally against worsening OFF-state motor burden.
Lower Caudate DAT Binding Made the Levodopa Pattern Biologically Plausible
DAT-SPECT is dopamine-transporter single-photon emission computed tomography, an imaging method that estimates presynaptic dopaminergic terminal integrity. Lower striatal binding usually means less dopaminergic reserve.
For levodopa, that reserve is not decorative: levodopa has to be converted into dopamine and handled by the remaining dopaminergic system.
Near treatment initiation, 29 SAA-negative and 136 SAA-positive patients had DAT-SPECT imaging. Caudate striatal binding ratio was lower in SAA-negative patients: 0.54 ± 0.23 vs. 0.75 ± 0.27 in SAA-positive patients (p < 0.001).
Longitudinally, both groups lost caudate DAT binding, but SAA-positive patients declined more slowly; the time-by-SAA interaction was β = 0.044 (p = 0.008).1
That imaging result keeps the levodopa-response finding from floating as a purely statistical association. If SAA-negative patients have lower caudate DAT binding at the start of treatment and lose binding faster, the declining proportional response makes pharmacological sense.
The drug is being given into a dopaminergic system with less capacity to convert, release, and buffer dopamine.
SAA-Negative Parkinson’s Should Not Be Collapsed Into Atypical Parkinsonism
Reduced levodopa response can raise suspicion for atypical parkinsonian syndromes, but Azizi et al. were careful not to treat the SAA-negative group as obvious misdiagnosis. The researchers noted that SAA-negative patients still showed measurable early levodopa response, and they argued that lower dopaminergic reserve could explain the later loss of response without requiring that the whole group be reclassified outside the Parkinson’s disease spectrum.1
That calibration fits adjacent work. Siderowf et al. used the PPMI cohort to show that α-synuclein SAA can identify biologically meaningful heterogeneity among clinically diagnosed Parkinson’s patients.2
Brooker et al. later focused on SAA-negative Parkinson’s disease and reported distinct clinical and imaging characteristics, giving the SAA-negative subgroup a phenotype rather than treating it as random assay noise.3
Levodopa-response literature points in the same direction. Malek et al. found in 1,007 early Parkinson’s cases that limited L-dopa response was associated with faster motor progression.4
Martin et al. warned that levodopa response is an imperfect diagnostic indicator, because response patterns do not map cleanly onto pathology in every patient.5 Azizi et al. add the missing biomarker layer: SAA-negative status may mark a subgroup in which levodopa response starts present but becomes less durable as dopaminergic denervation advances.
Motor Complications Did Not Diverge Like Motor Benefit
The motor-complication result is a useful restraint on overinterpretation. At treatment initiation, SAA-positive patients had lower MDS-UPDRS Part IV total scores (β = −1.07, p = 0.001) and lower motor-fluctuation scores (β = −0.90, p < 0.001) than SAA-negative patients.
During follow-up, however, the progression rate of total motor complications, dyskinesia, motor fluctuations, and painful OFF dystonia was similar across groups; all time-by-SAA interaction p-values were >0.15.1
a stronger levodopa-benefit trajectory could have been paired with a sharply worse complication trajectory. The paper did not show that.
SAA-positive patients had more durable motor benefit, but motor complications did not accelerate away from the SAA-negative group in the same way. For treatment planning, the result supports realistic response expectations more than it supports a simple “avoid levodopa complications” rule.
Clinical Use Is Still Trial-Stratification First
CSF SAA is powerful as a biological classifier, but it is not yet a routine community-neurology lever for changing levodopa treatment. The Azizi analysis is a preprint, the SAA-negative sample was small, and treatment exposure was observational rather than randomized.
Levodopa equivalent daily dose was included as a covariate, but dose escalation, adherence, symptom timing, and clinician decisions were not experimentally controlled.1
The strongest immediate use is clinical-trial stratification. If a trial is testing an α-synuclein-directed therapy, enrolling SAA-negative patients can dilute the signal.
If a trial is testing symptomatic dopaminergic strategy, SAA status may help explain why 2 clinically similar patients show different response durability. Rukavina et al. separately linked striatal DaT uptake to levodopa dose requirements in early Parkinson’s disease, which supports the idea that dopamine-transporter imaging can carry treatment-relevant information rather than only diagnostic information.6
For patients already diagnosed with Parkinson’s disease, the result is most useful when the clinical course is mismatched: rapid ON-state worsening, early gait/postural instability, weak durability of benefit despite reasonable dosing, or a question about trial eligibility. A stable, clearly levodopa-responsive patient does not become a different treatment problem just because SAA testing exists.
Questions About SAA Status and Levodopa Response
Did SAA-negative patients fail to respond to levodopa at the start?
No. Baseline proportional response was 29.9% in SAA-negative patients and 28.0% in SAA-positive patients, and baseline absolute improvement was 7.8 vs. 6.6 MDS-UPDRS Part III points.
The source-paper finding is declining durability in SAA-negative patients, not absent initial response.1
Does the 3.47 vs. 0.87 points/year gap prove SAA-negative patients have atypical parkinsonism?
No. The gap supports biological heterogeneity, but Azizi et al. argued against treating atypical parkinsonism as the main explanation for the whole SAA-negative group.
The patients had abnormal DAT imaging and early levodopa response, and only longitudinal monitoring or postmortem validation can settle the underlying pathology for individual cases.1
Why does the DAT-SPECT result matter for interpreting levodopa response?
Levodopa needs surviving dopaminergic terminals to become useful dopamine signaling. SAA-negative patients had lower caudate DAT binding near treatment initiation (0.54 vs. 0.75 SBR) and faster DAT decline over time (interaction p = 0.008), which makes the loss of proportional response biologically plausible instead of just statistically noticeable.1
Should SAA status change levodopa prescribing now?
Not by itself. The result is strong enough to justify biomarker stratification in research and careful counseling in unusual clinical courses, but not strong enough to replace symptom-guided levodopa titration.
The study was observational, preprint-stage, and based on 40 SAA-negative patients.
Did SAA-positive patients pay for better response with faster dyskinesia or fluctuation progression?
The paper did not show that tradeoff. SAA-positive patients had lower motor-complication and motor-fluctuation scores at treatment initiation, while later progression of total complications, dyskinesia, fluctuations, and painful OFF dystonia was comparable between SAA groups, with all progression-interaction p-values >0.15.1
References
- Differential Levodopa Responsiveness and Motor Complication Trajectories in Parkinson’s Disease by α-Synuclein Seed Amplification Assay Status. Azizi H et al. medRxiv. 2026. doi:10.64898/2026.04.21.26350973
- Assessment of heterogeneity among participants in the Parkinson’s Progression Markers Initiative cohort using α-synuclein seed amplification: a cross-sectional study. Siderowf A et al. The Lancet Neurology. 2023;22(5):407-417. doi:10.1016/S1474-4422(23)00109-6
- Clinical and imaging characteristics of Parkinson’s disease with negative alpha-synuclein seed amplification assay. Brooker SM et al. Movement Disorders. 2026. doi:10.1002/mds.70197
- L-dopa responsiveness in early Parkinson’s disease is associated with the rate of motor progression. Malek N et al. Parkinsonism & Related Disorders. 2019;65:55-61. doi:10.1016/j.parkreldis.2019.05.022
- Is Levodopa Response a Valid Indicator of Parkinson’s Disease? Martin WRW et al. Movement Disorders. 2021;36(4):948-954. doi:10.1002/mds.28406
- Early Parkinson’s disease: levodopa requirements are associated with the striatal DaT-uptake. Rukavina K et al. Journal of Neural Transmission. 2026;133:137-142. doi:10.1007/s00702-025-02999-9