A 30-trial meta-analysis found that cholinergic modulators improved schizophrenia negative symptoms, SMD −0.42, while the overall total PANSS/BPRS effect was not statistically significant.1 The clearest signal came from muscarinic agonists, which makes acetylcholine biology promising but not uniformly positive across every cholinergic drug class.
Research Highlights
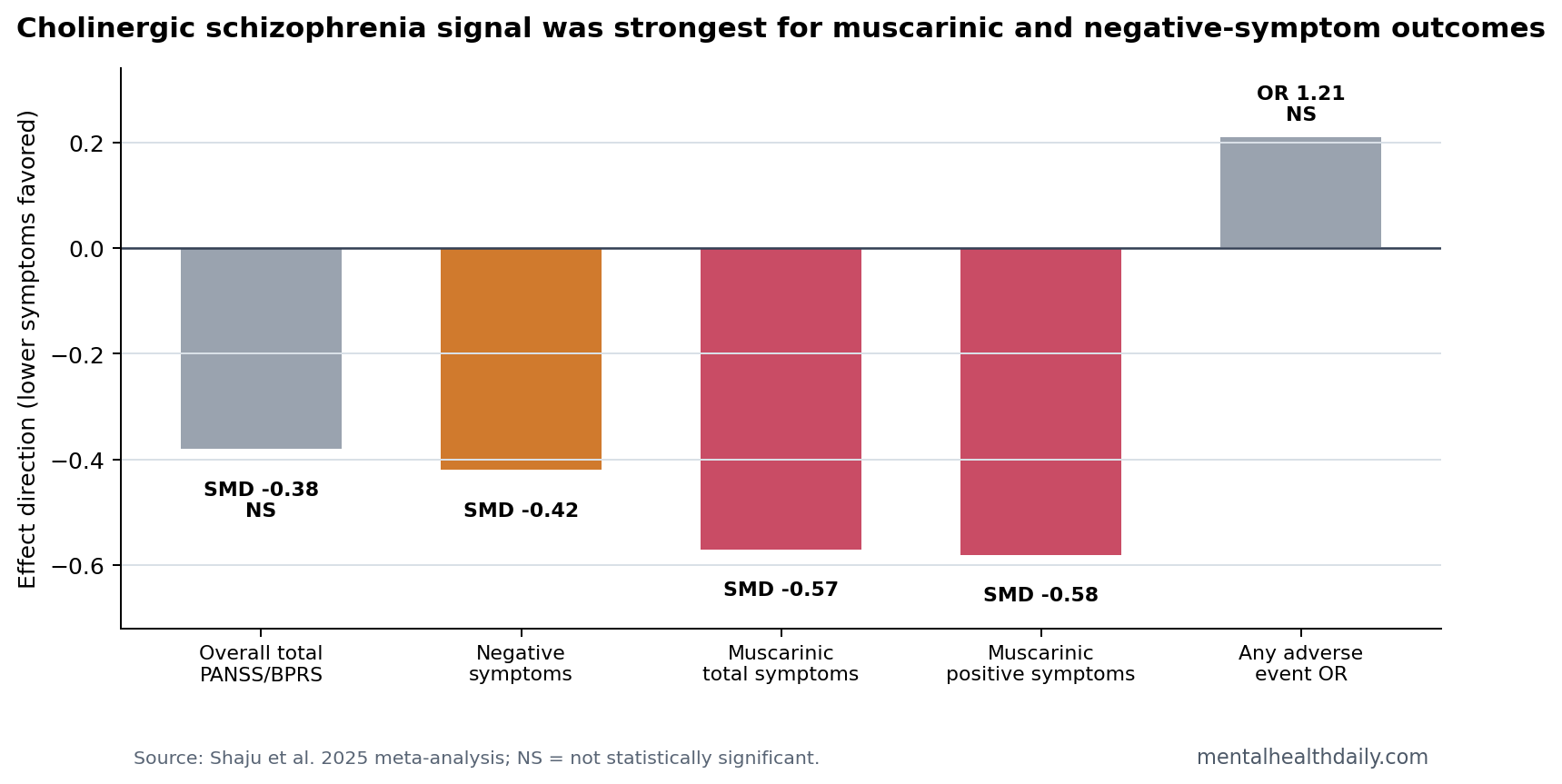
- Negative symptoms improved: Cholinergic modulators reduced PANSS-N/SANS negative symptom scores with SMD −0.42 (95% CI −0.59 to −0.25).1
- Total symptoms were mixed: Overall PANSS-T/BPRS change was SMD −0.38 (95% CI −0.93 to 0.18), p = 0.182, with I² = 97%.1
- Muscarinic agonists carried the strongest signal: The muscarinic subgroup improved total symptoms, SMD −0.57 (95% CI −0.72 to −0.42), positive symptoms, and negative symptoms.1
- Adverse events did not clearly exceed placebo overall: Pooled adverse events showed OR 1.21 (95% CI 0.94 to 1.56), though class-specific tolerability still matters.1
- The class label is too broad: A 30-trial synthesis combines muscarinic agonists, nicotinic agonists, acetylcholinesterase inhibitors, and dual approaches that did not behave identically.
Cholinergic modulators are drugs that alter acetylcholine signaling. Acetylcholine is a neurotransmitter involved in attention, salience, cortical processing, autonomic function, and striatal dopamine regulation. In schizophrenia, the most relevant split is between muscarinic receptors, especially M1 and M4, and nicotinic receptors, including alpha7 nicotinic receptors.
PANSS means Positive and Negative Syndrome Scale. It separates positive symptoms such as hallucinations and delusions from negative symptoms such as blunted affect, low motivation, and reduced social engagement. Negative symptoms are often harder to treat with standard dopamine-blocking antipsychotics.
The 2025 review is useful because it does not treat acetylcholine as one drug target. It separates muscarinic agonists, nicotinic agonists, acetylcholinesterase inhibitors, and mixed approaches, then asks whether the pooled signal survives across symptom domains. That split matters because a drug that stimulates M1/M4 muscarinic receptors is not clinically interchangeable with an alpha7 nicotinic agonist or a medication that raises acetylcholine indirectly by blocking its breakdown.
Total Symptom Pooling Was Not a Clean Class-Wide Win
Across the full set of cholinergic modulators, the pooled total PANSS/BPRS change was SMD −0.38 (95% CI −0.927 to 0.176), p = 0.182. Heterogeneity was high at I² = 97%, meaning trial results varied widely.1
Heterogeneity means the included studies disagreed on effect size more than would be expected from sampling error alone. In this context, high heterogeneity is clinically understandable: the meta-analysis pooled different receptor targets, different drugs, monotherapy and augmentation designs, and different symptom endpoints.
The sensitivity analysis after excluding high-risk-of-bias studies became statistically significant, SMD −0.24 (95% CI −0.42 to −0.07), but the prediction interval still crossed no effect. That is a calibrated signal, not a simple class-wide verdict.
The study-selection funnel also explains why the pooled estimate should be read carefully. Reviewers started with 4,823 database records and 97 registry records, screened 3,442 unique records, assessed 256 full reports, and ended with 30 randomized trials involving 3,128 participants.1
That is enough evidence to reject the idea that cholinergic treatment is a fringe hypothesis, but it is still a small and heterogeneous clinical literature once split by receptor class.
Moderate certainty for the total and negative-symptom estimates still leaves different confidence levels across drug families. The review rated some evidence domains lower because inconsistency, imprecision, and study-design differences still affect the answer. A receptor-specific interpretation fits the data best: muscarinic agonists look like the strongest therapeutic lane, while the broader cholinergic label remains too blunt for treatment decisions.
Muscarinic Agonists Improved Total, Positive, and Negative Symptoms
The muscarinic subgroup was the strongest part of the paper. Muscarinic agonists improved total PANSS/BPRS, SMD −0.57 (95% CI −0.72 to −0.42), positive symptoms, SMD −0.58 (95% CI −0.73 to −0.43), and negative symptoms, SMD −0.40 (95% CI −0.59 to −0.21).1
Xanomeline-trospium is the best-known modern muscarinic approach: xanomeline stimulates muscarinic receptors, while trospium limits peripheral cholinergic adverse effects. That combination aims to engage central M1/M4 signaling without making nausea, sweating, salivation, and gastrointestinal effects intolerable.
The muscarinic result is also clinically different from a dopamine-only story. Standard antipsychotics primarily reduce dopamine D2 signaling; xanomeline-trospium tries to alter upstream cholinergic control of cortical and striatal circuits.
The review notes that xanomeline targets M1 and M4 receptors, while trospium is added to reduce peripheral muscarinic activation outside the brain.1 That design is an attempt to preserve central antipsychotic effect while limiting the gastrointestinal and autonomic burden that historically made cholinergic drugs difficult to tolerate.
That is why the muscarinic subgroup deserves more weight than the broad pooled total-symptom estimate. A mixed meta-analysis can look indecisive when the true pattern is that one receptor lane works better than the others. Point estimates in this review fit that pattern: muscarinic agonists improved total, positive, negative, and CGI-S severity scores, while nicotinic agonists showed a narrower negative-symptom and severity signal.
Nicotinic Signals Were Narrower Than the Muscarinic Signal
Nicotinic agonists showed a negative-symptom signal in the main subgroup analysis, SMD −0.28 (95% CI −0.47 to −0.09), and a CGI-S signal, SMD −1.31 (95% CI −2.38 to −0.24).1 They did not deliver the same broad total, positive, and negative symptom pattern as muscarinic agonists.
Alpha7 nicotinic receptor drugs have been attractive because alpha7 signaling is tied to sensory gating, attention, and cognition. The clinical record has been uneven, which is why the 2025 meta-analysis is useful: it separates receptor classes instead of treating “acetylcholine” as a single therapeutic lever.
- Muscarinic route: broader symptom signal in the included trials.
- Nicotinic route: narrower negative-symptom and severity signals.
- Acetylcholinesterase route: weaker and less consistent schizophrenia symptom effects.
A separate 2026 network meta-analysis on cognition in schizophrenia gives this receptor split more context. It ranked xanomeline second for composite cognition after lurasidone, while most other antipsychotics had weaker or less stable cognitive rankings.2 That does not prove xanomeline is a cognitive enhancer in routine care, but it keeps the muscarinic signal from being only a psychosis-rating artifact.
Older alpha7 nicotinic trials are the cautionary counterweight. Nicotinic stimulation has a strong mechanistic rationale because schizophrenia is associated with sensory-gating and attentional abnormalities, yet clinical trials have not produced a consistently broad schizophrenia-symptom effect. The practical read is not “nicotinic drugs failed.” It is narrower: nicotinic agonism may still matter for specific negative, severity, or cognitive endpoints, but the current symptom-domain evidence is less complete than the muscarinic evidence.
Adverse-Event Pooling Needs Class-Specific Reading
The pooled odds ratio for any adverse event was 1.21 (95% CI 0.94 to 1.56), which did not significantly exceed placebo overall.1 That headline is reassuring, but it should not erase class-specific tolerability.
Cholinergic drugs can affect nausea, vomiting, diarrhea, sweating, salivation, heart rate, blood pressure, sleep, and cognition depending on receptor selectivity and peripheral exposure. Trospium’s role in xanomeline-trospium exists because peripheral muscarinic activation is a real tolerability problem, not a theoretical footnote.
The adverse-event estimate also has a denominator problem that readers should not miss. “Any adverse event” pools many different drugs and many different side-effect mechanisms into one binary outcome. A nonsignificant OR 1.21 can coexist with clinically meaningful nuisance effects in one drug class and cleaner tolerability in another. For schizophrenia treatment, that distinction matters because adherence often fails on side effects before efficacy can be judged.
For a patient already taking a dopamine-blocking antipsychotic, an adjunctive cholinergic drug must clear a different bar than a monotherapy candidate. It needs to add symptom benefit without worsening the side-effect load enough to make the baseline antipsychotic harder to continue.
The review included both monotherapy and add-on designs, so the pooled safety estimate should be treated as a starting point for class comparison, not the final tolerability answer for any one medication.
Negative Symptoms Are the Practical Target
The most clinically relevant signal is negative symptoms. Standard antipsychotics can reduce delusions and hallucinations while leaving motivation, social engagement, emotional expression, and cognitive function impaired. A drug class that moves negative symptoms through a mechanism beyond dopamine D2 blockade deserves attention.
Negative symptoms are also where false optimism is easiest. Blunted affect, avolition, alogia, and social withdrawal can reflect primary schizophrenia biology, medication side effects, depression, sleep disruption, substance use, poverty, or long-term demoralization.
A rating-scale improvement does not automatically mean a person returns to work, rebuilds social life, or becomes cognitively sharper. The practical claim should stay close to the data: negative-symptom scores improved; durable functional recovery remains a harder endpoint.
The best clinical question is therefore not whether “cholinergic drugs work” in schizophrenia. It is which cholinergic mechanism fits which unresolved symptom domain. Muscarinic agonists currently have the broader symptom signal. Nicotinic agonists remain more endpoint-specific. Acetylcholinesterase inhibitors look less convincing as a broad schizophrenia-symptom strategy. That hierarchy is more useful than a class-wide yes-or-no answer.
Evidence-strength note: the meta-analysis supports a real acetylcholine-pathway signal, especially for muscarinic agonists. It does not prove that every cholinergic modulator works, that effects persist long term, or that symptom gains translate into durable functional recovery.
Questions About Cholinergic Modulators in Schizophrenia
Are cholinergic drugs antipsychotics?
Some are being developed or tested as antipsychotic treatments, especially muscarinic agonists. They differ from standard dopamine D2-blocking antipsychotics because they target acetylcholine receptors more directly.
Which schizophrenia symptoms looked most improved?
Negative symptoms improved across the broader cholinergic pool. Muscarinic agonists showed the clearest wider pattern across total, positive, and negative symptom scores.
Did side effects increase?
Overall adverse events did not significantly exceed placebo in the pooled analysis, but tolerability depends on the specific receptor target and drug. Muscarinic activation can still produce peripheral cholinergic side effects.
Does this replace dopamine-blocking antipsychotics?
Best read: the evidence supports cholinergic modulation as a serious non-dopamine pathway, especially for muscarinic drugs. It does not show that current antipsychotics should be abandoned.
The near-term role is more likely add-on treatment, alternative mechanism development, or symptom-domain targeting for patients whose negative symptoms remain disabling.
References
- Shaju A, et al. Efficacy and safety of cholinergic modulators in schizophrenia. British Journal of Psychiatry. 2025. doi:10.1192/bjp.2025.44
- Olgiati P, et al. Impact of selected second- and third-generation antipsychotics on cognitive dysfunctions in schizophrenia. International Clinical Psychopharmacology. 2026. doi:10.1097/yic.0000000000000607
- Brannan SK, et al. Muscarinic cholinergic receptor agonist and peripheral antagonist for schizophrenia. New England Journal of Medicine. PubMed
- Freedman R, et al. Alpha7 nicotinic receptor agonists and schizophrenia cognition. American Journal of Psychiatry. PubMed