A 36-person experiment found that 18 Hz infrasound raised salivary cortisol and negative mood appraisal even though participants did not detect the infrasound above chance (p = 0.241).1 The result is a controlled acute signal, not proof that every real-world low-frequency noise complaint is physiologically caused by infrasound.
Research Highlights
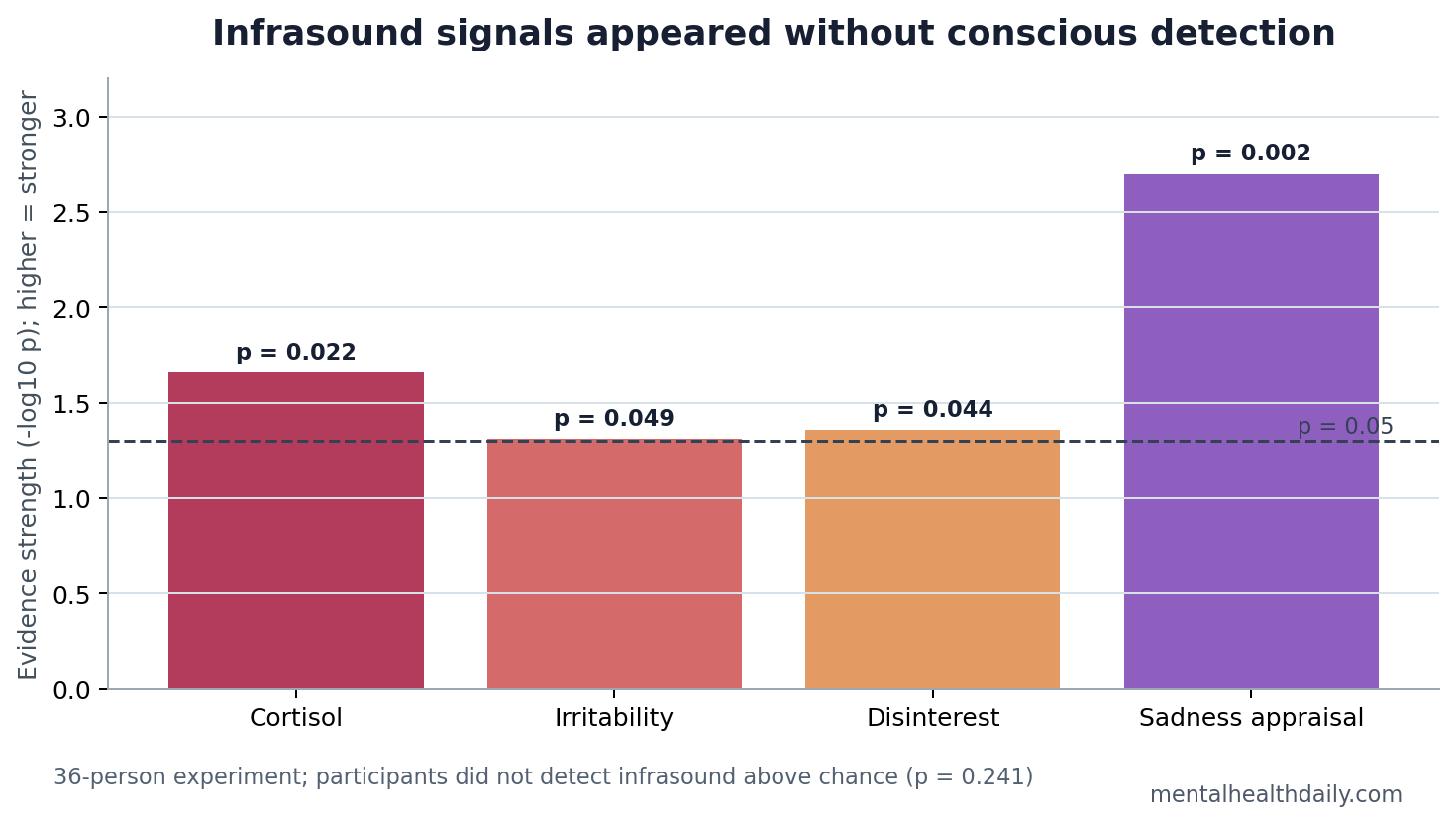
- Cortisol rose with infrasound: Infrasound exposure was associated with higher salivary cortisol (p = 0.022, rrb = 0.390) after the music exposure.1
- Participants did not consciously detect it: Detection was not above chance (p = 0.241), which weakens a simple expectancy-only explanation.1
- Negative appraisal increased: Infrasound was linked to more irritability (p = 0.049), disinterest (p = 0.044 and 0.047), and sadness appraisal (p = 0.002).1
- The design was small and acute: The experiment used 36 participants in a 2 x 2 design, so it tests immediate response rather than chronic environmental exposure.1
- Random-forest signals converged: Interest, irritability, sadness appraisal, and cortisol were among the variables that helped classify infrasound exposure in the model.1
Infrasound means acoustic energy below 20 Hz, beneath the conventional lower limit of human hearing. People usually cannot label it as a sound, but that does not automatically mean the body cannot respond to it.
Salivary cortisol is a saliva-based measure of cortisol, a hormone released through the hypothalamic-pituitary-adrenal axis, the body’s main stress-response system. Cortisol is not a perfect stress meter, but it gives a biological anchor when a study also measures subjective mood.
18 Hz Infrasound Changed Cortisol Without Clear Detection
Scatterty et al. exposed participants to calming or unsettling music with infrasound present or absent. The study used a 2 x 2 between-subjects design: calming vs. unsettling music, and infrasound on vs. off. Saliva was collected before exposure and 20 minutes after exposure onset, while self-report measures were collected immediately after the exposure.1
Participants did not detect the infrasound above chance. That result matters because many infrasound debates collapse into expectancy: people believe a source is harmful, notice symptoms, and then attribute those symptoms to the sound. In this experiment, the physiological and appraisal signals appeared even without conscious detection.
Cortisol signal: infrasound was associated with elevated salivary cortisol (p = 0.022, rrb = 0.390). The rank-biserial correlation gives a nonparametric effect-size read, so the direction had effect-size support even though the sample was still small.
The cortisol timing also keeps the result modest. Saliva was collected immediately before exposure and 20 minutes after exposure onset, which is a reasonable acute stress window but not a chronic exposure measure. The finding says the body responded during a short controlled session; it does not say whether repeated low-frequency exposure produces adaptation, sensitization, sleep disruption, or no durable change.
That is the right level of caution for a 36-person experiment. The useful claim is acute biological reactivity during masked 18 Hz exposure, not a finished clinical syndrome or a universal explanation for environmental noise distress. Replication should test whether the signal survives larger, noisier, real-world samples.
Mood Shifted Toward Irritability, Disinterest, and Sadness
Self-report results moved in the same general direction as cortisol. Infrasound exposure was linked to higher irritability (p = 0.049, eta squared = 0.096), disinterest (p = 0.044, eta squared = 0.121; p = 0.047, eta squared = 0.118), and sadness appraisal (p = 0.002, eta squared = 0.253).1
Eta squared is an effect-size estimate for how much variance in an outcome is associated with a factor in the model. The sadness-appraisal value was the largest of the reported appraisal effects, which fits the paper’s claim that infrasound altered negative subjective experience.
The appraisal pattern converged across several domains. Irritability, disinterest, sadness appraisal, and cortisol all moved in the infrasound-linked direction, and those same domains helped the random-forest model classify exposure. That convergence matters more than any single p-value hovering near 0.05.
The mood results should not be inflated into a diagnosis. Irritability and sadness appraisal after a short exposure are not depression or anxiety disorders. They do show that a low-frequency acoustic condition can shift affective reporting in a controlled setting.
The Experiment Sits Between Nocebo Claims and Environmental Alarm
Infrasound has a long physical-science history. Bedard and Georges described atmospheric infrasound as a real low-frequency acoustic phenomenon generated by natural and human-made sources.2 Urban mechanical systems, ventilation, traffic, wind turbines, storms, and water movement can all produce low-frequency energy.
The mental-health question is different from the physical-acoustics question. The issue is not whether infrasound exists; it is whether subaudible exposure can alter stress physiology, affect, sleep, annoyance, or threat appraisal at realistic exposure levels.
Scatterty et al. are useful because they did not rely only on complaint reports near an environmental source. The experiment manipulated exposure, measured detection, collected cortisol, and tested mood appraisal. That design directly addresses one weakness in purely observational infrasound debates.
Animal and Tissue Studies Make the Human Result Plausible
Bui et al. found that Atlantic salmon changed group behavior in response to light, infrasound, and sound stimuli, supporting animal sensitivity to low-frequency acoustic cues.3 Animal findings cannot be pasted onto humans, but they make it biologically plausible that low-frequency acoustic energy can matter without conscious human labeling.
Chaban et al. tested high-level infrasound in a human myocardial contractility model and reported negative effects in vitro.4 That does not prove that ordinary environmental infrasound damages the heart. It does show that physiological systems can respond to low-frequency exposure under controlled conditions.
Together, those adjacent studies keep the interpretation calibrated. The new human experiment is not isolated weirdness, but it is also not enough to settle chronic exposure risk, building complaints, wind-turbine policy, or individual symptom causality.
What the 36-Person Study Can and Cannot Support
Supported: acute 18 Hz infrasound exposure, embedded in music, was associated with higher cortisol and more negative affective appraisal in a small controlled human experiment. Conscious detection was not required for the signal.
Not supported: a diagnosis of infrasound sensitivity, proof of chronic disease, or a universal explanation for low-frequency noise complaints. The study did not track weeks or months of exposure, sleep architecture, cardiovascular outcomes, or clinical mental-health endpoints.
Most useful next step: repeat the design with larger samples, exposure-dose variation, objective sleep or autonomic measures, preregistered endpoints, and real-world acoustic profiles. Chronic-exposure claims need chronic-exposure data.
Why Detection and Expectancy Still Need Separate Measurement
Expectancy can produce real symptoms. If people believe a sound is dangerous, anxiety, vigilance, poor sleep, and symptom attribution can follow. That pathway is not fake; it is a psychological pathway that can amplify bodily experience.
Scatterty et al. do not erase that pathway. They show that an infrasound-linked signal can appear even when detection is poor. A mature model should allow both routes: direct physiological or affective response in some contexts, and expectancy-driven amplification in others.
Practical research implication: future studies should measure actual acoustic exposure, conscious detection, beliefs about the source, baseline anxiety, sleep quality, cortisol or autonomic physiology, and symptom reporting in the same design. Separating those variables is the only way to stop arguing from anecdotes.
Exposure Measurement Is the Weak Link in Real-World Claims
Environmental infrasound debates often fail before the biology starts because the exposure is poorly characterized. A resident may report a low rumble, a researcher may record broadband low-frequency noise, and a policy discussion may label the whole experience as infrasound even when audible low-frequency sound, vibration, sleep disruption, annoyance, and visual cues are mixed together.
Minimum exposure description: frequency band, amplitude, duration, distance from source, background noise, vibration, time of day, and whether the person could consciously detect the stimulus. Scatterty et al. controlled those pieces more tightly than a field complaint can, which is why the small laboratory result is useful even though it is not the final environmental-health answer.
That distinction also protects people with symptoms. If future work finds that some low-frequency exposures alter cortisol or sleep, the response should be better measurement and mitigation, not vague reassurance. If expectancy explains a large share of symptoms in another setting, the response should still address sleep, anxiety, communication, and trust rather than dismissing the person as imagining it.
Questions About Infrasound and Stress
Can humans respond to sound they cannot hear?
This study suggests that humans may show cortisol and mood-appraisal responses to 18 Hz infrasound even without conscious detection. It does not show that all subaudible sound has meaningful health effects.
Does this prove wind turbines cause anxiety?
No. Wind-turbine exposure involves distance, amplitude, expectation, sleep, visual cues, community conflict, and other noise bands. A short laboratory exposure cannot settle that broader question.
Why use cortisol?
Cortisol gives a physiological stress-response marker that is harder to explain as only questionnaire bias. It still needs cautious interpretation because cortisol changes with timing, sleep, food, stress, and individual biology.
What would make the evidence stronger?
Larger preregistered experiments with dose-response testing, repeated exposure, objective sleep and autonomic measures, and careful expectancy measurement would make the finding more useful for environmental-health decisions.
References
- Scatterty KR, VonStein D, Prichard LB, Franczak BC, Hamilton TJ, Schmaltz RM. Infrasound exposure is linked to aversive responding, negative appraisal, and elevated salivary cortisol in humans. Frontiers in Behavioral Neuroscience. 2026. doi:10.3389/fnbeh.2026.1729876
- Bedard AJ, Georges TM. Atmospheric infrasound. Physics Today. 2000. doi:10.1063/1.883019
- Bui S, Oppedal F, Korsoeen OJ, Sonny D, Dempster T. Group behavioural responses of Atlantic salmon to light, infrasound and sound stimuli. PLoS One. 2013. doi:10.1371/journal.pone.0063696
- Chaban R, Ghazy A, Georgiade E, Stumpf N, Vahl CF. Negative effect of high-level infrasound on human myocardial contractility: in-vitro controlled experiment. Noise & Health. 2021. doi:10.4103/nah.nah_28_19