A 2026 adolescent depression study used resting-state functional magnetic resonance imaging to test whether childhood trauma leaves a measurable network signature in the depressed teen brain. The researchers found disrupted default-mode network hubs in teenagers with major depressive disorder and childhood trauma, and baseline functional-connectome patterns predicted treatment response with 82% accuracy.1
Research Highlights
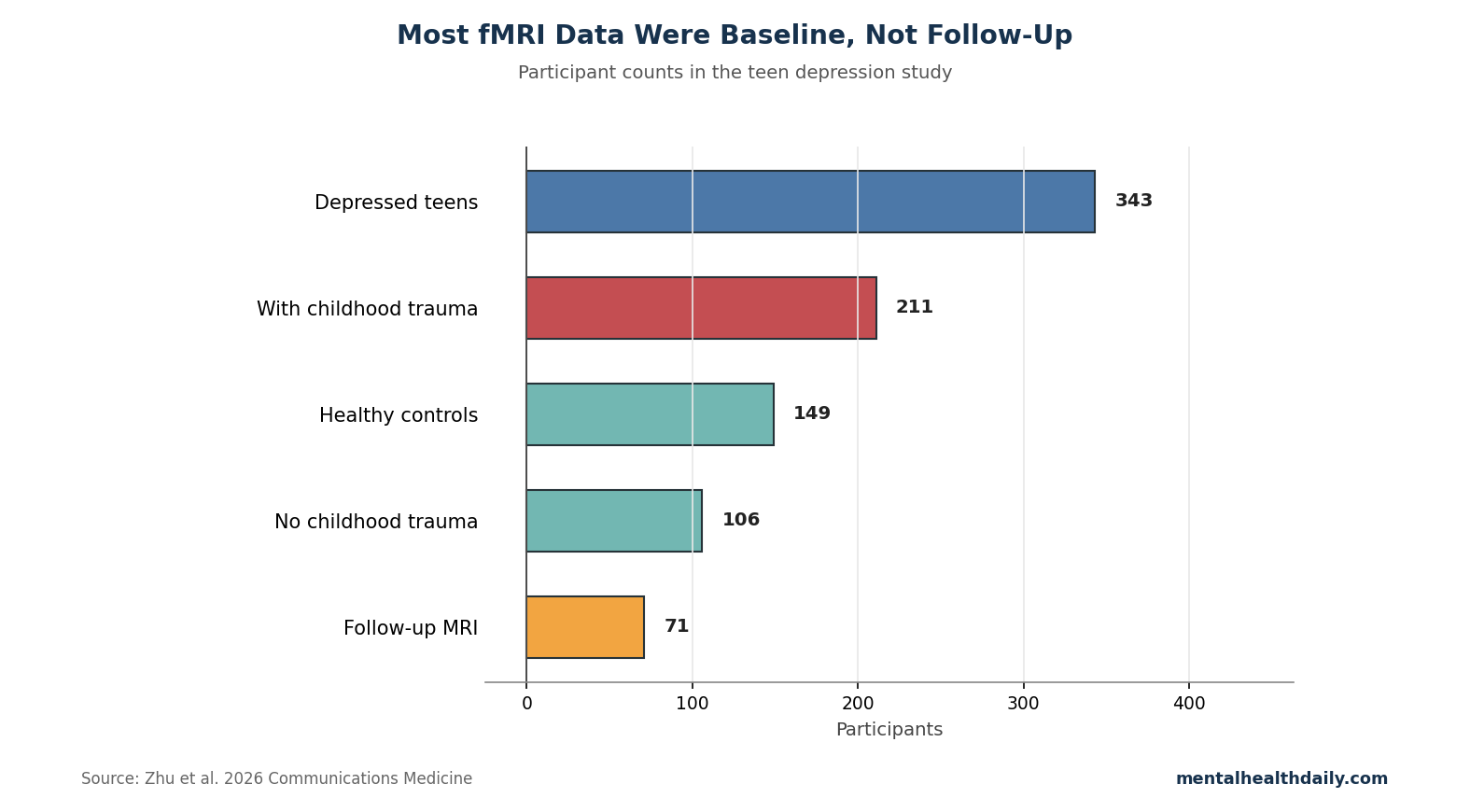
- Large adolescent imaging sample: Zhu et al. analyzed resting-state fMRI from 343 teenagers with major depressive disorder and 149 healthy controls; 211 depressed teens had childhood trauma and 106 did not, with 26 missing trauma-questionnaire data.1
- Trauma tracked network disruption: Childhood trauma was linked to more random functional-network organization and deficits in default-mode hubs including parahippocampal, posterior cingulate, and temporal-pole regions.1
- Treatment response was not evenly distributed: Overall remission in depressed teens was 46.98%, with lower remission in the childhood-trauma group than in the non-trauma group.1
- Follow-up imaging was limited: Only 71 teenagers had post-treatment MRI after an average 44.22 days, so the longitudinal normalization signal is informative but not definitive.1
- Prediction was promising: Machine-learning models using baseline brain-network matrices classified responders vs. non-responders with 82% accuracy.1
Graph theory is a way to describe the brain as a network: regions are nodes, functional connections are edges, and metrics such as efficiency, path length, degree, and small-worldness describe how information can move through the system. In depression research, graph metrics are useful because mood, memory, attention, sleep, and self-referential thinking depend on distributed circuits rather than one isolated spot.
343 Depressed Teens and 149 Controls Made This Larger Than Most fMRI Studies
The study recruited 492 adolescents aged 10–18: 343 with first-episode major depressive disorder and 149 healthy controls. Within the depressed group, 211 teenagers met Childhood Trauma Questionnaire cutoffs for at least 1 trauma domain, 106 did not, and 26 lacked trauma data.1
- Depression severity: The researchers used the 17-item Hamilton Depression Rating Scale, a clinician-rated depression scale.
- Anxiety severity: The study used the 14-item Hamilton Anxiety Rating Scale.
- Trauma exposure: The Childhood Trauma Questionnaire assessed emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect.
- Imaging method: Resting-state fMRI measured spontaneous blood-oxygen-level signal correlations while participants were not performing a task.
The sample size is a strength. Many psychiatric imaging studies are underpowered, especially in adolescents. The tradeoff is that the treatment-response component was much smaller: 71 participants returned for follow-up imaging after treatment, with an average treatment duration of 44.22 days.
Childhood Trauma Was Tied to Default-Mode Hub Disruption
Default-mode network refers to a set of brain regions active during self-referential thought, memory, autobiographical recall, and internally focused attention. In adolescent depression, this network is a plausible trauma-sensitive target because rumination, self-blame, and threat-biased memory often become fused.
Zhu et al. reported trauma-linked disruption in hubs including the left parahippocampal gyrus, posterior cingulate gyrus, and temporal pole. The parahippocampal region helps bind memory and context; the posterior cingulate is a central default-mode hub; the temporal pole contributes to social and emotional meaning.1
Interpretive boundary: These are associations in a cross-sectional imaging design. The study can show that childhood trauma, depressive illness, and brain-network topology travel together in this sample. It cannot prove that trauma caused the imaging pattern in an individual teenager.
Treatment Response Shifted Precuneus and Amygdala Network Measures
The follow-up scan subgroup showed partial normalization after treatment, especially in the left precuneus and amygdala. The precuneus is a medial parietal default-mode hub involved in self-related imagery and memory. The amygdala assigns emotional salience to threat, reward, and social cues.
Changes in left precuneus nodal degree and nodal efficiency correlated with concurrent changes in anxiety and depression scores. In one subgroup split, lower-change participants showed a strong negative correlation between change in nodal efficiency and change in HAMD-17 (r = −0.634, p < 0.001), while the high-change subgroup did not show the same relationship.1
This is a signal for biological heterogeneity. Some teenagers may improve through network reorganization that standard symptom scales only partly capture. Others may improve through medication response, sleep recovery, family stabilization, psychotherapy exposure, or regression toward the mean.
82% Response Prediction Is Promising, Not Clinic-Ready
The machine-learning model used baseline functional-network matrices to classify treatment responders and non-responders. It reached 82% accuracy, which is meaningful for a difficult adolescent depression problem.1
Model caveat: accuracy inside one imaging cohort is not the same as deployable prediction. A clinical tool would need external validation across scanners, countries, treatment types, trauma distributions, medication protocols, and comorbid conditions.
The treatment context also matters. The follow-up interval averaged 44.22 days, which is long enough to capture early HAMD-17 movement but not long enough to prove durable remission, relapse prevention, school recovery, or safety stabilization. The model therefore predicts early response status in this research cohort, not full recovery from trauma-linked depression. Longer follow-up would need to show whether the same network features predict relapse, functional recovery, and sustained safety.
- Useful now: a research signal that trauma-related depression may have measurable network markers.
- Not ready now: an individual scan result that chooses treatment for a teenager.
Replication context: adjacent work on depression neuroimaging has repeatedly shown this gap. Drysdale et al. proposed resting-state connectivity biotypes in depression, but later reanalyses raised concerns about stability and reproducibility.3,4
The adolescent trauma study is strongest when read as a mechanism-and-prediction lead, not as a finished diagnostic test.
How to Read the 82% Prediction Number
The treatment-response model is the most headline-friendly result, but it needs careful translation. A classifier that reaches 82% accuracy in one cohort may be identifying true treatment-relevant biology, scanner-specific quirks, site-specific treatment patterns, or sample characteristics tied to trauma severity and illness burden.
Clinically useful prediction would require the model to answer a practical question before treatment starts: which teenager should receive ordinary antidepressant care, trauma-focused psychotherapy, family intervention, sleep treatment, intensive monitoring, or a faster switch to another modality? Zhu et al. did not test treatment assignment. The model predicted response inside the care pathway used in the study.1
- Internal prediction: useful for identifying a biological signal inside the dataset.
- External prediction: needed before claiming the model works across hospitals, scanners, and populations.
- Treatment-selection prediction: needed before a scan can tell clinicians which intervention to choose.
- Outcome-improvement prediction: needed before biomarker-guided care can be called better than ordinary measurement-based care.
Trauma-Specific Depression Needs More Than Symptom Reduction
Teenagers with depression and childhood trauma often need care that reaches beyond mood scores. Sleep disruption, threat sensitivity, family context, school avoidance, dissociation, self-harm risk, and substance exposure can all keep symptoms active even when a medication reduces sadness or anxiety.
Measurement-based care: repeated symptom scales still matter. But trauma-linked depression also needs repeated safety checks, school-function tracking, sleep assessment, family-support mapping, and attention to avoidance patterns. A brain-network marker could eventually add biological context, but it would not replace direct measurement of daily life.
The strongest clinical implication is prioritization. Depressed teenagers with trauma histories should receive faster measurement-based follow-up than low-risk mild depression. They are a higher-risk subgroup with lower remission and potentially distinct network dynamics.
- Follow symptoms: depression, anxiety, sleep, and self-harm urges.
- Follow function: school attendance, family conflict, avoidance, and peer contact.
What Families Should Take From the Imaging Signal
The useful family-level message is not that a scan can explain a teenager’s depression. It is that trauma-linked depression can involve measurable stress-sensitive brain networks and may need more active follow-up than low-risk depression. A teenager who improves partly but stays avoidant, sleepless, self-harming, or threat-reactive may need treatment adjustment rather than reassurance that the first response is enough.
Care target: symptom remission should be paired with functioning. School attendance, sleep regularity, peer contact, family conflict, substance exposure, and self-harm urges are practical endpoints that imaging studies cannot replace.
Medication Response Is Only One Part of Recovery
Because the study’s follow-up period averaged about 6 weeks, it captured early symptom movement rather than durable recovery. Teen depression with trauma often needs a longer horizon: relapse prevention, sleep repair, family stabilization, school re-entry, and reduced avoidance. A teenager can show a lower HAMD-17 score and still remain functionally stuck.
Practical endpoint: remission should mean fewer symptoms plus better daily function. Imaging biomarkers may eventually help identify risk, but care still has to track real-world recovery week by week.
Questions About Teen Depression, Trauma, and fMRI
Does this mean childhood trauma permanently changes the brain?
No. The follow-up data showed movement toward normalization in some regions after treatment. The study supports plasticity, not fatalism.
Can a teenager get an fMRI to pick an antidepressant?
Not from this evidence. The 82% classifier is a research result, not a clinical test. External validation would be required before it could guide care.
Why does trauma lower remission?
Trauma can add threat learning, sleep disturbance, family stress, dissociation, self-blame, and attachment disruption to depression. Those mechanisms can make ordinary symptom-only treatment less complete.
References
- Graph theory reveals functional connectome disruptions in adolescent major depressive disorder with childhood trauma. Zhu T, Huang Y, Li X, et al. Communications Medicine. 2026. doi:10.1038/s43856-026-01593-8
- Childhood maltreatment and characteristics of adult depression: meta-analysis. Nelson J, Klumparendt A, Doebler P, Ehring T. British Journal of Psychiatry. 2017;210(2):96–104. doi:10.1192/bjp.bp.115.180752
- Resting-state connectivity biomarkers define neurophysiological subtypes of depression. Drysdale AT, Grosenick L, Downar J, et al. Nature Medicine. 2017;23:28–38. doi:10.1038/nm.4246
- Evaluating the evidence for biotypes of depression. Dinga R, Schmaal L, Penninx BWJH, et al. NeuroImage: Clinical. 2019;24:101976. doi:10.1016/j.nicl.2019.101976