A 2026 Scottish health-system preprint used natural language processing of CT and MRI reports to subtype stroke and found that lobar intracerebral hemorrhage carried a higher dementia risk beyond 6 months, aHR 3.49 vs matched controls.1 The method reduced unspecified stroke coding from 26.1% to 3.4%, making location-specific prognosis easier to see.
Research Highlights
- Lobar brain bleeds carried the strongest dementia signal: beyond 6 months, lobar intracerebral hemorrhage had dementia aHR 3.49 (95% CI 2.30-5.29) vs matched controls.1
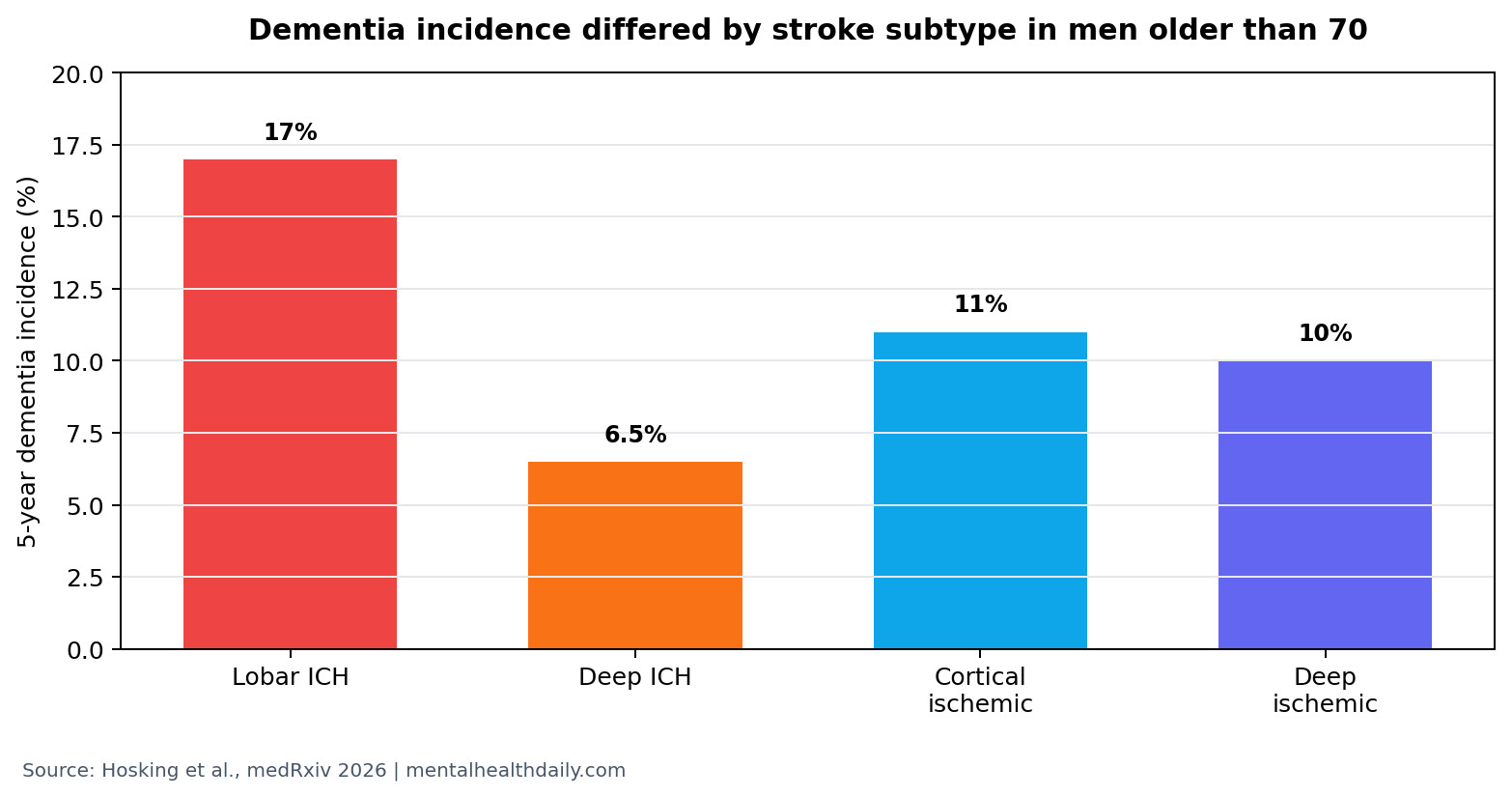
- Absolute dementia risk differed by subtype: in men older than 70, 5-year dementia incidence was 17% after lobar ICH, 6.5% after deep ICH, 11% after cortical ischemic stroke, and 10% after deep ischemic stroke.1
- NLP improved subtype capture: unspecified stroke fell from 26.1% to 3.4% after radiology-report subtyping.1
- Population scale was large: the study linked 785,331 people with head scans and 64,219 people with clinical stroke phenotypes.1
- Epilepsy and MI risks also separated: early epilepsy after lobar ICH had aHR 10.98, while early MI after cortical ischemic stroke had aHR 4.6.1
Natural language processing means software that reads text and extracts structured information. In this study, NLP parsed radiology reports from CT and MRI head scans, then assigned stroke subtypes such as deep ischemic stroke, cortical ischemic stroke, deep intracerebral hemorrhage, and lobar intracerebral hemorrhage.
Intracerebral hemorrhage is bleeding into brain tissue. Lobar hemorrhage occurs in outer brain lobes, while deep hemorrhage occurs in deeper structures. That location distinction matters because lobar hemorrhage is often closer to cerebral amyloid angiopathy and cortical network injury, both relevant to dementia risk.
NLP Reduced Unspecified Stroke From 26.1% to 3.4%
Hosking et al. linked head-scan reports, hospital readmissions, prescriptions, death records, and cancer-registry data in Scotland. The source population included 785,331 people with head scans, and 64,219 people had clinical stroke phenotypes. Mean age was 73.4 years, and 49.5% were male.1
The NLP system subtyped 12,616 deep ischemic strokes, 14,103 cortical ischemic strokes, 1,814 deep intracerebral hemorrhages, and 1,456 lobar intracerebral hemorrhages. Unspecified stroke fell from 26.1% to 3.4%. That is not a cosmetic coding improvement; it changes what prognosis can be estimated from routine data.
Administrative diagnosis codes often flatten stroke into broad categories. Radiology reports contain location and subtype language, but those details are hard to use at population scale unless text can be parsed consistently. This study shows why that extra detail changes dementia, seizure, recurrent stroke, and myocardial infarction risk estimates.
Lobar Intracerebral Hemorrhage Had the Highest Dementia Signal
Beyond 6 months, lobar intracerebral hemorrhage had dementia aHR 3.49, 95% CI 2.30-5.29, vs matched controls.1 Adjusted hazard ratio means the model compared event rates over time after accounting for measured differences between groups.
The absolute-risk contrast helps translate the model. Among men older than 70, 5-year dementia cumulative incidence was 17% after lobar ICH, 6.5% after deep ICH, 11% after cortical ischemic stroke, and 10% after deep ischemic stroke.1
Prior intracerebral-hemorrhage studies already showed substantial post-ICH dementia risk and linked dementia to hemorrhage features, small-vessel disease, and recurrent vascular injury.2,3 The new contribution is population-scale subtype extraction from report text, not a brand-new claim that stroke can precede dementia.
Lobar ICH is clinically different from deep ICH because the likely vascular substrate often differs. Deep hemorrhage is more often tied to hypertensive small-vessel disease in basal ganglia, thalamus, brainstem, or cerebellar regions. Lobar hemorrhage is more often tied to cortical and subcortical injury patterns, including cerebral amyloid angiopathy in older adults.
Cerebral amyloid angiopathy means amyloid deposits in small and medium blood vessels of the brain. It can cause lobar hemorrhage, microbleeds, cortical superficial siderosis, and cognitive decline. The Hosking analysis did not diagnose amyloid angiopathy directly, but the lobar-vs-deep split is one reason the dementia-risk separation is biologically plausible.
The absolute-risk numbers are more useful for counseling than the hazard ratio alone. A 17% 5-year dementia incidence after lobar ICH in men older than 70 is not destiny, but it is high enough to justify planned cognitive follow-up rather than waiting for family members to notice decline years later.
Stroke Location Also Separated Epilepsy and MI Risk
Dementia was not the only outcome that separated by subtype. Early epilepsy after lobar ICH had aHR 10.98, 95% CI 6.82-19.08, compared with aHR 3.42, 95% CI 1.49-7.86, after deep ICH.1
Early myocardial infarction after cortical ischemic stroke had aHR 4.6, 95% CI 3.35-6.31. Readmission with stroke was higher after lobar vs deep ICH, aHR 1.71, 95% CI 1.15-2.54.1
Those findings support a practical view of stroke follow-up. Stroke subtype can change cognitive monitoring, seizure counseling, recurrent-stroke surveillance, cardiovascular evaluation, and the priority given to dementia-risk communication.
Report-Text NLP Is Useful but Not Image Diagnosis
Evidence-strength note: this was a preprint using rules-based NLP on radiology-report text. The system did not directly interpret raw CT or MRI images. It extracted what radiologists had already written, then linked those extracted labels to outcomes.
That distinction matters. Report-text NLP can improve health-system research and audit coding, but it inherits report quality, local language conventions, scan availability, and missing outpatient dementia diagnoses. Individual patients still need clinical assessment, imaging review, cognitive history, and follow-up.
Post-stroke dementia reviews have already emphasized age, prestroke cognition, recurrent stroke, lesion burden, and vascular risk factors.4 NLP-derived subtype data adds location precision to that risk map while clinical assessment still carries the final patient-level interpretation.
Why Routine Records Miss Stroke-Prognosis Detail
Health records often preserve billing and encounter labels better than anatomical detail. A hospital code may say stroke, ischemic stroke, or intracerebral hemorrhage while the radiology report says whether the lesion was cortical, deep, lobar, lacunar, hemorrhagic, or recurrent. Prognosis depends on those details.
That mismatch creates a research problem and a care-quality problem. If 26.1% of strokes remain unspecified in structured fields, a health system cannot easily compare dementia risk by subtype, target follow-up, or estimate which patients need seizure counseling. Reducing unspecified stroke to 3.4% makes the same record system more clinically informative.
The method is also less glamorous than many “AI in medicine” headlines imply. Rules-based text extraction can be valuable precisely because it solves a concrete documentation problem: radiologists already wrote subtype clues, and the software made those clues usable at population scale.
How This Should Change Post-Stroke Follow-Up
The study points toward subtype-aware follow-up rather than one dementia pathway for every stroke survivor. Lobar ICH, cortical ischemic stroke, deep ICH, and deep ischemic stroke carried different dementia, epilepsy, readmission, and myocardial-infarction profiles.
For lobar ICH in older adults, the cognitive signal is the clearest. A 17% 5-year dementia incidence in men older than 70 is high enough to support scheduled cognitive screening, family education about early cognitive changes, medication review, vascular-risk management, and low threshold for memory-clinic referral when symptoms appear.
For cortical ischemic stroke, myocardial-infarction risk and recurrent vascular risk may deserve more attention alongside cognition. For lobar ICH, seizure counseling may be especially relevant because early epilepsy risk was much higher than after deep ICH. The subtype label is not the care plan, but it helps prioritize which risks should be discussed first.
The operational lesson is simple: structured health records should preserve anatomy. When stroke location is lost in generic coding, prognosis gets flattened. When radiology-report detail is recovered, patients can be grouped into more clinically useful risk categories.
The dementia finding should still be interpreted as risk stratification, not fate. Older age, prior cognition, recurrent stroke, vascular risk, education, delirium, depression, medications, and rehabilitation access all shape cognitive outcome after stroke. Subtype improves the map while patient-level history remains essential.
That is why NLP is best used upstream of clinical judgment. It can flag which groups deserve closer follow-up and better counseling, while clinicians still decide whether a specific patient needs cognitive testing, seizure precautions, vascular workup, medication changes, or caregiver support.
The strongest operational use is probably audit and triage. Health systems can identify patients whose report text suggests lobar hemorrhage or cortical ischemic stroke, then check whether cognitive follow-up, seizure advice, vascular prevention, and caregiver education were actually delivered. That turns text mining into a quality-improvement tool rather than a replacement for bedside care.
Questions About Stroke Subtypes and Dementia Risk
Why was lobar hemorrhage linked to more dementia?
Lobar hemorrhage can overlap with cortical injury and cerebral amyloid angiopathy patterns, both of which can affect cognition. This study estimated risk; it did not prove one mechanism for every patient.
Does NLP predict dementia from the scan itself?
No. The study used NLP to read radiology-report text and assign stroke subtype labels. It did not directly analyze raw imaging pixels as a diagnostic AI model.
What should change in follow-up?
Patients with lobar ICH may deserve especially careful cognitive follow-up, seizure counseling, and recurrent-risk review. The exact plan still depends on age, baseline cognition, imaging, comorbidity, and recovery course.
References
- Hosking J, et al. Prognosis of stroke subtypes in whole population health systems data: a matched cohort study. medRxiv. 2026. doi:10.64898/2026.04.17.26351150
- Biffi A, et al. Association between blood pressure control and risk of recurrent intracerebral hemorrhage. JAMA Neurology. 2016. doi:10.1001/jamaneurol.2016.0955
- Moulin S, et al. Dementia after spontaneous intracerebral hemorrhage: a prospective cohort study. Lancet Neurology. 2016. doi:10.1016/s1474-4422(16)00130-7
- Pendlebury ST, Rothwell PM. Incidence and prevalence of dementia associated with transient ischemic attack and stroke. Lancet Neurology. 2019. doi:10.1016/s1474-4422(18)30442-3