Resting-state fMRI studies of postpartum depression have produced inconsistent results for years. A 2026 voxel-based meta-analysis pooled 12 studies of 475 patients and found 4 reliable regional differences (amygdala, precuneus, occipital, precentral cortex) at uncorrected thresholds, none of which held up under strict family-wise error correction.1
Research Highlights
- 12-study fMRI pool: Chen et al. analyzed 475 PPD patients and 504 controls with Seed-based d Mapping (SDM-PSI), pooling ALFF, fALFF, ReHo, VMHC, degree centrality, and cerebral blood flow studies. Patients were DSM-IV/V diagnosed, medication-naive postpartum.1
- 4 uncorrected regions: increased resting-state activity appeared in left inferior occipital gyrus and left precuneus; decreased activity appeared in right amygdala and left precentral gyrus. Hedges’ g effect sizes were 0.28–0.39 in absolute value — small to moderate.1
- FWE correction failure: the regional pattern is suggestive and replicates in jackknife sensitivity analyses (14–15 of 17 datasets), but the strictest multiple-comparisons threshold did not hold.1
- 3 neurotransmitter systems: spatial-correlation analysis using JuSpace neurotransmitter atlases showed PPD-related activity changes co-localized with serotonergic (5-HT1a, 5-HT1b, 5-HT2a, 5-HT4, SERT), dopaminergic (D1, D2, DAT, FDOPA), and vesicular acetylcholine transporter (VAChT) maps.1
- Ion-channel enrichment: genes whose expression patterns spatially correlated with the PPD functional map were enriched for inorganic ion transmembrane transport, ion-gated channel activity, and cation channel complexes — a different angle than the usual hormone-or-monoamine framing.1
Postpartum depression (PPD) affects roughly 17% of new mothers globally, with substantial impact on mothers, infants, and families.2 Diagnosis is clinical — depressive episode within 4 weeks postpartum (DSM-5) or up to 12 months (ICD-11) — but mechanistic biology remains unsettled. Hormone-withdrawal models, neuroinflammation, sleep deprivation, and stress-axis dysregulation each have supportive data; none have been definitive.3
Imaging has been a recurring frustration. Individual studies often find regional differences in PPD vs. controls, but the regions don’t replicate across studies. The Chen et al. meta-analysis is the first to pool the resting-state literature with consistent voxel-wise methods, identify the regions most likely to be real, and link those regions to neurotransmitter and gene-expression maps.
Voxel-Based Meta-Analysis: What It Is and What It Cannot Do
The classical problem with fMRI meta-analysis is that individual studies report peak coordinates of significant clusters, not whole-brain effect-size maps. Seed-based d Mapping with Permutation of Subject Images (SDM-PSI) — the tool used here — reconstructs effect-size maps from peak coordinates plus reported t-values, weights them by sample size and within-study variability, and pools them in a random-effects model.1
The approach lets researchers ask “what regional pattern shows up across studies?” rather than “which study found which region?” It also generates jackknife sensitivity analyses — remove 1 study at a time, rerun the meta — that flag findings driven by single outlier studies.
What it cannot do: rescue underpowered individual studies. If the underlying literature is uniformly underpowered, the meta-analysis pools weak signals into a slightly less weak signal but does not manufacture statistical certainty. The Chen meta’s failure to survive FWE correction across 12 studies and 475 patients is a useful calibration: even pooled, the resting-state PPD literature does not produce strong, region-specific signals at the strict-correction bar.
The 4 Regions That Repeat Across PPD Studies
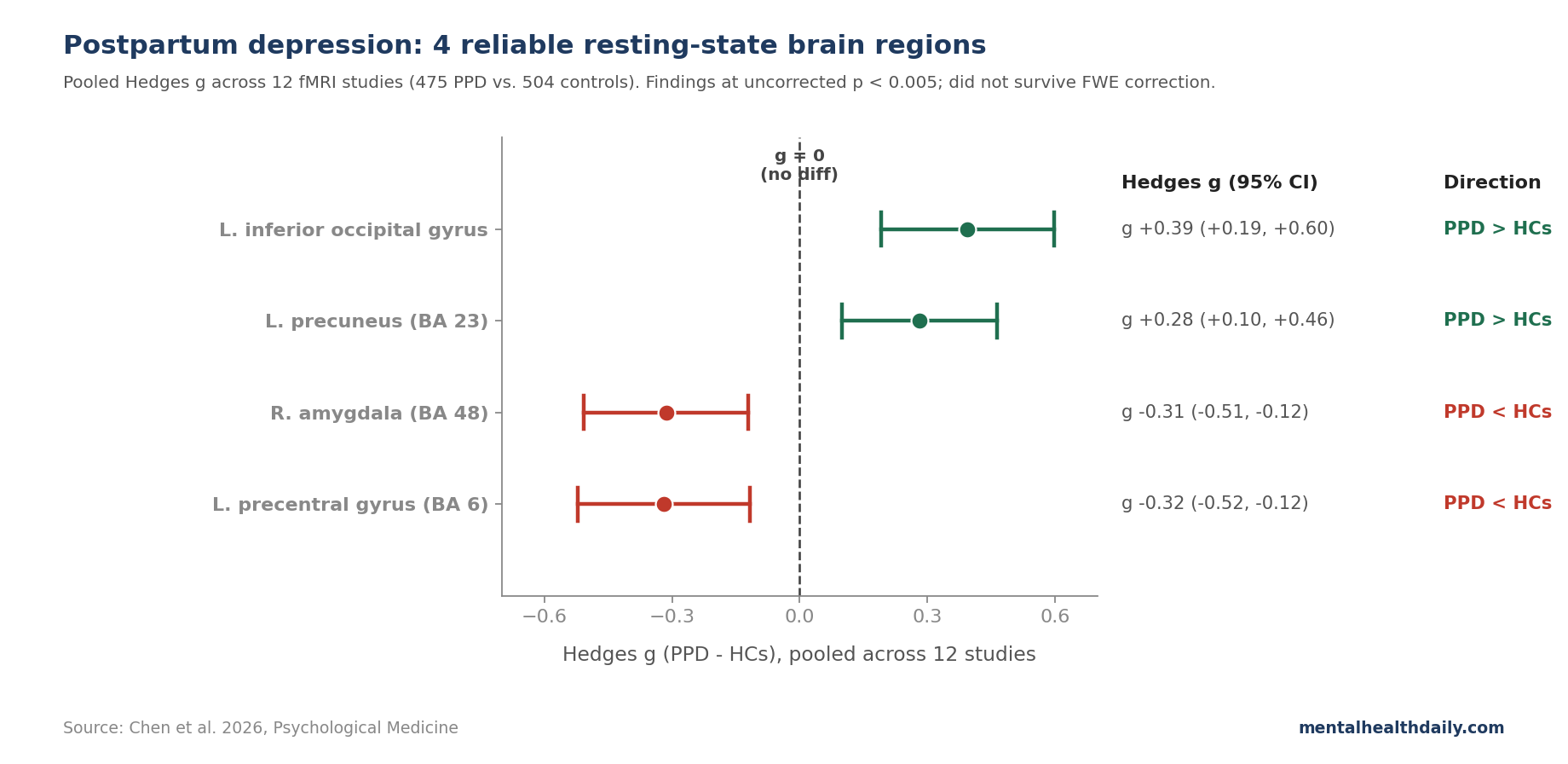
Left inferior occipital gyrus (BA 18): increased activity in PPD. Hedges’ g = 0.39 (95% CI 0.19–0.60), low heterogeneity (I² = 15.7%), no publication bias on Egger’s test (p = 0.96), survived 15 of 17 jackknife resamplings. The largest cluster in the meta-analysis at 202 voxels.1
The occipital finding is interesting and counterintuitive. Vision is not where most PPD theories live. Possible interpretations include altered visual processing of infant faces or emotional stimuli, increased baseline sensory gain in major depressive states more broadly, or a marker of altered attentional engagement.
Left precuneus (BA 23): increased activity in PPD. Hedges’ g = 0.28, low heterogeneity, survived 14 of 17 resamplings. The precuneus is a core node of the default mode network — the set of midline regions active during self-referential thinking and rumination. Increased default-mode activity is a recurring finding in major depression more broadly.4
Right amygdala (BA 48): decreased activity in PPD. Hedges’ g = −0.31. The amygdala is the canonical fear/threat-processing region, and the direction here is opposite the usual depression imaging finding, where amygdala reactivity is often elevated to negative stimuli during task fMRI.
The discrepancy may reflect resting-state vs. task-state distinction, or a different state in PPD specifically — possibly reflecting blunted maternal threat-monitoring rather than the heightened threat-monitoring seen in classical depression.
Left precentral gyrus (BA 6): decreased activity in PPD. Hedges’ g = −0.32. The precentral gyrus is primary motor cortex, and reduced resting-state activity there in PPD has been reported in individual studies but its functional meaning is unclear. Possible links include psychomotor slowing (a depression hallmark) or maternal-care motor planning differences.
Spatial Overlap with Serotonin, Dopamine, and Acetylcholine Maps
The transcriptomic-and-neurotransmitter side of the analysis uses a different logic. Researchers have built atlases of where serotonin, dopamine, and acetylcholine receptors and transporters are densest in the brain, derived from PET and SPECT studies in healthy populations. JuSpace takes the meta-analytic functional map and asks whether its spatial pattern correlates with each neurotransmitter atlas.5
This does not show that PPD is caused by serotonergic or dopaminergic dysfunction; it shows that the regions where PPD differs from controls happen to be regions densely innervated by those systems. That is suggestive but not mechanistic.
The PPD functional pattern showed FDR-corrected spatial overlap with:
- Serotonergic targets: 5-HT1a, 5-HT1b, 5-HT2a, 5-HT4 receptors, and the serotonin transporter (SERT).
- Dopaminergic targets: D1 and D2 receptors, dopamine transporter (DAT), and FDOPA (a marker of dopamine synthesis capacity).
- Cholinergic targets: vesicular acetylcholine transporter (VAChT).
The serotonin overlap is consistent with SSRIs being first-line pharmacotherapy in PPD — mechanism aligns with treatment, even if neither is fully understood.6 The dopamine and acetylcholine overlaps are less commonly emphasized in PPD discussions but consistent with broader depression neurobiology.
The Ion-Channel Story Is Less Familiar
The transcriptomics-and-neuroimaging analysis used the Allen Human Brain Atlas (AHBA), which provides whole-brain microarray gene expression data from 6 postmortem brains, mapped onto MNI coordinates. Researchers ran partial least-squares regression to find the gene expression pattern most correlated with the PPD meta-analytic functional map, then submitted the top genes to enrichment analysis.1
The first PLS component (PLS-1) explained 21.4% of the variance in PPD functional divergence (p = 0.011 after spatial-autocorrelation correction). Genes loading on PLS-1 enriched for:
- Biological processes: inorganic ion transmembrane transport.
- Molecular functions: ion-gated channel activity, substrate-specific channel activity, cation channel activity, passive transmembrane transporter activity.
- Cellular components: ion channel complex, transmembrane transporter complex, cation channel complex.
This is a different angle than the standard hormone-and-monoamine framing of PPD. Ion channels regulate neuronal excitability, including how easily brain cells fire and how strongly inhibitory or excitatory signals pass through a circuit.
Ion-channel dysfunction is implicated in major depression more broadly — including in the rapid antidepressant effect of ketamine, which acts on glutamate-related ion channels, and in the suspected mechanism of brexanolone (a neurosteroid GABA-A modulator approved specifically for PPD in 2019).7
The Chen finding does not say PPD is “caused by ion channel mutations.” It says that the regional pattern of brain dysfunction in PPD spatially aligns with where ion-channel-related genes are most expressed — consistent with the idea that the same channels matter for whichever excitability shifts are happening in PPD brains.
Hormone, Sleep, and Inflammation Models Converge With the Imaging Pattern
The classical hormone-withdrawal model, articulated by Schiller et al. 2015 and others, posits that the rapid drop in estradiol and progesterone after delivery destabilizes monoamine and GABA systems in vulnerable women.8 The neurosteroid allopregnanolone — a progesterone metabolite that potentiates GABA-A receptors — falls precipitously postpartum, and exogenous allopregnanolone analogs (brexanolone IV in 2019, zuranolone oral in 2023) are FDA-approved for PPD on the strength of this model.7
Stress-axis and sleep-deprivation models add layers. The hypothalamic-pituitary-adrenal (HPA) axis recalibrates around delivery; chronic sleep disruption from infant care interacts with stress reactivity. Inflammatory mechanisms have also been proposed, with elevated IL-6 and CRP showing some association with depressive symptoms in pregnancy and postpartum.9
The Chen meta-analysis adds 2 things to this picture:
- Regional specificity at the imaging level. If you want to know where PPD-related brain differences are most likely to show up, the amygdala, precuneus, occipital cortex, and precentral cortex are the best meta-analytic candidates — but only at uncorrected thresholds.
- Cross-modal alignment. The functional pattern overlaps with monoamine and acetylcholine systems and with ion-channel-related gene expression. That convergence supports rather than refutes the existing pharmacology (SSRIs targeting serotonin; brexanolone/zuranolone targeting GABA-A through neurosteroid mechanisms).
Limitations of the Chen Synthesis
Findings did not survive FWE correction. This is the most important caveat. At the conventional uncorrected p < 0.005 with cluster extent > 10 voxels, 4 regions emerge reliably. At the more conservative family-wise error correction across the whole brain, none survive.
SDM developers argue uncorrected thresholds with cluster extents are acceptable in voxel-based meta-analysis, but the gap between uncorrected and corrected results means the regional pattern should be treated as a candidate for replication, not as confirmed.1
Effect sizes are small to moderate. Hedges’ g of 0.28–0.39 means the average PPD patient differs from the average control by about a quarter to a third of a standard deviation in regional resting-state activity. That is not the kind of effect that lets you diagnose PPD from an MRI scan.
Heterogeneity in imaging methods. The meta-analysis pools ALFF, fALFF, ReHo, VMHC, degree centrality, and cerebral blood flow studies. These measure related but not identical aspects of resting-state activity. Combining them gains power but blurs interpretation.
Sample skew toward Chinese cohorts. Multiple included studies were Chinese; the AHBA gene expression data is from 6 mostly Western postmortem brains. Generalizability across populations is unknown.
Cross-sectional, observational. The meta cannot distinguish brain changes that precede PPD, occur during PPD, or are consequences of PPD. Longitudinal imaging from pregnancy through postpartum is sparse.
Medication-naive sample. Including only untreated patients is a strength for mechanism but limits generalizability to treated PPD — the population most clinicians are working with.
What This Meta Means for Patients and Clinicians
- The biology is real but diffuse. PPD has a measurable neural signature, but it is small, distributed across multiple regions, and not strong enough to support imaging-based diagnosis. Treat clinical assessment (Edinburgh Postnatal Depression Scale, structured interview) as the primary tool.
- SSRIs and brexanolone/zuranolone target real biology. The serotonergic spatial-overlap finding aligns with first-line SSRI use in PPD; the neurosteroid-GABA-A and ion-channel angle aligns with the brexanolone/zuranolone mechanism. Both are evidence-based options.6,7
- Don’t over-read individual fMRI findings. If you see a single PPD imaging study claiming a specific region matters, this meta-analysis is the right context: 12 studies and 475 patients pooled barely produce regional differences at strict correction. Single-study claims should be treated as preliminary.
- Practical care still leads with proven treatments. Cognitive-behavioral therapy, interpersonal therapy, SSRIs, brexanolone/zuranolone for severe cases, social support, sleep optimization, and lactation-compatible medication selection where relevant. The biology informs the field; it does not yet inform individual care decisions.
Questions About Postpartum Depression and the Brain
Does postpartum depression show up on a brain scan?
Not reliably enough to use diagnostically. The 12-study, 475-patient meta found regional differences at uncorrected statistical thresholds — meaningful for understanding mechanism but with effect sizes too small (Hedges’ g around 0.3) and too distributed for individual diagnosis.1
Clinical screening (Edinburgh Postnatal Depression Scale, structured interview) remains the diagnostic standard.
What brain regions are involved?
The reliable regional candidates from this meta-analysis are increased resting activity in the left precuneus and left inferior occipital gyrus, and decreased activity in the right amygdala and left precentral gyrus.1
The precuneus is part of the default mode network involved in self-referential thinking. The amygdala mediates threat processing. The precentral gyrus is motor cortex. The occipital finding is the most surprising and least understood.
What about hormones and PPD?
The hormone-withdrawal hypothesis — that the steep postpartum drop in estradiol, progesterone, and the GABA-A-modulating neurosteroid allopregnanolone destabilizes mood in vulnerable women — is still the most influential mechanistic model.8
Brexanolone (IV) and zuranolone (oral) are FDA-approved neurosteroid analogs that target this system specifically. The Chen meta’s ion-channel gene-enrichment finding fits with this picture, since allopregnanolone acts on GABA-A receptor ion channels.
How effective are SSRIs in postpartum depression?
SSRIs (sertraline, paroxetine, fluoxetine, escitalopram) are first-line pharmacotherapy and have RCT evidence comparable to general adult depression: effect sizes around SMD 0.3–0.5 vs. placebo on standard depression scales.6
Sertraline and paroxetine are the most studied for breastfeeding compatibility (lower transfer to breast milk). The serotonergic spatial-overlap finding in the Chen meta-analysis aligns with this established pharmacology.
What is brexanolone vs. zuranolone?
Brexanolone (Zulresso) is a synthetic allopregnanolone given as a 60-hour IV infusion. Zuranolone (Zurzuvae) is an oral analog approved in 2023 for adult PPD, taken once daily for 14 days. Both target GABA-A receptors and have shown rapid antidepressant effects in PPD trials.7
Zuranolone is more practically usable than brexanolone (no inpatient infusion required), and its 2023 approval expanded the PPD-specific pharmacotherapy toolkit beyond SSRIs.
What if I think I have postpartum depression?
Talk to your obstetrician, primary care provider, or a mental health professional. The Edinburgh Postnatal Depression Scale is a validated 10-item self-report screen that can flag the need for evaluation. Effective treatments exist.
In the United States, the Postpartum Support International helpline (1-800-944-4773) offers nonurgent guidance. For acute crisis, the 988 Suicide & Crisis Lifeline is available 24/7.
References
- Intrinsic regional brain activity differences and its relationship with neurotransmitter and gene expression in postpartum depression: a voxel-based meta-analysis. Chen G et al. Psychological Medicine. 2026;56:e110. doi:10.1017/S0033291726103651
- Mapping global prevalence of depression among postpartum women. Wang Z et al. Translational Psychiatry. 2021;11(1):543. doi:10.1038/s41398-021-01663-6
- Postpartum depression. Stewart DE & Vigod SN. New England Journal of Medicine. 2016;375(22):2177-2186. doi:10.1056/NEJMcp1607649
- Default-mode brain dysfunction in mental disorders: a systematic review. Whitfield-Gabrieli S & Ford JM. Annual Review of Clinical Psychology. 2012;8:49-76. doi:10.1146/annurev-clinpsy-032511-143049
- JuSpace: a tool for spatial correlation analyses of magnetic resonance imaging data with nuclear imaging derived neurotransmitter maps. Dukart J et al. Human Brain Mapping. 2021;42(3):555-566. doi:10.1002/hbm.25244
- Antidepressant treatment for postnatal depression. Brown JVE et al. Cochrane Database of Systematic Reviews. 2021;2(2):CD013560. doi:10.1002/14651858.CD013560.pub2
- Zuranolone for the treatment of postpartum depression. Deligiannidis KM et al. American Journal of Psychiatry. 2023;180(9):668-675. doi:10.1176/appi.ajp.20220785
- The role of reproductive hormones in postpartum depression. Schiller CE, Meltzer-Brody S & Rubinow DR. CNS Spectrums. 2015;20(1):48-59. doi:10.1017/S1092852914000480
- Inflammation and clinical depression: the immunocytokine model. Maes M et al. Neuropsychobiology. 2011;65(1):1-12. doi:10.1159/000329995