A 2026 network meta-analysis of 57 randomized trials involving 5,675 cancer survivors found that exercise helped several survivorship symptoms, but the strongest signal depended on the symptom: mind-body exercise ranked highest for cancer-related fatigue, aerobic training ranked highest for health-related quality of life, and combined aerobic plus resistance training led physical-function outcomes.1
Research Highlights
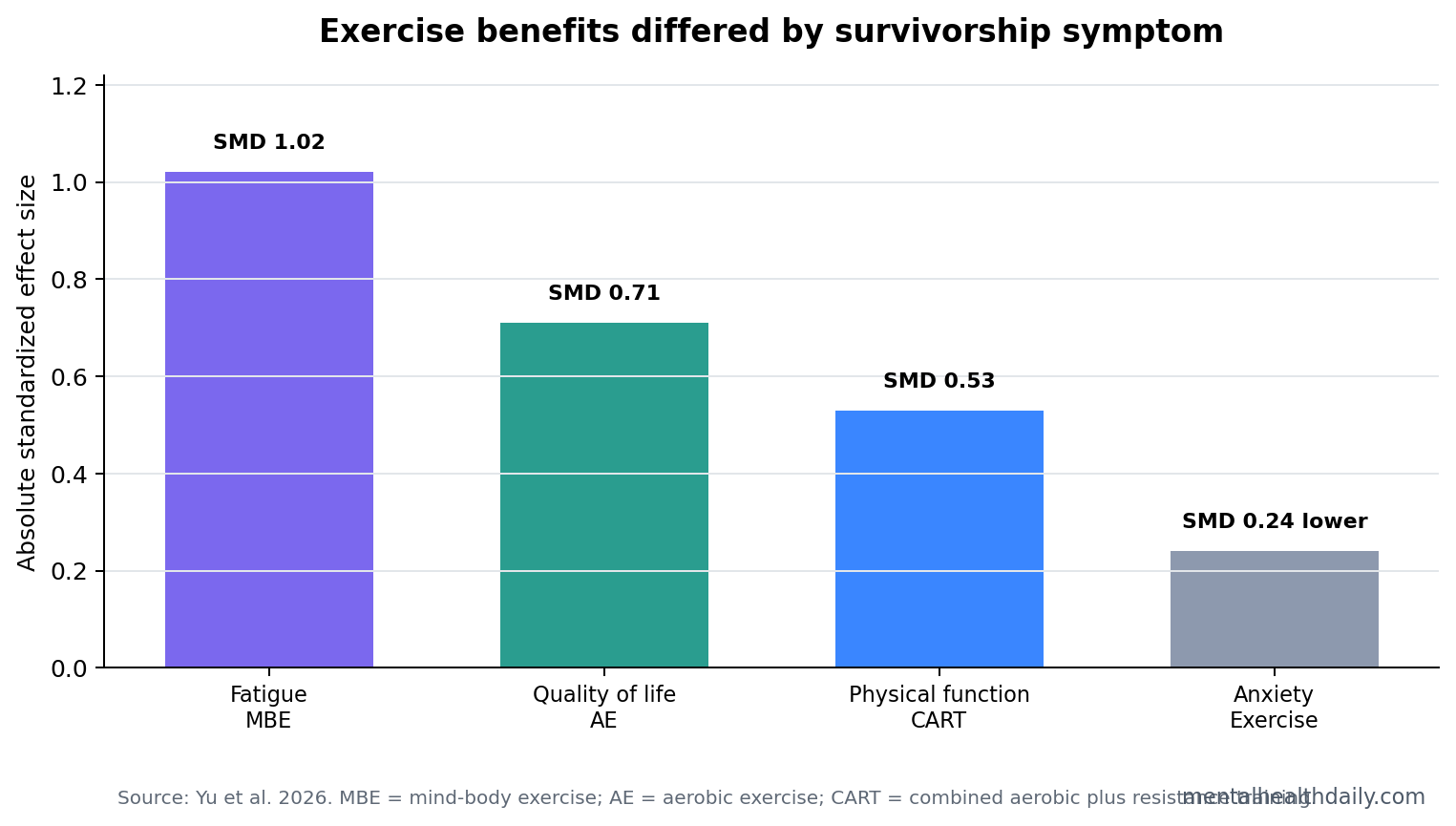
- Fatigue ranking favored mind-body exercise: mind-body exercise showed the largest fatigue estimate vs. usual care (SMD = 1.02, 95% CrI 0.53 to 1.51; P-score = 0.97), but fatigue heterogeneity was high (I² = 90.9%).1
- Quality of life favored aerobic training: aerobic exercise improved health-related quality of life (SMD = 0.71, 95% CrI 0.37 to 1.06; P-score = 0.92).1
- Physical function favored combined training: combined aerobic plus resistance training improved patient-reported function (SMD = 0.53, 95% CrI 0.29 to 0.76) and cardiorespiratory fitness (SMD = 0.55, 95% CrI 0.14 to 0.96).1
- Mood effects were modest: depression estimates were directionally favorable but not individually significant, while anxiety improved modestly in 11 studies (SMD = −0.24, 95% CI −0.47 to −0.01).1
- Guidelines already support exercise: the new contribution is not that exercise works, but that 57 trials can be organized into symptom-specific choices instead of one generic recommendation.2,3
Cancer-related fatigue is persistent tiredness tied to cancer or cancer treatment that is not fully relieved by rest. It overlaps with sleep disruption, inflammation, deconditioning, pain, anemia, mood symptoms, and treatment burden, so a single exercise format is unlikely to dominate every survivor and every outcome.
Network meta-analysis is a statistical method that combines direct trial comparisons with indirect comparisons through shared control groups. That lets researchers rank treatments even when every possible head-to-head trial has not been run. The tradeoff is that rankings become fragile when studies differ sharply in cancer type, treatment stage, exercise dose, control condition, and outcome scale.
Mind-Body Exercise Had the Largest Fatigue Estimate
Yu et al. found the largest fatigue estimate for mind-body exercise, a category that included practices such as yoga, qigong, and related movement-attention formats. The estimate was large: SMD = 1.02 vs. usual care, with a 95% credible interval from 0.53 to 1.51.1 A standardized mean difference (SMD) expresses change in units of pooled standard deviation, so a value near 1.0 is large by conventional meta-analysis language.
That large fatigue estimate needs calibration. The fatigue network had I² = 90.9%, meaning trial results varied widely beyond chance, and the usual-care vs. mind-body loop showed major inconsistency (Q = 253.92, p < 0.0001). Point estimates favor mind-body exercise for fatigue, but the evidence is not clean enough to treat yoga or qigong as universally superior.
Aerobic Training Was the Strongest Quality-of-Life Signal
Aerobic exercise ranked first for health-related quality of life, with SMD = 0.71 vs. usual care and P-score = 0.92.1 Health-related quality of life means the survivor’s overall perceived physical, emotional, and social functioning across daily life, beyond tumor status or laboratory health.
The aerobic result is clinically plausible. Walking, cycling, treadmill programs, and similar conditioning work can improve cardiorespiratory tolerance, daily energy, and confidence in movement. Those are exactly the domains that tend to shape global quality-of-life scores after cancer treatment.
Combined Training Best Matched Physical Function
Combined aerobic plus resistance training had the broadest physical-function profile. It improved patient-reported physical functioning (SMD = 0.53, 95% CrI 0.29 to 0.76) and objective cardiorespiratory fitness (SMD = 0.55, 95% CrI 0.14 to 0.96).1
- Aerobic work: targets endurance, oxygen use, and daily exertion tolerance.
- Resistance training: targets strength, muscle loss, and functional reserve.
- Combined training: fits survivors whose main problem is physical limitation rather than fatigue alone.
Depression and Anxiety Signals Were More Modest
Depression outcomes were directionally favorable across modalities, but no single exercise type clearly separated from the rest. Aerobic exercise had the largest depression estimate vs. usual care (SMD = 0.43), but its credible interval crossed the null (−0.03 to 0.88).1
Anxiety had a smaller but statistically significant pairwise signal across 11 studies: SMD = −0.24, 95% CI −0.47 to −0.01. That is a real average reduction, not a strong guarantee. The prediction interval crossed zero, so future settings may find smaller, absent, or occasionally opposite effects.
Exercise Prescriptions Should Start With the Dominant Symptom
Campbell et al. already concluded that exercise can help fatigue, anxiety, depressive symptoms, and quality of life in cancer survivors.2 Mustian et al. found exercise and psychological interventions outperformed medication approaches for cancer-related fatigue in a large comparative meta-analysis.3 Yu et al. add a ranking layer: the first choice should be guided by the symptom the survivor most wants to change.
- Fatigue-dominant presentation: mind-body exercise is a reasonable first option when access, preference, and safety fit, with aerobic or combined training still defensible.
- Quality-of-life priority: aerobic exercise has the clearest ranking signal.
- Physical deconditioning: combined aerobic plus resistance training best matches the outcome.
- Anxiety or depression priority: exercise can be part of care, but modality-specific claims are weaker than for fatigue or function.
Evidence Strength Depends on the Outcome
Evidence-strength note: this was a broad network meta-analysis, not a direct head-to-head trial of every exercise format. It can rank likely choices across a heterogeneous trial literature. It cannot tell a specific survivor that one modality will outperform another in their cancer type, treatment phase, baseline fitness level, or symptom cluster.
Implementation still depends on screening, supervision, and adherence. A survivor who will not attend yoga will not benefit from yoga’s ranking. A survivor with marked deconditioning may need combined training even if fatigue is present. Optimal care starts with the data, then adapts to access, safety, preference, and the symptom being treated.
Why the Ranking Should Not Become a Rigid Ladder
The ranking is most useful when it is read as a starting map, not a fixed hierarchy. Network meta-analysis can rank treatments even without many direct head-to-head trials, but the ranking inherits every difference across trials: cancer type, treatment stage, baseline fatigue, supervision, session length, intensity, adherence, and control-group quality.
Clinical implication: start with the symptom-matched option, then adjust quickly if the intervention does not fit the survivor’s body or life. A fatigued survivor who enjoys yoga may be well matched to mind-body exercise. A survivor whose main problem is stairs, shopping, or returning to work may need combined aerobic and resistance training. A survivor whose goal is global quality of life may reasonably begin with aerobic conditioning.
Depression and Anxiety Need a Different Threshold for Claims
The mood outcomes should be read more conservatively than the fatigue and quality-of-life outcomes. Depression estimates leaned in the expected direction but did not clearly separate modalities. Anxiety improved on average, but the pooled effect was small and the prediction interval crossed zero. That pattern supports exercise as a useful adjunct, not as a stand-alone mental-health treatment.
Two overstatements to avoid: the first is the wellness claim that any exercise prescription reliably treats anxiety or depression after cancer. The second is the nihilistic claim that modest effects are meaningless.
A small average anxiety reduction can matter when exercise also improves fatigue, physical function, sleep regularity, and self-efficacy. It just should not be sold as a substitute for psychotherapy, medication, pain control, or sleep treatment when those are clinically indicated.
Adherence Decides Whether the Ranking Survives Contact With Care
Exercise trials can make modalities look cleaner than survivorship care actually is. Transportation, neuropathy, anemia, fear of injury, lymphedema concerns, pain, depression, and work schedules all change adherence. The best-ranked modality is only useful if the survivor can do it often enough to receive the biological and psychological dose.
Supervision also changes the meaning of a program. A monitored hospital or research-session intervention is not the same as an unsupervised home plan, especially for survivors with cardiopulmonary limits, balance problems, or severe post-treatment fatigue.
That makes shared decision-making part of the evidence, not a soft add-on. If mind-body exercise is best for fatigue on paper but the patient strongly prefers walking, aerobic training may be the better first prescription. If aerobic exercise is best for quality of life but weakness is the limiting symptom, combined training may be more rational.
Questions About Exercise for Cancer Fatigue and Mood
Did mind-body exercise clearly beat all other exercise types for fatigue?
No. It had the largest estimate and highest ranking, but the fatigue network had high heterogeneity and important inconsistency. Point estimates support mind-body exercise as a strong option, not a universal winner.
Should cancer survivors do aerobic exercise instead?
If quality of life is the priority, aerobic exercise had the strongest result. If fatigue is the main problem, mind-body exercise may be a good starting point. If physical function is the main problem, combined aerobic plus resistance training fits better.
Can exercise replace mental-health treatment for depression or anxiety after cancer?
No. Exercise showed modest mood benefits, especially for anxiety, but the evidence does not support replacing psychotherapy, medication, sleep treatment, pain care, or social support when those are needed.
References
- Yu J, et al. Comparative efficacy of different exercise interventions for cancer-related fatigue, health-related quality of life, anxiety and depression symptoms in cancer survivors: a systematic review and network meta-analysis. BMC Public Health. 2026. https://doi.org/10.1186/s12889-026-27420-2
- Campbell KL, et al. Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Medicine & Science in Sports & Exercise. 2019. https://doi.org/10.1249/mss.0000000000002116
- Mustian KM, et al. Comparison of Pharmaceutical, Psychological, and Exercise Treatments for Cancer-Related Fatigue: A Meta-analysis. JAMA Oncology. 2017. https://doi.org/10.1001/jamaoncol.2016.6914
- Singh B, et al. Exercise oncology: a comprehensive review. CA: A Cancer Journal for Clinicians. 2018. https://doi.org/10.3322/caac.21457