A 2026 scoping review screened 174 records and found 7 human studies linking sleep bruxism with gastroesophageal reflux disease.1 The signal was consistent but messy: case-control studies reported roughly 5- to 6-fold higher odds of bruxism with GERD, while instrumental studies suggested reflux episodes, arousals, swallowing, and jaw-muscle bursts may cluster during sleep.
Research Highlights
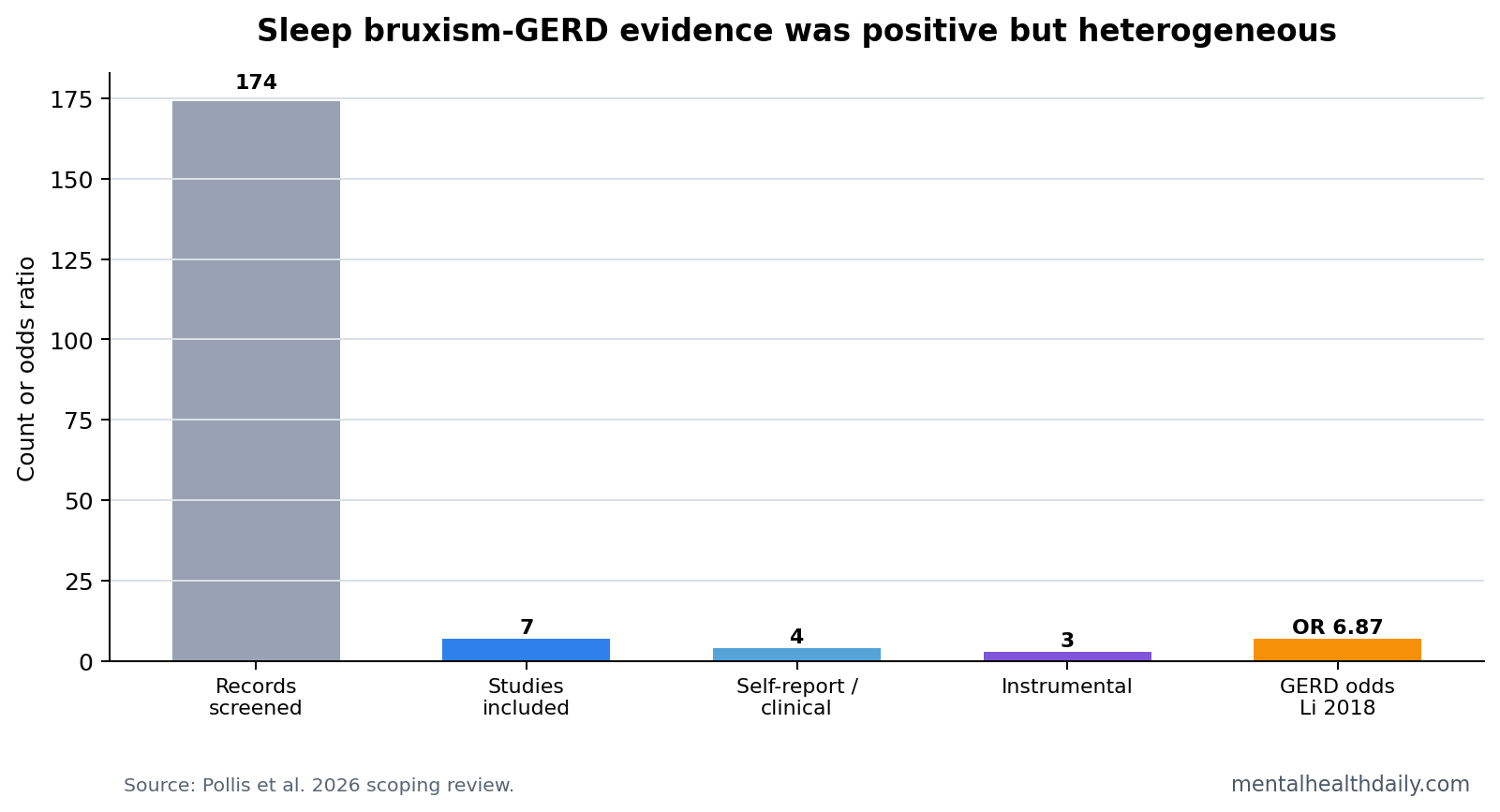
- 7 studies made the final review: Pollis et al. screened 174 records, retrieved 11 full texts, and included 7 studies.1
- Every included study was positive: The review found 4 self-report/clinical studies and 3 instrumental studies, all reporting a sleep bruxism-GERD link.1
- Case-control odds were large: GERD was associated with bruxism at OR 5.30, 95% CI 2.62 to 10.70, and OR 6.87, 95% CI 4.34 to 10.88, in 2 Li studies.1
- Instrumental studies supported timing: In 1 pH/EMG study, reflux episodes averaged 0.5 vs. 0.0 per hour in bruxism vs. controls.1
- Causality stayed unresolved: The review could not determine whether GERD triggers bruxism, bruxism protects against reflux injury, or both arise from 3-second sleep micro-arousals.1
Sleep bruxism is rhythmic or sustained jaw-muscle activity during sleep, often noticed as tooth grinding or clenching. Modern dental sleep medicine no longer treats it as a disorder in every case; it can be harmful, neutral, or possibly protective depending on context.
Gastroesophageal reflux disease (GERD) involves backward movement of stomach contents into the esophagus and sometimes the throat or mouth. During sleep, reflux can trigger arousal, swallowing, salivation, coughing, and changes in breathing or muscle tone.
7 Studies Linked Sleep Bruxism With GERD, but Methods Varied
Pollis et al. included 7 studies after screening 174 records. Four studies relied on self-report or clinical bruxism assessment, while 3 used instrumental assessment such as electromyography, polysomnography, esophageal pH monitoring, or endoscopy-linked reflux evaluation.1
The heterogeneity is the main reason the review should be read carefully. A questionnaire-defined bruxism case is not the same as a polysomnography-confirmed rhythmic masticatory muscle activity case. Symptom-defined GERD is not the same as overnight pH-metry.
GERD Was Associated With 5- to 6-Fold Higher Bruxism Odds
The self-report and clinical studies were directionally consistent. Li et al. reported GERD-bruxism associations of OR 5.30, 95% CI 2.62 to 10.70, and OR 6.87, 95% CI 4.34 to 10.88. Mengatto et al. reported adjusted OR 6.58, 95% CI 1.40 to 30.98.1
Those odds ratios are large, but they should not be mistaken for proof that reflux causes tooth grinding. People with reflux may sleep poorly, wake more often, report more symptoms, or have other health factors that increase bruxism detection.
Reflux Episodes May Trigger Jaw-Muscle Activity Through Arousal and Swallowing
The mechanistic studies are more interesting than the questionnaire associations. In 2003, Miyawaki et al. reported that the bruxism group had more gastroesophageal reflux episodes than controls, averaging 0.5 vs. 0.0 episodes per hour, and spent more sleep time in reflux, 3.6% vs. 0.1%.1
Rhythmic masticatory muscle activity (RMMA) is the jaw-muscle burst pattern often used as the physiological marker of sleep bruxism. Reflux may provoke arousal and swallowing, and those arousal sequences can end in RMMA. In that model, bruxism may be part of a sleep-protective response to acid exposure.
- Protective model: jaw activity and swallowing increase saliva and may help clear acid.
- Shared-arousal model: reflux and bruxism both ride on sleep fragmentation and sympathetic activation.
- Dental-risk model: even if bruxism has a protective origin, repeated grinding can still damage teeth and worsen jaw pain.
Acid Suppression Results Hint at Mechanism but Do Not Settle Treatment
Two instrumental studies reported that proton pump inhibitor treatment reduced EMG bursts or RMMA episodes. That fits the reflux-trigger model: if less acid reaches the esophagus, fewer reflux-linked arousals and jaw-muscle episodes should occur.
Evidence-strength note: the review was a scoping review, not a pooled meta-analysis. The included studies were few, heterogeneous, and often small. The evidence supports screening for GERD symptoms in selected sleep-bruxism patients, especially when dental erosion, cough, throat symptoms, or nocturnal reflux symptoms are present. It does not support treating every bruxism case with acid suppression.
Dental Sleep Medicine Needs Both Directions of the Question
Sleep bruxism can damage teeth, restorations, jaw muscles, and temporomandibular joints. GERD can erode enamel chemically through acid exposure. When they appear together, mechanical wear and chemical wear can be mistaken for one problem unless the clinician asks about both.
Dental clue: erosion patterns, sour taste, chronic throat clearing, morning cough, or reflux history should make GERD part of the bruxism workup. A night guard may protect teeth from mechanical forces, but it does not treat acid reflux reaching the esophagus or mouth.
Sleep clue: repeated awakenings, choking sensations, supine worsening, snoring, witnessed apneas, and daytime sleepiness should broaden the evaluation beyond tooth grinding. Sleep apnea, reflux, and bruxism can cluster through arousal physiology, and treating only the jaw can leave the sleep trigger untouched.
Bruxism May Be Harmful and Protective in Different Moments
The review’s most useful conceptual move is separating bruxism as a behavior from bruxism as a disease. A jaw-muscle burst after reflux may increase saliva and swallowing, helping clear acid. Repeated bursts across months or years can still wear teeth and worsen jaw pain.
Those 2 claims can both be true. A short-term protective reflex can become a long-term dental problem. The clinical task is to identify the driver: reflux exposure, sleep fragmentation, stress physiology, medication effects, sleep apnea, or a primary bruxism pattern.
- Reflux-dominant pattern: nocturnal heartburn, sour taste, throat symptoms, dental erosion, or pH evidence.
- Arousal-dominant pattern: frequent awakenings, sympathetic activation, sleep apnea symptoms, or insomnia.
- Jaw-dominant pattern: morning jaw soreness, masseter hypertrophy, tooth wear without reflux clues, or daytime clenching.
Better Studies Need Simultaneous Sleep, pH, and Muscle Recording
The field needs designs that measure reflux and bruxism at the same time. Self-report can identify people worth testing, but it cannot show whether acid exposure came before the jaw-muscle burst, after it, or in an unrelated part of the night.
The strongest design would combine polysomnography, masseter EMG, esophageal pH-impedance monitoring, body position, sleep-stage scoring, respiratory-event scoring, and symptom diaries. That would let researchers test whether reflux episodes, micro-arousals, swallowing, RMMA, and tooth-grinding sounds follow a consistent sequence.
Without that timing data, GERD and bruxism remain associated conditions with plausible bidirectional mechanisms. With timing data, clinicians could decide who needs reflux treatment, who needs sleep-disorder workup, who needs dental protection, and who needs a combination.
What Patients Should Not Infer From the Association
The review does not say that stress is irrelevant, that every night guard is inadequate, or that reflux medication is the answer to tooth grinding. It says GERD belongs on the differential when the symptom pattern points there.
Practical screening: a bruxism history should include reflux symptoms, sour taste, nocturnal cough, throat irritation, dental erosion, alcohol timing, late meals, body position, sleep apnea symptoms, and medications that affect sleep or saliva. A reflux history should include tooth wear, morning jaw soreness, partner-reported grinding, and sleep fragmentation.
That bidirectional screen is useful because patients rarely organize symptoms by specialty. A dentist may see enamel erosion and worn teeth. A gastroenterologist may hear nocturnal reflux. A sleep clinician may see arousals. The GERD-bruxism connection is most visible when those observations are put in the same timeline.
The treatment sequence should follow that timeline. If reflux symptoms clearly precede grinding episodes, reflux management and sleep-position changes may be reasonable before escalating jaw-focused interventions. If grinding occurs without reflux clues, dental protection, stress/sleep assessment, medication review, and sleep-apnea screening may be higher yield.
Timing is the hinge: the same patient can have reflux, arousals, and jaw-muscle bursts in one night, but treatment logic changes when reflux reliably comes first vs. when grinding appears independent of acid exposure. That is why pH-impedance testing, sleep recording, and symptom timing matter more than a single label such as “stress grinding” or “reflux bruxism.”
Either way, the review supports a broader intake form. Bruxism and GERD live at the boundary of dentistry, sleep medicine, gastroenterology, and behavioral health, so narrow specialty-only questioning misses the pattern the scoping review was built to map.
The strongest practical conclusion is simple: grinding during sleep should prompt reflux questions, and nocturnal reflux should prompt bruxism questions. That does not diagnose either condition, but it prevents a common blind spot.
It also keeps treatment from becoming narrower than the night-time physiology patients actually experience.
Questions About Sleep Bruxism and GERD
Can reflux cause tooth grinding?
It may contribute in some people. The strongest model is reflux-related arousal and swallowing leading to jaw-muscle activity during sleep.
Does bruxism protect the esophagus?
Possibly in some episodes. Jaw activity can increase saliva and swallowing, which may help clear acid. Bruxism can still damage teeth, irritate jaw muscles, and worsen orofacial pain.
Should someone with sleep bruxism try a proton pump inhibitor?
Only when GERD is clinically suspected or diagnosed. The review does not support using acid suppression as a blanket bruxism treatment.
References
- Pollis M, et al. Sleep Bruxism and Gastroesophageal Reflux Disease: A Scoping Review. Nature and Science of Sleep. 2026. doi:10.2147/nss.s574762
- Li Y, et al. Gastroesophageal reflux symptoms and bruxism case-control studies. PubMed
- Miyawaki S, et al. Sleep bruxism, esophageal pH, and rhythmic masticatory muscle activity. PubMed
- Ohmure H, et al. Proton pump inhibitor effects on sleep bruxism and reflux-related RMMA. PubMed