A 2026 arterial spin labeling MRI study found that 34 patients with non-auditory tinnitus and cerebral venous congestion had lower corrected cerebral blood flow across multiple brain regions than venous-congestion patients without tinnitus and healthy controls.1 Compared with those 2 groups, the tinnitus group had poorer sleep quality, higher depression scores, and slightly lower cognitive scores.
Research Highlights
- 87 people were scanned: The study compared 34 venous-congestion patients with non-auditory tinnitus, 17 venous-congestion patients without tinnitus, and 36 healthy controls.1
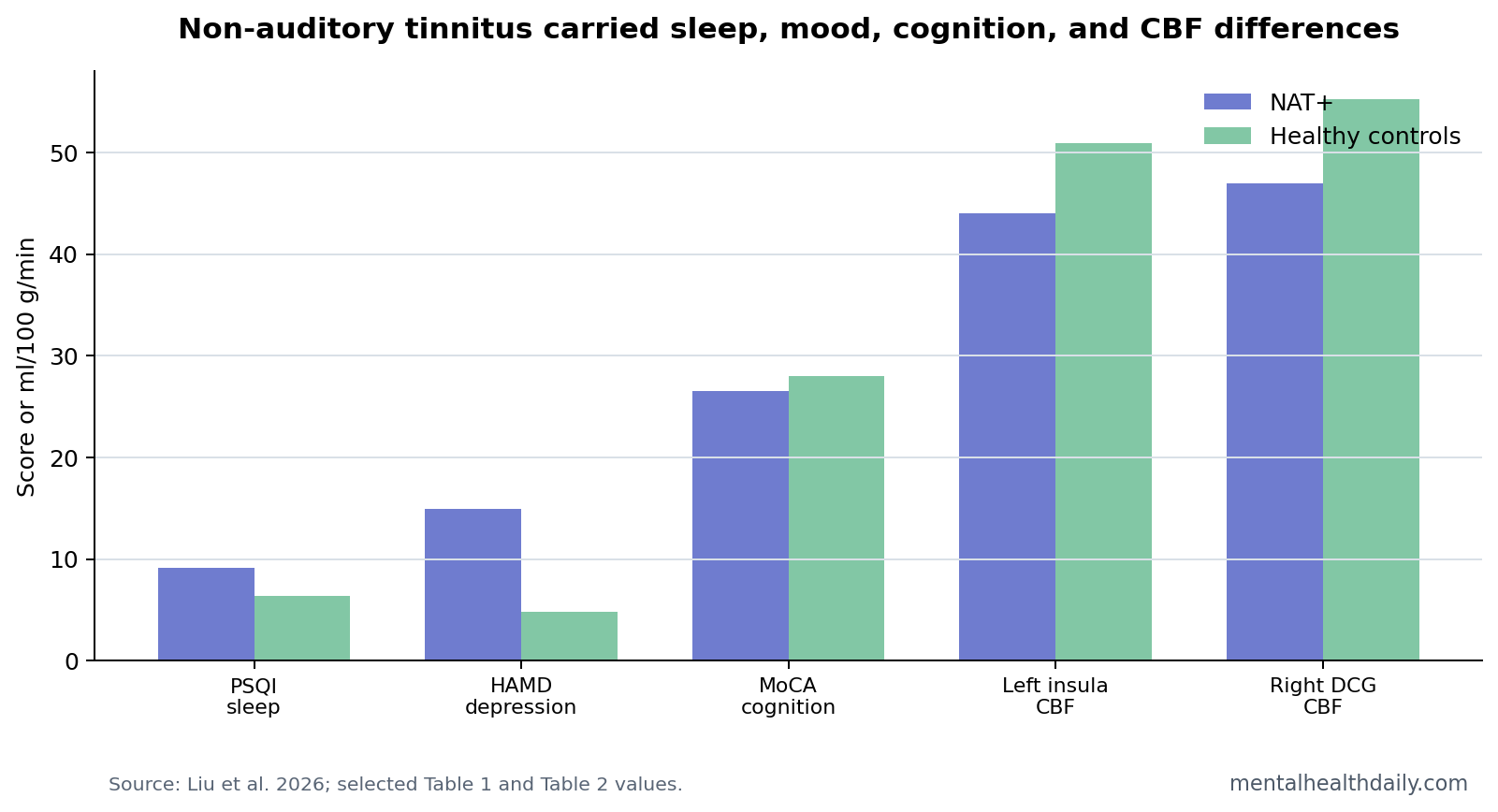
- Sleep quality was poorer with tinnitus: Pittsburgh Sleep Quality Index scores averaged 9.09 in the tinnitus group vs. 6.06 and 6.37 in the comparison groups, p = 0.004.1
- Depression scores were higher: HAMD scores averaged 14.96 in the tinnitus group vs. 11.20 and 4.85, p < 0.001.1
- Cognition was modestly lower: MoCA scores averaged 26.48 with tinnitus vs. 27.27 and 27.97, p = 0.022.1
- Perfusion tracked symptoms: Right middle cingulate blood flow correlated with sleep quality at r = −0.394, p = 0.021.1
Non-auditory tinnitus means tinnitus-like perception without a standard auditory cause such as hearing loss or primary ear pathology. In this paper, the relevant vascular context was cerebral venous congestion, a state in which internal jugular venous stenosis or transverse sinus stenosis can impair venous outflow from the brain.
Arterial spin labeling (ASL) is an MRI method that magnetically labels blood water and estimates cerebral blood flow without injected contrast. Liu et al. used multi-delay pseudo-continuous ASL to adjust for arterial transit time, which is important when venous outflow problems might distort timing-sensitive perfusion measures.
NAT+ Patients Had Lower Blood Flow Across 18 Regions
The main imaging result was not a single tinnitus spot. Corrected cerebral blood flow was lower in a broad set of regions in the non-auditory tinnitus group, including the inferior frontal gyrus, supplementary motor area, olfactory cortex, middle cingulate, insula, precentral and postcentral gyri, paracentral lobule, cerebellar regions, pregenual anterior cingulate cortex, and locus coeruleus.1
Several differences were large enough to be clinically interpretable. Left insula blood flow averaged 43.97 ml/100 g/min in the tinnitus group vs. 50.95 in controls, FDR-corrected p = 0.017. Left cerebellar hemisphere VIII averaged 28.37 vs. 35.35, p = 0.017. Right middle cingulate averaged 46.98 vs. 55.25, p = 0.030.
Sleep, Depression, and Cognition Were Part of the Same Clinical Pattern
In this sample, non-auditory tinnitus appeared with a broader symptom pattern than sound perception alone. The tinnitus group had poorer sleep quality, higher anxiety and depression ratings, and lower memory/cognition scores than healthy controls. The PSQI difference was especially clear: 9.09 in NAT+ patients vs. 6.06 in NAT- patients and 6.37 in healthy controls.
Reader translation: a PSQI around 9 usually reflects clinically meaningful sleep disturbance. The result does not prove that venous congestion caused insomnia or depression. It shows that the tinnitus-plus-venous-congestion group carried a broader brain-health symptom load.
Perfusion Correlations Pointed to Sleep and Mood Circuits
Within the tinnitus group, corrected blood flow in the right middle cingulate correlated negatively with PSQI scores, r = −0.394, p = 0.021. Right pregenual anterior cingulate blood flow showed a similar relationship with PSQI, r = −0.411, p = 0.016.1
The cingulate and insula are not “tinnitus centers.” They are salience, autonomic, affective, and interoceptive regions. Lower perfusion in those regions fits a model in which venous outflow problems may interact with arousal, sleep disruption, mood symptoms, and cognitive fatigue.
This Supports a Vascular-Brain Subtype, Not a Universal Tinnitus Theory
Evidence-strength note: the study was cross-sectional. It cannot show that venous congestion caused tinnitus, that reduced blood flow caused sleep disturbance, or that treating venous stenosis would reverse the MRI pattern. It also does not generalize to ordinary auditory tinnitus without venous pathology.
Adjacent tinnitus imaging work has reported regional blood-flow and metabolic changes in chronic tinnitus.3 Venous stenosis and pulsatile-tinnitus studies make the vascular angle plausible in selected patients.2 Liu et al. add a more specific point: in non-auditory tinnitus with venous congestion, perfusion abnormalities were tied to sleep, depression, and cognition rather than hearing thresholds alone.
Venous Congestion Changes the Interpretation of ASL
ASL is usually described as an arterial perfusion method because it labels inflowing arterial blood. Venous congestion complicates that simple description. If venous outflow is restricted, arterial inflow, capillary transit, venous pressure, and tissue oxygen delivery can all shift. Multi-delay ASL helps because it samples multiple post-labeling times and adjusts for arterial transit time.
Reader translation: the scan is not directly photographing blocked veins. It is estimating how much blood reaches brain tissue under conditions where venous drainage may be abnormal. That makes the vascular interpretation plausible, but it also means ASL should be paired with venous imaging and clinical examination rather than read in isolation.
The affected regions also matter. Cingulate and insula findings fit symptom regulation better than a simple ear-noise model. Motor, paracentral, cerebellar, and locus coeruleus differences point toward arousal, sensorimotor integration, and autonomic regulation. Olfactory cortex findings are harder to interpret, but they reinforce that the perfusion pattern was not limited to primary auditory cortex.
Sleep May Be a Clinical Bridge Between Perfusion and Tinnitus Burden
Sleep disturbance is one of the most actionable findings in the paper. The tinnitus group had PSQI scores averaging 9.09, and right cingulate blood-flow values correlated negatively with PSQI scores. That pattern does not prove causality, but it gives clinicians a practical target: sleep quality can be measured and treated even before vascular mechanisms are fully settled.
Sleep-arousal pathway: tinnitus can increase vigilance, fragmented sleep can amplify tinnitus salience, and poor sleep can worsen mood and attention. Venous congestion may add another physiological stressor by altering perfusion or pressure dynamics. These pathways can reinforce one another without requiring one single first cause.
That is why the cognitive and depression findings should not be dismissed as unrelated symptoms. Lower MoCA and memory scores may partly reflect sleep disruption, mood burden, vascular physiology, or attentional capture by tinnitus. The study cannot apportion those causes, but it shows they traveled together in the NAT+ group.
Who Should Be Considered for Vascular Workup?
This paper does not support vascular imaging for every person with ringing in the ears. It supports a more selective question: does the symptom pattern fit a non-auditory or venous-congestion phenotype?
- Higher-yield clues: non-pulsatile tinnitus without hearing loss, headache, visual symptoms, pressure-like sensations, known jugular or transverse sinus stenosis, or symptoms that vary with posture.
- Lower-yield clues: classic noise-induced hearing loss, stable high-frequency tinnitus after acoustic injury, or isolated tinnitus with no vascular or neurological features.
- Clinical guardrail: imaging should be used to answer a specific diagnostic question, not to hunt for incidental venous variants.
The next evidence step is longitudinal: if venous outflow improves, do ASL perfusion patterns, sleep scores, and tinnitus severity improve together? That design would move the field beyond cross-sectional association.
The Imaging Result Should Change Questions, Not Create a Diagnosis
The most defensible clinical use is question generation. A patient with non-auditory tinnitus and venous-congestion features may need a more integrated review of sleep, mood, cognition, headache, vision symptoms, venous anatomy, and medication exposure. The MRI result should not become a new diagnostic label by itself.
Measurement caution: ASL values can be affected by scanner protocol, arterial transit time, motion, vascular anatomy, caffeine, sleep deprivation, and physiological state on the scan day. The study adjusted for arterial transit time, but routine clinical interpretation would still need consistent acquisition and comparison standards.
The depression and anxiety scores also need careful language. NAT+ and NAT- patients both had higher mood and anxiety ratings than healthy controls, while the tinnitus group had the heavier sleep and cognitive pattern. That supports a broad venous-congestion symptom burden, with tinnitus marking a subgroup rather than a completely separate disorder.
A practical follow-up study should collect scan-day sleep, caffeine, medication, headache, venous-pressure markers, and tinnitus loudness in the same protocol. Without those paired measures, a perfusion map can look more mechanistic than it really is. The value of Liu et al. is that it points to the right integrated measurement set.
That integrated approach is also more patient-facing: tinnitus severity, sleep disruption, mood symptoms, and cognitive fatigue are experienced together, even when research papers analyze them separately.
That is also the main clinical restraint: vascular imaging should sharpen a specific differential diagnosis, not turn every tinnitus complaint into a perfusion disorder.
Questions About Non-Auditory Tinnitus and Blood Flow
Is this the same as common tinnitus after hearing loss?
No. The study focused on non-auditory tinnitus in patients with venous congestion. It should not be used as a universal explanation for all tinnitus.
Does lower blood flow mean brain damage?
Not necessarily. ASL measured perfusion differences, not tissue loss. Lower corrected cerebral blood flow may reflect vascular outflow, arousal state, or compensatory physiology.
Should tinnitus patients be screened for venous congestion?
The paper supports vascular evaluation when symptoms fit a venous or non-auditory pattern. It does not justify blanket venous imaging for every tinnitus complaint.
References
- Liu Y, et al. Cerebral blood flow alterations in non-auditory tinnitus: implications for the pathophysiology of cerebral venous congestion. Brain Imaging and Behavior. 2026. doi:10.1007/s11682-026-01144-8
- Venous stenosis and pulsatile tinnitus perfusion studies. PubMed
- Arterial spin labeling studies in chronic tinnitus. PubMed
- Sleep disturbance and tinnitus research. PubMed