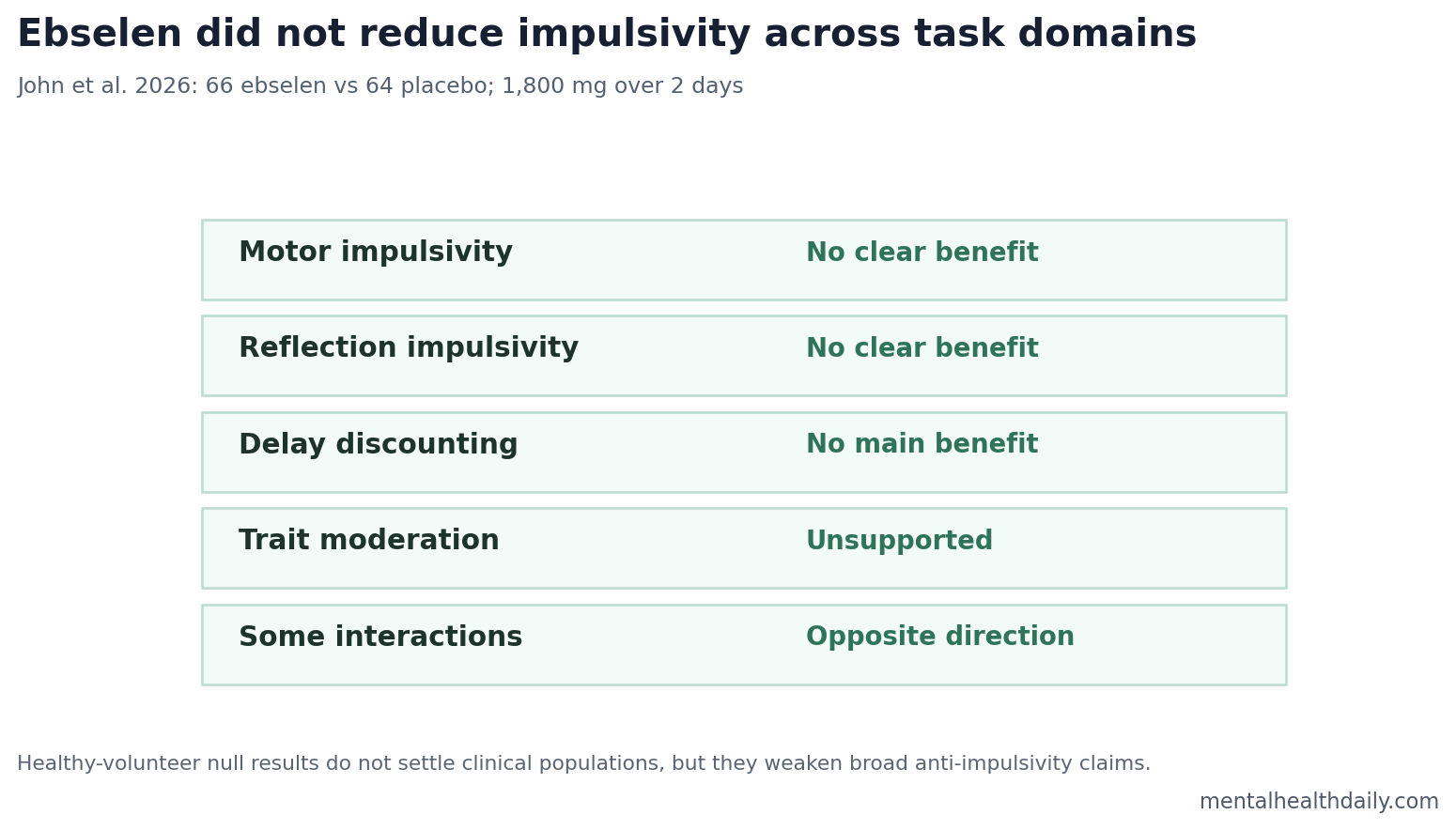
A double-blind placebo-controlled trial found no evidence that ebselen reduced impulsivity in 130 healthy adults: 66 received ebselen, 64 received placebo, and the 1,800 mg 2-day regimen did not improve motor impulsivity, reflection impulsivity, or delay discounting.1 The more interesting calibration is that several trait-impulsivity interactions ran opposite the secondary prediction, weakening the idea that ebselen is a general anti-impulsivity drug.
Research Highlights
- No main impulsivity benefit appeared: In 130 healthy adults, ebselen did not substantively reduce motor impulsivity, reflection impulsivity, or delay discounting vs. placebo.1
- The dose was pharmacologically serious: Participants received 1,800 mg over 2 days, a regimen selected from prior human ebselen work.1
- Trait moderation was unsupported: High-trait impulsive participants did not show convincing extra benefit compared with low-trait participants.1
- Some discounting interactions ran backward: Titrating Alternatives log k showed beta = 0.08, t(124) = 3.45, p = 0.001, opposite the expected benefit direction.1
- Clinical extrapolation is limited: The trial tested healthy adults for 2 days, not patients with bipolar disorder, mania, addiction, or severe impulsivity.1
Ebselen is a selenium-containing drug candidate studied partly because it can inhibit inositol monophosphatase, an enzyme in the phosphoinositide pathway. Lithium also affects this pathway, which is why ebselen has attracted interest as a possible lithium-like compound.
Impulsivity is not one thing. Motor impulsivity means acting before stopping; reflection impulsivity means deciding with too little evidence; delay discounting means preferring smaller immediate rewards over larger delayed rewards. A drug can plausibly affect one domain and miss another.
130 Healthy Adults Tested a Short Ebselen Regimen
John et al. randomized healthy adults to ebselen or placebo. The final analysis included 130 participants: 66 in the ebselen group and 64 in the placebo group. The regimen delivered 1,800 mg over 2 days.1
The design matters because it tests acute human pharmacology, not long-term treatment. A negative healthy-volunteer task result does not prove ebselen would fail in mania, bipolar disorder, or substance-use disorders. It does show that a simple laboratory anti-impulsivity claim did not survive this test.
Earlier work made the trial plausible. Singh et al. reported that ebselen inhibited inositol monophosphatase and produced lithium-like biology in preclinical systems.2 Human pharmacology studies also suggested central effects, but central activity is not the same as clinical symptom improvement.3
Motor, Reflection, and Choice Impulsivity Did Not Improve
The trial’s main result was broad non-support across the impulsivity battery. Ebselen did not produce substantive improvements in motor impulsivity, reflection impulsivity, or delay discounting vs. placebo.1
Delay discounting measures how steeply a person devalues a reward when it is delayed. Steeper discounting generally means a stronger pull toward immediate reward. In theory, a drug that reduces impulsive choice should flatten discounting.
Reflection impulsivity measures how much evidence someone gathers before deciding. A person can be impulsive in action but not in evidence gathering, or impulsive in reward choice but not in stopping behavior. That multidimensional structure is one reason broad anti-impulsivity claims are hard to prove.4
Trait-Impulsivity Moderation Did Not Rescue the Drug Signal
The secondary idea was that ebselen might help people who started out more impulsive. That is clinically sensible as a hypothesis because a ceiling effect can hide benefits in low-symptom healthy volunteers.
The moderation analysis did not provide convincing support. High-trait impulsive participants did not show a clean extra benefit across the task battery. Some delay-discounting interactions moved opposite the predicted benefit direction: Titrating Alternatives log k, beta = 0.08, t(124) = 3.45, p = 0.001; AUC, beta = −0.02, t(124) = −2.49, p = 0.01; and MCQ, beta = 0.11, t(125) = 1.99, p = 0.05.1
The practical read is not that ebselen worsens impulsivity in general. It is narrower: the study did not show the predicted trait-selected improvement, and the few interaction signals are not a clean therapeutic pattern.
Lithium-Like Mechanism Did Not Translate Into a Broad Task Benefit
The ebselen story is a useful warning about mechanism-to-outcome leaps. Inhibiting an enzyme in a lithium-relevant pathway can be biologically interesting while still failing to improve a laboratory outcome.
That distinction is especially important for impulsivity because task endpoints split apart. A drug that affects mood instability, mania risk, or neural excitability might not immediately change delay discounting in healthy volunteers. The reverse is also possible: a drug can move a laboratory task without becoming a useful psychiatric treatment.
Supported: this trial weakens a broad claim that short-course ebselen reduces impulsivity in healthy adults.
Not supported: a definitive failure in bipolar disorder, addiction, mania, or clinically selected high-impulsivity groups. Those populations would need separate randomized trials with symptom-relevant endpoints.
Healthy-Volunteer Results Narrow the Ebselen Claim
The trial is still informative because healthy-volunteer pharmacology is where broad cognitive claims should be easiest to detect under controlled conditions. Participants can be randomized, dosed, tested, and compared without active mania, intoxication, withdrawal, acute mood episodes, or major medication changes driving the result.
What narrowed: the claim that ebselen acutely reduces general impulsivity across laboratory domains. The study tested several impulsivity constructs and did not find a coherent benefit pattern. That makes future ebselen claims more specific by necessity: they need a clinical population, a dosing schedule, and an endpoint that matches the proposed mechanism.
What remains open: ebselen could still have effects on mood instability, oxidative stress, inositol signaling, or clinical symptoms in selected disorders. Those possibilities require patient trials. The current trial mainly blocks the shortcut from lithium-like enzyme effect to broad anti-impulsivity effect.
Delay Discounting Interactions Require Directional Caution
The delay-discounting interaction results are the part that prevents a soft “maybe it helps the right people” reading. In several models, higher trait impulsivity did not reveal the predicted ebselen benefit. Titrating Alternatives log k moved with beta = 0.08, t(124) = 3.45, p = 0.001, while AUC moved with beta = −0.02, t(124) = −2.49, p = 0.01.1
Those statistics should not be converted into a clinical harm claim. They do, however, make the moderation story weaker. A trait-selected benefit should show a consistent directional pattern across tasks or at least a biologically coherent split. This trial did not produce that pattern.
The next ebselen trial should choose one clinical target instead of a broad task battery. For example, mania relapse, stimulant-use craving, or aggression would each require different timing, outcomes, and safety monitoring. A mechanism can be shared while the clinical test remains indication-specific.
Endpoint selection is the major lesson. If the target is bipolar disorder, mood instability and relapse prevention may be more relevant than a one-session discounting task. If the target is addiction, craving, relapse, or drug choice under stress may be more relevant. If the target is aggression, response inhibition under provocation may be closer to the clinical problem.
The John trial keeps those future designs honest. It says a short ebselen course did not shift a broad impulsivity battery in healthy adults, so the next study needs a sharper population and a sharper endpoint. A weaker version of the same healthy-volunteer claim would be a low-value repeat.
Safety and tolerability also belong in the next design. A drug proposed as a lithium-like alternative has to show more than a mechanistic resemblance; it has to show that the expected benefit justifies exposure, monitoring, and interaction risk in the population being treated. That standard is especially important when the proposed outcome is behavioral control rather than a laboratory biomarker.
For now, the evidence supports restraint. Ebselen remains a biologically interesting compound, but the anti-impulsivity claim needs clinical specificity before it becomes useful.
That specificity should include whether the target behavior is impulsive action, impulsive choice, emotional urgency, relapse under craving, or risky decision-making during mood elevation. Those are related constructs, but they are not interchangeable endpoints.
Each endpoint needs its own trial logic.
Patient selection would also need to be tighter than a broad "high impulsivity" label. A bipolar-disorder trial might enrich for recent manic symptoms or relapse risk, while an addiction trial might enrich for cue-induced craving or early abstinence. Those groups could plausibly have different inositol-signaling, oxidative-stress, sleep, and medication backgrounds. Treating them as one impulsivity population would blur the same domain distinctions that made the healthy-volunteer result hard to rescue.
Dosing duration is another open design choice. A 2-day exposure can test acute task effects, but mood stabilization, relapse prevention, and behavioral control may require longer treatment windows with repeated symptom measurement.
Questions About Ebselen and Impulsivity
Does this mean ebselen has no psychiatric potential?
No. It means this 2-day healthy-volunteer trial did not show a broad anti-impulsivity effect. Other indications would need direct testing.
Why test healthy adults?
Healthy-volunteer pharmacology can detect acute cognitive or behavioral effects under controlled conditions. Patient trials remain necessary for clinical indications.
Was the trial completely null?
The main therapeutic claim was unsupported. Some moderation interactions were statistically notable, but they did not form a clean benefit pattern and some moved opposite the prediction.
Should people use ebselen for impulsivity?
No clinical use follows from this paper. The study does not support ebselen as an anti-impulsivity treatment.
References
- John A, et al. No evidence of moderated impulsivity following ebselen in healthy volunteers. Human Psychopharmacology. 2026. doi:10.1002/hup.70040
- Singh N, Halliday AC, Thomas JM, et al. A safe lithium mimetic for bipolar disorder. Nature Communications. 2013. doi:10.1038/ncomms2337
- Masaki C, Sharpley AL, Cooper CM, et al. Effects of the potential lithium-mimetic ebselen on emotional processing and reward seeking. Neuropsychopharmacology. 2016. doi:10.1038/npp.2015.356
- Pattij T, Vanderschuren LJMJ. The neuropharmacology of impulsive behaviour. European Journal of Pharmacology. 2008. doi:10.1016/j.ejphar.2008.06.095