A 2026 pilot randomized trial involving 36 older U.S. veterans with PTSD symptoms found that a structured social-function group therapy produced stronger signals for romantic and family functioning than a support group, with condition-by-time effects of eta-squared = 0.072 and eta-squared = 0.112. The same trial did not show a specific advantage for friendships and socializing, where both groups appeared to improve and the condition-by-time effect was near zero at eta-squared = 0.009.
Research Highlights
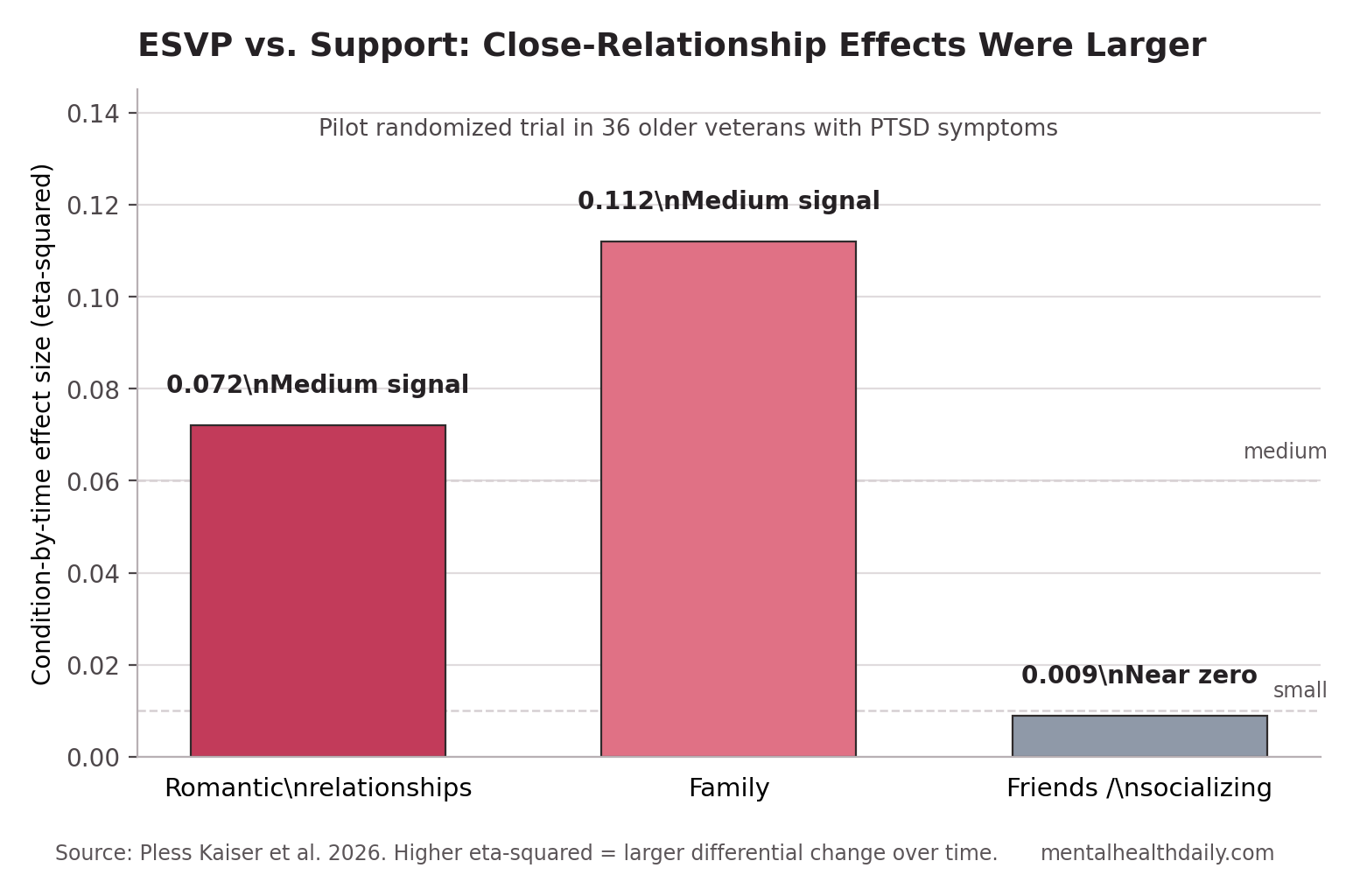
- Close relationships carried the signal: ESVP showed medium condition-by-time effects for romantic relationship impairment (eta-squared = 0.072) and family impairment (eta-squared = 0.112).
- Socializing was not ESVP-specific: Friends and socializing improved over time, but the intervention-vs.-support interaction was eta-squared = 0.009.
- Enrollment was possible but labor-intensive: Researchers attempted to contact 270 veterans, assessed 117 for eligibility, found 74 eligible, and randomized 36.
- Engagement looked similar across groups: Veterans attended 6.56 ESVP sessions vs. 5.62 support sessions on average, and 72% vs. 69% attended at least 5 of 9 sessions.
- Evidence strength is preliminary: The trial analyzed 34 participants after 2 pre-session support dropouts, had baseline imbalances, and was not powered as a definitive efficacy study.
Enhancing Social Function for Older Veterans with PTSD (ESVP) is a 9-session group intervention designed to make social functioning a direct treatment target rather than a hoped-for side benefit of PTSD care. Sessions covered interpersonal relationships, communication, anger management, social support and activities, stress management, and final review, with practice assignments between meetings.
Social function means the practical ability to maintain relationships, participate in social activities, communicate, manage conflict, and feel connected rather than isolated. In PTSD, social function can be damaged by avoidance, irritability, emotional numbing, mistrust, shame, and trauma-linked withdrawal; in later life, retirement, bereavement, physical limitations, and shrinking routines can make those problems harder to compensate for.
ESVP Was Built for Relationship Skills, Not PTSD Symptom Exposure
Pless Kaiser et al. tested ESVP against a support-group comparison condition, not against no treatment. That choice matters because the comparator also gave veterans 9 group sessions, discussion time, peer contact, and take-home work.
ESVP content: structured education, worksheets, role play, group discussion, and homework focused on relationships, communication, anger management, social support, activities, and stress management.
Support content: a present-focused group check-in where members raised current issues, shared experiences, received feedback, and completed simple between-session homework about what went well and what felt difficult.
The design therefore asked a sharper question than “is group contact useful?” It asked whether structured social-function skills added anything beyond supportive peer discussion for older veterans with military-related trauma and PTSD symptoms.
36 Veterans Were Randomized After a Large Recruitment Screen
Recruitment required a large funnel. The study team attempted to contact 270 veterans by phone or mail. Of the 160 reached by telephone, 43 were not interested, and 117 were assessed for eligibility.
Eligibility required U.S. military veteran status, age 60 years or older, military-related trauma, and PTSD symptoms across DSM-5-TR symptom clusters. Exclusions included current individual PTSD treatment, psychosis, dementia or severe cognitive disorder, and recent hospitalization for suicidal ideation or psychosis.
The final randomized sample included 36 veterans: 18 assigned to ESVP and 18 assigned to support. Two veterans assigned to support could not be reached before sessions began and were treated as pre-intervention dropouts, leaving 34 participants in the intervention analyses.
Sample profile: Participants ranged from 61 to 85 years old, with a mean age of 71.62 years. Most were male (94%), White (85%), and partnered (62%). By structured interview, 19 of 34 participants (56%) met current PTSD criteria, and 31 (91%) met lifetime PTSD criteria.
Baseline social concerns fit the intervention target. Veterans most often endorsed difficulty sharing thoughts and feelings, being patient, settling arguments, and engaging in social support or social activities.
Engagement Was Similar in ESVP and Support Groups
Attendance looked feasible for both arms. Veterans assigned to ESVP attended an average of 6.56 sessions, SD = 3.00, and 13 of 18 (72%) attended at least 5 of 9 sessions. Veterans assigned to support attended 5.62 sessions, SD = 3.50, and 11 of 16 post-randomization starters (69%) attended at least 5 sessions.
The mean attendance difference was not statistically significant, t = 0.83, p = 0.414. Six-month follow-up participation was modest but similar: 11 ESVP participants (61%) attended the follow-up session and 13 (72%) completed measures, compared with 9 support participants (56%) attending and 11 (69%) completing measures.
Acceptability: Relevance and satisfaction ratings were high and did not significantly differ between ESVP and support. ESVP participants gave especially strong content-understanding ratings: 95% of ratings described the content as “very” understandable, and 67% said discussions helped them understand their own experiences “very” well.
ESVP also separated from support on immediate post-session state and skill use. Participants in ESVP reported lower anger, lower distress, a greater sense of doing better than the prior session, and more frequent coping and anger-management skill use.
Close-Relationship Outcomes Favored the Structured Group
The main social-function outcome was the Inventory of Psychosocial Functioning (IPF), a PTSD-related functioning scale where higher scores mean worse impairment. Researchers focused on romantic relationships, family, and friendships/socializing because work, education, and some other subscales were less relevant for older adults.
Romantic relationship impairment showed a medium condition-by-time signal, eta-squared = 0.072. ESVP participants improved from baseline to post-intervention, t = 3.39, p = 0.003, and did not show a significant rebound by 6 months, t = 0.41, p = 0.690. Support participants also improved immediately after treatment, t = 2.75, p = 0.015, but their scores rebounded by 6 months, t = 2.80, p = 0.013, leaving no significant baseline-to-6-month change.
Family-function impairment showed a medium condition-by-time effect too: eta-squared = 0.112. ESVP participants improved from baseline to post-intervention, t = 3.16, p = 0.006, without significant rebound at 6 months. Support participants did not show significant family-function improvement from baseline to post-intervention, t = 0.63, p = 0.538.
The most plausible clinical read is domain-specific: structured communication, anger-management, and relationship-practice content may matter most inside close relationships, where repeated conflict patterns and avoidance loops have fewer places to hide.
Friendships and Socializing Improved Without a Specific ESVP Advantage
Friendships and socializing did not show an ESVP-specific effect. The condition-by-time interaction was eta-squared = 0.009, while the time effect was larger, eta-squared = 0.131.
That pattern is useful rather than disappointing. A support group can itself be a social intervention: participants meet peers, talk about current problems, receive feedback, and have a weekly setting for connection. For veterans whose main problem is low social contact, the act of attending a supportive group may be part of the treatment.
Older-adult social-connection trials point in the same direction. Conwell et al. tested peer companionship for older primary-care patients, and Van Orden et al. piloted Engage Psychotherapy to increase social connection and reduce later-life suicide risk. Neither intervention was PTSD-specific, but both treat social contact and social goal-setting as modifiable health targets rather than soft lifestyle extras.
Holt-Lunstad et al. made the broader stakes harder to dismiss in a 2010 meta-analysis: stronger social relationships were associated with roughly 50% greater odds of survival. A small PTSD group trial cannot prove mortality benefit, but social function belongs in the health-outcome column rather than the satisfaction-score column.
Pilot Design Limits the Strength of the Claim
This was a pilot trial, so the evidence-strength note has to be explicit. The design can show feasibility, acceptability, retention patterns, plausible outcome domains, and preliminary effect-size signals. It cannot prove that ESVP is an established PTSD treatment or that it would outperform support groups in a larger, more diverse veteran sample.
Several limitations narrow the claim:
- Small sample: 36 randomized veterans and 34 analyzed participants leave unstable estimates.
- Baseline imbalance: Support participants had higher PTSD symptom severity, while ESVP participants had greater romantic-relationship impairment at baseline.
- Limited diversity: Participants were mostly older, White, male veterans, so generalizability is limited.
- COVID-era delivery shift: The first cohort was in person, while later cohorts transitioned to telehealth.
- No multiple-comparison correction: The study emphasized pilot effect sizes rather than definitive hypothesis testing.
Active comparison also cuts both ways. Support groups may have made ESVP harder to beat, especially for general socializing, but that same comparator makes the close-relationship signal more interesting than a waitlist comparison would have been.
Where ESVP Fits in PTSD Care
ESVP should be read as a possible adjunct for older veterans whose PTSD is entangled with isolation, conflict, avoidance, or shrinking social roles. Trauma-focused psychotherapy, medication management, crisis care, substance-use treatment, and dementia evaluation remain the higher-priority lanes when those are the active problems.
Existing PTSD treatments already improve functioning for some patients. Beidel et al. tested a multicomponent behavioral treatment for chronic combat-related PTSD, and Thorp et al. compared prolonged exposure with relaxation training in older veterans. ESVP sits beside that literature by making relationship repair and social engagement the direct target.
The practical selection question is concrete:
- Close-relationship impairment: ESVP looks most relevant when romantic or family conflict, avoidance, irritability, or communication breakdown is central.
- Friendship/socializing isolation: A structured social group may help, but a support group, peer-companion program, or social-goal intervention may provide similar first-line social contact.
- Severe PTSD, psychosis, dementia, or acute suicidality: Those presentations need higher-intensity assessment and safety planning before a group social-skills intervention is treated as the main answer.
Questions About PTSD Social Function Therapy for Older Veterans
Did ESVP reduce PTSD symptoms?
This trial focused on social function, feasibility, and acceptability rather than proving PTSD symptom reduction. PTSD symptoms were part of eligibility and baseline characterization, but the headline outcome was relationship functioning on the IPF.
Was the support group a weak comparison?
No. Support participants had 9 sessions, peer contact, agenda-setting, discussion, feedback, and take-home work. That makes the friendship/socializing result easier to interpret: general group contact may itself be therapeutic for some social-function outcomes.
Who might benefit most from ESVP?
The pilot data point most strongly toward older veterans whose PTSD-related functioning problems sit inside close relationships: family conflict, romantic strain, anger, avoidance, communication breakdown, or difficulty sharing thoughts and feelings.
What would a stronger trial need?
A larger trial would need more diverse participants, clearer baseline social-function thresholds, stronger missing-data handling, fidelity checks, and enough power to test close relationships, friendship/socializing, loneliness, belongingness, and PTSD symptoms without treating every exploratory signal as decisive.
Bottom line: ESVP is best understood as promising social-function therapy for older veterans with PTSD, especially when close relationships are the main impairment. The 2026 pilot supports feasibility and a close-relationship signal, while friendship/socializing gains may come from structured ESVP or from the simpler act of joining a supportive peer group.
References
- Pless Kaiser A, Ream M, Spiro A, Sloan DM, Cook JM, Vogt D, Moye JA. Feasibility, acceptability, and outcomes: A pilot trial of the Enhancing Social Function in Older Veterans with PTSD (ESVP) group intervention. Psychological Services. 2026;23(2):293-306. doi:10.1037/ser0000962
- Holt-Lunstad J, Smith TB, Layton JB. Social relationships and mortality risk: A meta-analytic review. PLoS Medicine. 2010;7(7):e1000316. doi:10.1371/journal.pmed.1000316
- Conwell Y, Van Orden KA, Stone DM, McIntosh WL, Messing S, Rowe J, et al. Peer companionship for mental health of older adults in primary care: A pragmatic, nonblinded, parallel-group, randomized controlled trial. American Journal of Geriatric Psychiatry. 2021;29(8):748-757. doi:10.1016/j.jagp.2020.05.021
- Van Orden KA, Arean PA, Conwell Y. A pilot randomized trial of Engage Psychotherapy to increase social connection and reduce suicide risk in later life. American Journal of Geriatric Psychiatry. 2021;29(8):789-800. doi:10.1016/j.jagp.2021.03.009
- Beidel DC, Frueh BC, Uhde TW, Wong N, Mentrikoski JM. Multicomponent behavioral treatment for chronic combat-related posttraumatic stress disorder: A randomized controlled trial. Journal of Anxiety Disorders. 2011;25(2):224-231. doi:10.1016/j.janxdis.2010.09.006
- Thorp SR, Glassman LH, Wells SY, Walter KH, Gebhardt H, Twamley E, et al. A randomized controlled trial of prolonged exposure therapy versus relaxation training for older veterans with military-related PTSD. Journal of Anxiety Disorders. 2019;64:45-54. doi:10.1016/j.janxdis.2019.02.003