A 259-person multiple system atrophy survey found diagnosed neurogenic orthostatic hypotension in 41.7% of respondents, while another 40.0% had upright symptoms suspicious for nOH without a diagnosis and 21.2% reported never having upright blood pressure measured.1 The operational problem is simple: in MSA, low blood pressure on standing can be disabling, missed, and still undertreated after it is recognized.
Research Highlights
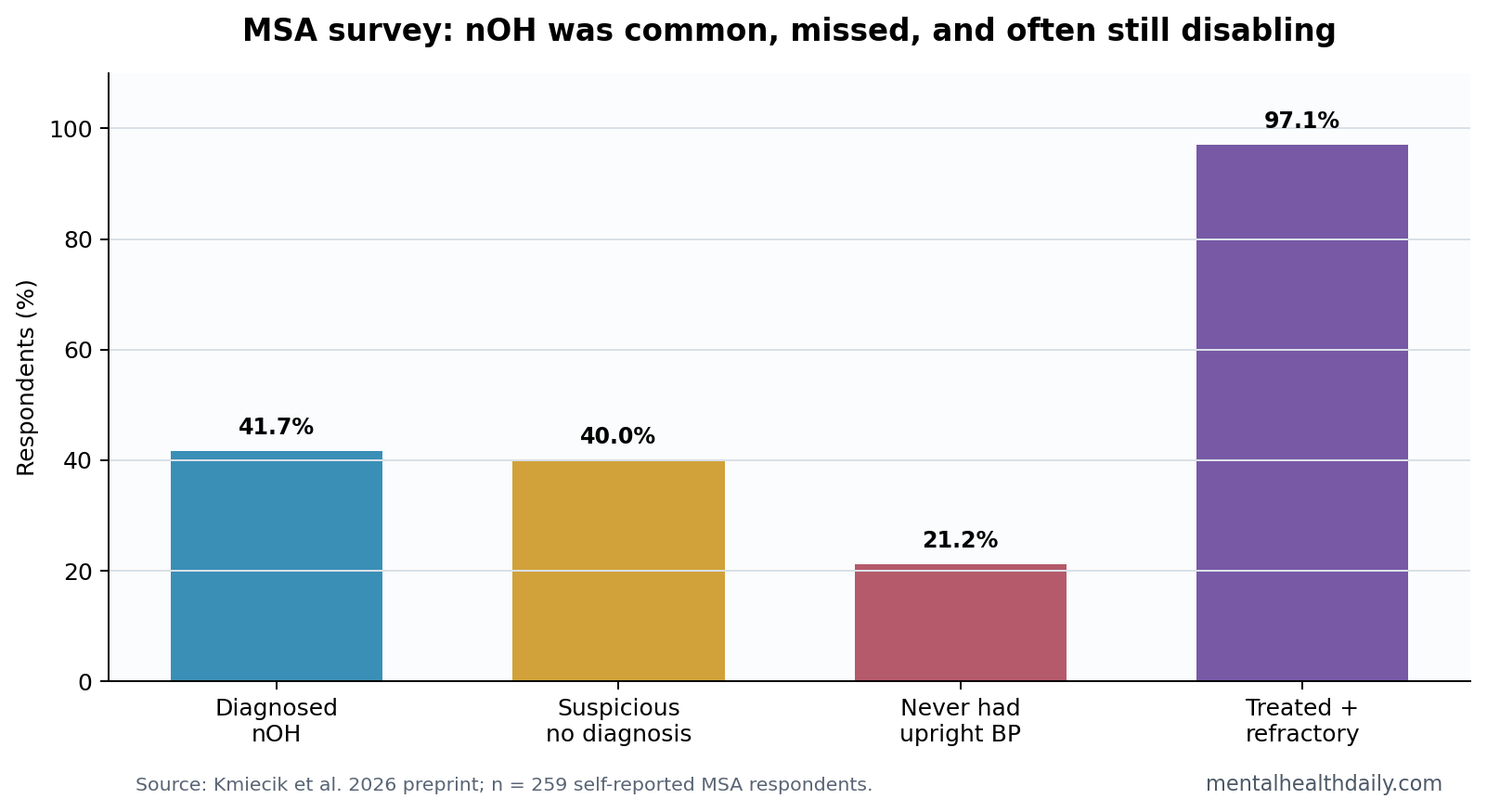
- Diagnosed nOH was common: Among 259 self-reported MSA respondents, 41.7% reported a neurogenic orthostatic hypotension diagnosis.1
- Possible missed nOH was also common: Another 40.0% had upright symptoms suspicious for nOH despite no diagnosis.1
- Screening gaps were visible: 21.2% of MSA respondents reported never having their blood pressure measured while upright.1
- Symptoms tracked function: nOH symptom count correlated with daily functional burden, r = 0.47, 95% CI 0.35 to 0.57, p = 2.80 x 10-12.1
- Treatment did not erase burden: Among treated respondents, 97.1% still reported refractory functional limitations from nOH symptoms.1
Multiple system atrophy (MSA) is a rare, progressive neurodegenerative disorder that affects movement and autonomic body functions. Neurogenic orthostatic hypotension (nOH) means blood pressure drops on standing because the nervous system does not regulate vascular tone properly.
nOH can cause dizziness, fatigue, visual dimming, falls, cognitive clouding, and fainting. In MSA, those symptoms can overlap with parkinsonism, cerebellar symptoms, urinary dysfunction, sleep disruption, and general disability, which makes active upright blood-pressure measurement essential.
41.7% Had Diagnosed nOH, and 40.0% Looked Undiagnosed
Kmiecik et al. analyzed 259 respondents with self-reported MSA.1 Of those, 108 respondents, or 41.7%, reported a physician diagnosis of nOH plus upright symptoms. A separate group of 103 respondents, or 40.0%, had upright symptoms suspicious for nOH but no diagnosis.
Why the suspected group matters: dizziness or lightheadedness, fatigue, postural symptoms, and functional limitation can be interpreted as generic MSA progression unless clinicians measure blood pressure lying down and standing. The survey found that 21.2% of respondents had never had upright blood pressure measured.
The result does not prove that every suspicious case truly had nOH. It does show a screening failure mode: a patient can have classic upright symptoms and still never receive the basic measurement that would clarify whether blood pressure is part of the problem.
nOH Symptoms Correlated With Daily Functional Burden
Among respondents with diagnosed or suspected nOH, the number of nOH symptoms correlated with the number of daily activities limited by blood-pressure drops, r(198) = 0.47, 95% CI 0.35 to 0.57, p = 2.80 x 10-12.1
That correlation is moderate, not total. Background MSA severity still explained much of the functional burden. The useful interpretation is that nOH symptom burden adds a measurable layer of disability, while MSA itself remains the larger disease context.
- Screening target: ask about upright symptoms and measure supine-to-standing blood pressure.
- Function target: connect dizziness, fatigue, falls, and cognitive clouding to daily tasks.
- Treatment target: check whether symptoms remain limiting despite non-drug steps or medication.
Each Additional Symptom Raised BP-Medication Odds by 18%
The survey also linked symptom burden to treatment. Each additional nOH symptom increased the odds of taking blood-pressure medication by 18%, OR = 1.18, 95% CI 1.03 to 1.36, p = 0.021.1
A 6-symptom threshold maximized the Youden index for BP-medication classification, but sensitivity and specificity were modest. Youden index is a diagnostic-summary statistic that balances sensitivity and specificity; here, it did not make symptom count a clean treatment classifier.
The treatment gap was more striking than the classifier. Among respondents treated for nOH, 97.1% still reported refractory symptoms that interfered with at least 1 daily function. Treatment existed, but daily-life limitation often remained.
That refractory figure changes how follow-up should sound. Treatment status is only the starting point. Standing tolerance, meal-related symptoms, falls, near-syncope, and activity avoidance need to improve enough to matter. A patient can be treated and still be unable to shower safely, stand in a pharmacy line, or leave home without planning around collapse risk.
Upright Blood Pressure Is the Low-Tech Gate
Consensus statements for neurogenic orthostatic hypotension emphasize active screening because symptoms can be unreliable and patients may not report them unless asked.2 MSA adds urgency because autonomic failure is not an incidental comorbidity; it is part of the disease biology.
Evidence-strength note: this was a cross-sectional online survey using self-reported MSA diagnosis. It can show patient-reported burden, screening gaps, and treatment frustration. It cannot establish clinician-confirmed prevalence or prove that all suspected cases had nOH.
The practical standard is still stronger than the evidence limit. If an MSA patient has dizziness, fatigue, falls, cognitive fog, visual symptoms, or postural worsening, upright blood pressure is a basic clinical measurement rather than an advanced specialty test.
nOH Screening Has to Separate Symptoms From Background MSA
MSA creates an interpretation problem because many symptoms can come from several mechanisms at once. Fatigue may reflect sleep disruption, autonomic failure, depression, medication effects, or neurodegeneration. Falls may reflect parkinsonism, cerebellar imbalance, visual symptoms, or blood-pressure collapse.
Clinical sorting step: the question is not whether a symptom belongs only to nOH. The question is whether the symptom worsens upright, improves lying down, appears after meals, or travels with measurable blood-pressure drops.
That is why upright measurement is a low-tech but high-yield gate. A clinician does not need an expensive biomarker to learn whether standing blood pressure collapses. The measurement can be repeated at home or in clinic, and it can be interpreted alongside symptom timing.
Treatment Failure Should Not Be Read as Symptom Exaggeration
One of the survey’s most important numbers was the refractory-symptom rate. Among respondents treated for nOH, 97.1% still reported functional limitation. Treatment may still have helped, but it often did not restore normal standing tolerance.
- Non-drug steps: hydration, salt strategies, compression, meal timing, and head-up sleeping may help but can be hard to sustain.
- Drug treatment: pressor medications can raise standing pressure, but dosing, supine hypertension, and side effects limit use.
- Disease context: MSA progression can keep daily function limited even when blood pressure improves.
- Caregiver load: falls, fainting risk, and activity restriction can shift burden onto family support.
The practical implication is follow-up. A diagnosis and prescription do not close the loop. Patients need repeated assessment of upright symptoms, home readings when feasible, supine hypertension risk, falls, and which daily activities remain blocked.
Patient-Reported Data Are a Strength and a Limitation
The survey’s patient-reported design is not a flaw to dismiss. MSA patients and caregivers often know which symptoms block showering, stairs, meals, standing, leaving the house, and clinic travel better than a short office visit can capture. That is why patient-reported functional burden belongs in autonomic research.
The same design also limits prevalence claims. Self-reported diagnosis, web access, support-group recruitment, and symptom recall can enrich the sample for patients who are more engaged, more symptomatic, or more frustrated with care. The result should therefore be read as a burden and screening-gap signal rather than a precise population estimate.
Balanced read: even if the exact percentages shift in clinician-confirmed cohorts, the combination of high suspected nOH, missed upright BP measurement, and refractory symptoms is operationally important. Those are fixable process failures alongside biological disease mechanisms.
Better future studies would pair patient-reported symptoms with verified MSA subtype, medication list, supine and standing blood pressure, home readings, falls, caregiver burden, and treatment changes over time.
Clinic workflow should be just as concrete. A visit that documents gait, bladder symptoms, medications, falls, and caregiver burden but skips upright blood pressure can miss a treatable contributor to daily disability, especially when symptoms worsen after standing, meals, or exertion.
Screening has to be repeated because nOH can change with disease stage, hydration, food intake, medication timing, heat exposure, infection, and deconditioning. One normal reading should not end the search.
Serial readings improve interpretation.
A practical log should pair numbers with context: lying pressure, standing pressure, time since standing, meal timing, medication timing, dizziness, falls, visual dimming, cognitive clouding, and whether the patient had to sit or lie down. That kind of record does not prove autonomic failure by itself, but it makes the office visit less dependent on memory and exposes patterns that a single clinic reading can miss.
The 21.2% never-measured figure is therefore more than a documentation problem.1 In MSA, missed upright measurement can mean missed fall prevention, missed supine-hypertension counseling, missed medication adjustment, and missed caregiver planning.
Questions About MSA and Neurogenic Orthostatic Hypotension
What symptoms should raise suspicion for nOH in MSA?
Dizziness, lightheadedness, fatigue, visual dimming, fainting, falls, weakness, cognitive clouding, and symptoms that worsen upright or after meals should prompt orthostatic blood-pressure assessment.
Does home blood-pressure monitoring solve the problem?
It can help, especially when clinic readings miss variability. Patients still need clear instructions on timing, posture, supine hypertension risk, and when to report results.
Why can treated patients still be disabled by nOH?
MSA autonomic failure can be severe, medication options are limited, and raising standing blood pressure can create tradeoffs such as supine hypertension. Persistent symptoms after treatment are common enough to require active follow-up.
References
- Kmiecik J, et al. The burden of neurogenic orthostatic hypotension in patients with multiple system atrophy: a real-world study. medRxiv. 2026. doi:10.64898/2026.04.20.26351214
- Fanciulli A, et al. Consensus statement on the definition of neurogenic orthostatic hypotension in Parkinson’s disease and related disorders. Movement Disorders. 2018. doi:10.1002/mds.27421
- Palma JA, Kaufmann H. Management of orthostatic hypotension. Continuum. 2020. doi:10.1212/con.0000000000000816
- Low PA. Prevalence of orthostatic hypotension. Clinical Autonomic Research. 2008. doi:10.1007/s10286-007-1001-3